
Abstract
Abstract
Background:
Published studies on laparoscopic surgery for transverse colon cancer are scarce. More studies are necessary to evaluate the feasibility, safety, and long-term oncologic outcomes of laparoscopic surgery for transverse colon cancer.
Subjects and Methods:
From April 1996 to December 2010, 102 consecutive patients with stage II or III disease who had undergone curative resection for transverse colon cancer were enrolled. Seventy-nine patients underwent laparoscopy-assisted colectomy (LAC), whereas 23 patients underwent conventional open colectomy (OC). Short- and long-term outcomes of the two groups were compared.
Results:
The OC group had a larger tumor size (7.6 ± 3.4 cm versus 5.2 ± 2.3 cm, P = .004) and more retrieved lymph nodes (26.4 ± 11.6 versus 17.5 ± 9.4, P = .002), without differences in resection margins. In the LAC group, return to diet was faster (4.5 ± 1.2 days versus 5.4 ± 1.8 days, P = .013), and postoperative hospital stay was shorter (12.1 ± 4.2 days versus 15.9 ± 4.8 days, P = .000). There were no differences in occurrence of intra- or postoperative complications. There were no statistically significant differences in overall survival rate (OS) or disease-free survival rate (DFS) between the two groups (5-year OS, 90.4% versus 90.5%, P = .670; 5-year DFS, 84.2% versus 90.7%, P = .463).
Conclusions:
Laparoscopic surgery for transverse colon cancer has better short-term outcomes compared with open surgery, with acceptable long-term outcomes. As in colorectal cancer of other sites, laparoscopic surgery can be a feasible alternative to conventional surgery for transverse colon cancer.
Introduction
S
Previously mentioned studies, however, did not include transverse colon cancers. The reasons for excluding transverse colon cancer were that this type is less frequent than other colon cancers and that it is difficult to handle the middle colic vessels laparoscopically. In addition, there are not many published studies on laparoscopic surgery for transverse colon cancer,6–15 and most of them used a retrospective design and dealt with short-term outcomes. Thus, more evidence is needed regarding the safety and usefulness of laparoscopic surgery in transverse colon cancer.
The purpose of the present study was to determine whether laparoscopic surgery could be an alternative treatment to open surgery in transverse colon cancer. Data from St. Vincent Hospital (The Catholic University of Korea, Suwon, Korea) were analyzed retrospectively, and both short- and long-term outcomes were compared.
Subjects and Methods
Patients and measured outcomes
In our institution, the use of laparoscopic surgery for transverse colon cancer started in April 1996. From April 1996 to February 2009, surgery was performed on 194 patients with primary transverse colon cancer. After exclusion of patients who met certain exclusion criteria (Table 1), data from 102 patients of the original 194 were ultimately assessed. This study was approved by the Institutional Review Board of St. Vincent Hospital (study number VC14RISI0117). Transverse colon cancer was defined as cancer arising between the hepatic and splenic flexures. Of the enrolled 102 patients, 79 underwent laparoscopic-assisted colectomy (LAC), and 23 underwent open colectomy (OC).
Double primary malignancy refers to the diagnosis of another primary cancer (other than transverse colon cancer) that required treatment within 1 year of transverse colon cancer surgery.
Previous malignancy refers to a primary malignancy treated within 5 years prior to transverse colon cancer surgery.
The two groups were compared on the basis of intention to treat and were analyzed for the following: patient characteristics, operative results, postoperative recovery course, intra- and postoperative complications, pathologic characteristics for the oncologic quality of the resected specimen, and long-term oncologic outcomes. In this study, postoperative complications encompassed all complications caused by primary surgery within 30 days postoperatively.
Perioperative management
Preoperative colonoscopy and barium enema or abdominopelvic computed tomography (CT) were performed on all patients to accurately assess the cancer location. For the LAC group, preoperative colonoscopic tattooing and clipping were applied for every lesion that was suspected as T2 or less in previous imaging studies. Bowel preparation was performed, and intravenous antibiotics were administered prior to the operation. 5-Fluorouracil-based chemotherapy was administered according to postoperative pathology results and clinical judgment.
Postoperative follow-up
A follow-up assessment was conducted every 3 months within 2 years of surgery, biannually 2–5 years after surgery, and annually after more than 5 years postoperatively. The carcinoembryonic antigen level was checked at each follow-up visit. Abdominopelvic CT was performed biannually, and a colonoscopy was performed annually. Positron emission tomography or chest CT was performed according to clinical necessity. The last follow-up was performed in December 2013.
Surgical procedures
Surgical treatment was performed according to the cancer's location. Right hemicolectomy or extended right hemicolectomy was performed for lesions in the hepatic flexure as well as for lesions within the distal 10 cm of the hepatic flexure. Left hemicolectomy or extended left hemicolectomy was performed for lesions in the splenic flexure as well as for lesions within the proximal 10 cm of splenic flexure. Transverse colectomy or extended right hemicolectomy was performed for the lesions in between.
For right-sided lesions, not only the middle colic vessels but also the right colic vessels (if present) and ileocolic vessels were ligated and divided at their origins after skeletonizing the anterior and right lateral sides of the superior mesenteric vessels for thorough lymph node dissection. Dissection proceeded very carefully around the middle colic vein (MCV) to avoid damaging the thin veins in the diverse drainage system of the MCV (Fig. 1).
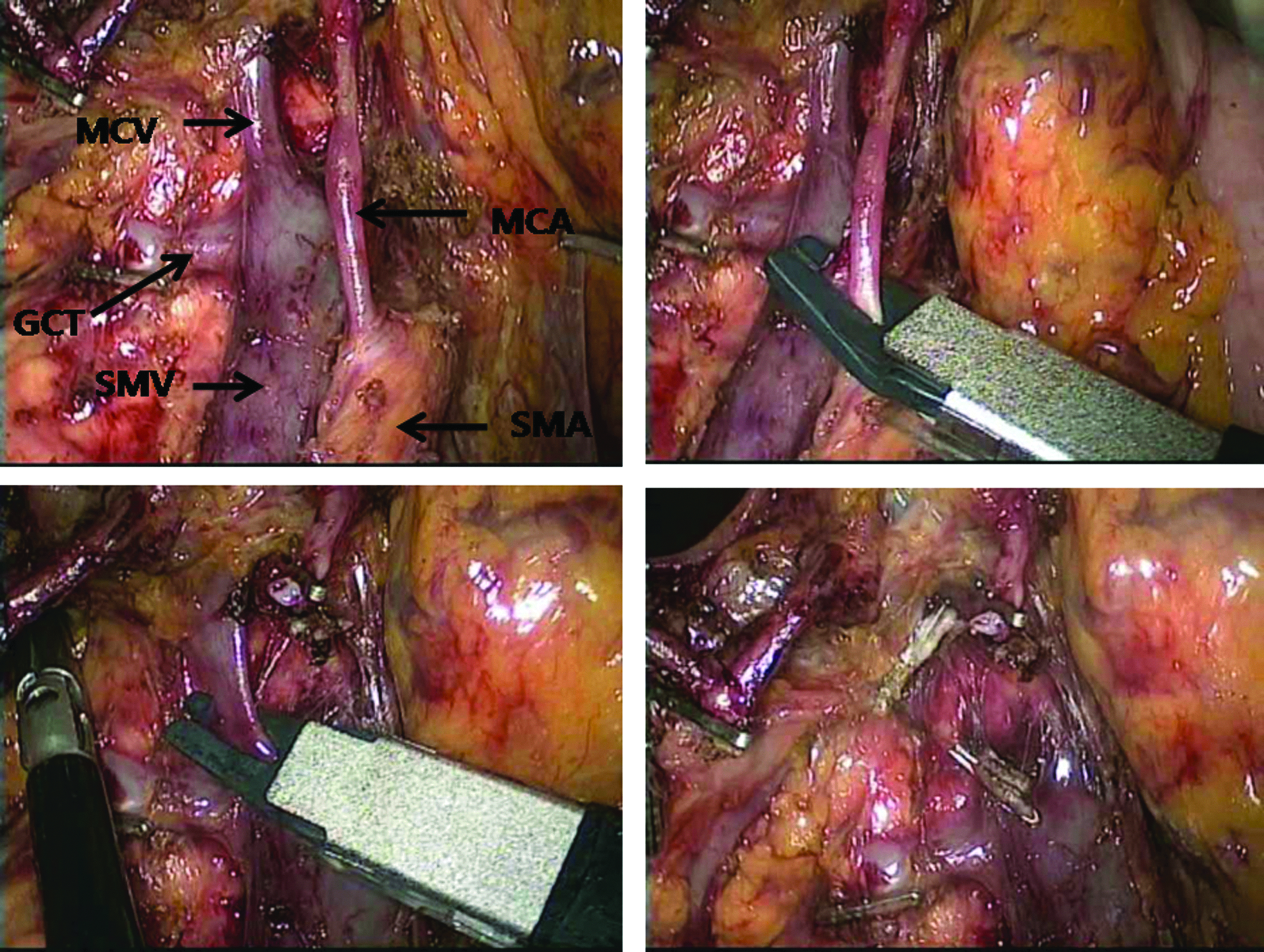
High ligation of the middle colic vessels from their origin. Note that one of the colic vein drains to the gastrocolic trunk was also ligated and divided adequately. GCT, gastrocolic trunk; MCA, middle colic artery; MCV, middle colic vein; SMA, superior mesenteric artery; SMV, superior mesenteric vein.
For left-sided lesions, dissection was performed from the caudal to cranial direction after ligating and dividing the left colic artery origin. The inferior mesenteric vein was then skeletonized until the left colic vein appeared. The left colic vein was ligated and divided at the origin. Middle colic vessels were identified at the inferior border of the pancreas by meticulously dissecting the lymph nodes anterior to the superior mesenteric artery and vein. The origin of the middle colic vessel was completely exposed, and vessel ligation was performed at the middle colic artery and MCV origin or at the left branch origin. At that time, variations of thin MCV were treated with special caution.
For midtransverse lesions, the transverse mesocolon was dissected from the inferior border of the pancreas after stretching the transverse mesocolon. The middle colic vessels were handled in the same manner. In this case, both hepatic and splenic flexures were usually fully mobilized. The surgeons preferred the medial to lateral approach for most cases. The surgical principle was to secure a distance of at least 10 cm for the proximal and distal margin.
The choice to perform laparoscopic surgery or open surgery was based on the surgeons' medical decision. In case of laparoscopic surgery, extracorporeal anastomosis was performed in a method similar to that used in open surgery.
Statistical analysis
To compare the two groups, a Student's t test was performed for continuous data, and Fisher's exact test was used for categorical data. The Kaplan–Meier method was performed for survival analysis, and the survival comparisons were performed with the log-rank test. Statistical significance was defined as P < .05. IBM (Armonk, NY) SPSS software (version 18.0) was used for statistical analysis.
Results
Patient characteristics and perioperative management
There were no statistical differences in gender, body mass index, American Society of Anesthesiologists score, history of previous abdominal surgery, preoperative carcinoembryonic antigen level, tumor location, operative method, or proportion of patients who received adjuvant chemotherapy between the two groups. The mean age of patients who received laparoscopic surgery was significantly older than that of those who received open surgery (65.7 ± 10.0 years versus 56.0 ± 15.9 years, P = .010) (Table 2).
ASA, American Society of Anesthesiologists; BMI, body mass index; CEA, carcinoembryonic antigen; LAC, laparoscopy-assisted colectomy; LHC, left hemicolectomy; OC, open colectomy; RHC, right hemicolectomy; SD, standard deviation.
Pathologic characteristics, including oncologic quality of specimen
Forty-eight patients (60.8%) in the LAC group and 15 (65.2%) in the OC group had stage II cancer. Thirty-one patients (39.2%) in the LAC group and eight (34.8%) in the OC group had stage III cancer. No differences were observed in the ratio of stage II and stage III disease between the two groups. Other pathologic results, such as pathologic T stage, N stage, tumor differentiation, and lymphovascular or perineural invasion, also showed no statistical differences. In the LAC group, the mean tumor size was significantly smaller than in the OC group (5.2 ± 2.3 cm versus 7.6 ± 3.4 cm, P = .004). The differences in proximal resection margin, distal resection margin, and mesenteric margin between the groups were statistically minimal, but more retrieved lymph nodes were detected in the OC group (17.5 ± 9.4 versus 26.4 ± 11.6, P = .002) (Table 3).
DRM, distal resection margin; LAC, laparoscopy-assisted colectomy; LN, lymph nodes; OC, open colectomy; PRM, proximal resection margin; SD, standard deviation.
Intra- and postoperative clinical outcomes
The operation time was longer by about 90 minutes for laparoscopic surgery than for open surgery (332.5 ± 81.8 minutes versus 241.3 ± 42.1 minutes, P = .000). Although there were no differences in the amount of intraoperative transfusion or the time to return of bowel function, the LAC group showed a faster postoperative recovery with respect to the return to an oral diet (4.5 ± 1.2 days versus 5.4 ± 1.8 days, P = .013) and postoperative length of hospital stay (12.1 ± 4.2 days versus 15.9 ± 4.8 days, P = .000) (Table 4).
LAC, laparoscopy-assisted colectomy; OC, open colectomy; SD, standard deviation.
Intraoperative and postoperative complication rates were not significantly different between the groups. All intraoperative complications of laparoscopic surgery were related to bleeding. Among them, 2 cases were managed conservatively with compression and electrocautery, but 1 case was converted to open surgery because of uncontrolled bleeding around the pancreas. Chylous ascites was the most common postoperative complication, but the incidence rate between groups was not statistically different (P = .375). All postoperative complications were resolved conservatively.
The conversion rate from LAC to OC was 6.3% (5/79) (Table 4). The reasons for conversion were as follows: bulky masses suspected of invading adjacent structures (2 cases), severe adhesion (1 case), the uncontrolled bleeding mentioned above (1 case), and twisted anastomosis (1 case).
Long-term outcomes
The median follow-up period was 67.5 (15–208) months in the LAC group and 132 (21–204) months in the OC group. There were no statistically significant differences in overall survival rate (OS) or disease-free survival rate (DFS) between the two groups (5-year OS, 90.4% versus 90.5%, P = .670; 5-year DFS, 84.2% versus 90.7%, P = .463) (Fig. 2). The 5-year OS rates for stage II were 91.0% for the LAC group and 92.3% for the OC group (P = .715). The 5-year OS rates for stage III were 89.7% for the LAC group and 87.5% for the OC group (P = .788). The 5-year DFS rates for stage II were 87.2% for the LAC group and 92.3% for the OC group (P = .570). The 5-year DFS rates for stage III were 79.0% for the LAC group and 87.5% for the OC group (P = .642). Ten-year survival in the LAC group was reduced to 88.0% in OS for stage II and 80.7% in OS for stage III, without changes in DFS or in survival rates for the OC group. Two patients whose follow-up period was less than 12 months were excluded from the survival analysis.
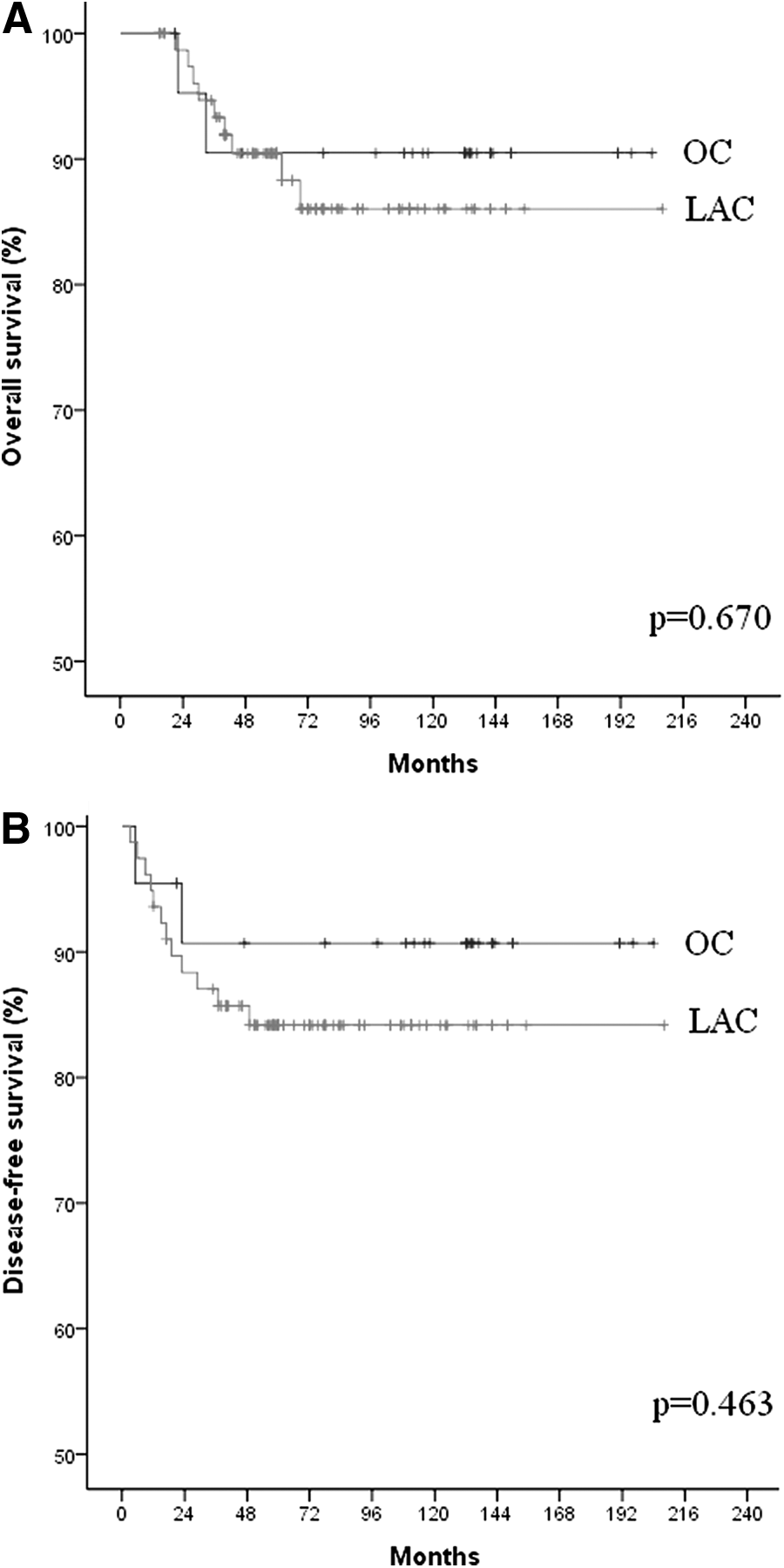
Cumulative survival of stage II and III transverse colon cancer patients. There is no significant difference between the laparoscopy-assisted colectomy (LAC) (n = 77) and open colectomy (OC) (n = 23) groups.
Discussion
Laparoscopic surgery has not been used as often for transverse colon cancer as it has in other sites of colon cancer for the following reasons.
First, transverse colon cancer has a relatively low incidence, making up about 10% of total colon cancers.16,17
Second, surgical methods may vary according to cancer site. To overcome the characteristic learning curve of laparoscopic surgery, sufficient experience with consecutive cases needs to be accumulated. However, the low incidence of transverse colon cancer and the surgical method variability hinder the surgeon's learning experience. Moreover, considering the lack of tactile sensation (especially for early-stage transverse colon cancer) in laparoscopy, the variability of surgical methods by cancer site is a burdening factor for the surgeons. We preferred to perform routine preoperative colonoscopic tattooing and clipping for clinically suspected T2 or less lesions. Preoperative localization proved its utility in proactive surgical planning and intracorporeal detection of the small lesions. Fortunately, all the preoperatively localized cases had successful identification of cancer site intracorporeally among the LAC group. Notably, laparoscopic surgeons also should keep in mind that some advanced colon cancers without preoperative localization are not detectable out of expectations.
Third, the middle colic artery, MCV, superior mesenteric artery, and superior mesenteric vein are anatomically adjacent to such important organs as the duodenum and the pancreas. The MCV especially presents accessory veins in more than 60% of cases, and their drainage to the superior mesenteric vein presents variations that make them vulnerable to injury. Therefore, laparoscopic ligation of the middle colic vessels at their origin and laparoscopic dissection of the lymph nodes are technically demanding. 18
Fourth, a relatively larger surgical field is necessary for transverse colon mobilization and no tension anastomosis compared with other sites of colon cancer. During surgery frequent position changes for the patient and surgeon are needed. Both wide anatomical knowledge and laparoscopic surgery experience are required. To mobilize the splenic flexure colon, refined surgical skill is needed to resect the adjacent omentum and to avoid injury of the transverse colon mesentery, pancreas tail, or spleen at the same time. These difficulties related to the use of laparoscopic surgery for transverse colon cancer provide the basis for its exclusion from major prospective randomized trials and also impede other studies on LAC from being carried out.
Up until recently, all published studies regarding laparoscopic surgery for transverse colon cancer have been retrospective in study design, and most have dealt only with the short-term outcomes of surgery. However, ultimately the most important results of cancer surgery are the long-term oncological outcomes. Recent studies show that survival outcomes differ according to the anatomical segment of colon in which the cancer occurred.16,19,20 Therefore, to determine the effect of laparoscopy on the long-term survival rate for transverse colon cancer, the suitable study method is to compare data from the open surgery and laparoscopic surgery groups treated in the same time period.
Among previous studies on the topic that have reported long-term survival rates, only two articles (those by Zhao et al. 14 and Kim et al. 15 ) used a suitable study method for satisfying these conditions. Other, more limited studies have presented the survival of laparoscopic surgery for transverse colon only, 12 analyzed descending colon cancer and transverse colon cancer together, 11 or compared laparoscopic surgery for transverse colon cancer with laparoscopic surgery for other sites of colon cancer.6,7,9,13
Here, we compared laparoscopic and open surgery for transverse colon cancer by presenting not only short-term but also long-term outcomes with a relatively long follow-up of 14 years. The beginning point for this research (April 1996) was the first time that laparoscopic surgery was used for transverse colon cancer, and we had begun using laparoscopic surgery 2 years before. In reviewing the results of this study, consideration should be given that the data include a certain learning curve.
The two groups' characteristics were not statistically different except for age and tumor size, and so they were suitable for a comparative analysis of short- and long-term outcomes. Tumor size was significantly larger in the OC group than in the LAC group. The surgeons likely considered the difficulty of manipulating large tumors when selecting the surgical method. The LAC group's mean age was about 10 years older than the OC group's, although age was not considered as a selection or exclusion criterion for laparoscopic surgery. These differences in basic characteristics may reflect selection bias, which is the limitation of our study.
The notable pathologic outcome in our study was that the number of retrieved lymph nodes was significantly smaller in the LAC group. Among the transverse colon cancer articles, only the report by Akiyoshi et al. 9 also showed a smaller number of retrieved lymph nodes by laparoscopy. Other articles showed that the open surgery group and the laparoscopic surgery group had similar lymph node retrieval, and one 14 even showed more lymph node retrieval by laparoscopic surgery, although the difference was not statistically significant. Lymph node harvest is associated with the extent of radical surgery, which is associated with long-term outcomes. Sargent et al. 21 reported that the survival rates for stage II and III colon cancers can be increased by harvesting more lymph nodes. Weber et al. 22 reported that a complete mesocolic excision and radical lymph node dissection by central ligation did not increase complication rates but increased long-term oncologic outcomes.
The number of lymph nodes harvested in LAC is generally less because, even though vascular ligation was performed around the origin of each vessel, lymph node dissection was difficult and dangerous near the middle colic vessels, and therefore sufficient soft tissues (including lymph nodes) were not resected. However, this was not the case in our study because there were no significant differences between groups for the proximal, distal, or mesenteric margins. After reviewing the data, we observed that there were seven pathologists who prepared colon cancer pathology reports during the study period and that the reports were generally prepared in different time periods. Storli et al. 23 reported that the number of lymph node harvested can differ remarkably based on the pathologist's specimen-handling skill, not just on tumor or surgical factors.
For intraoperative and postoperative outcomes, the LAC group showed a longer operation time compared with the OC group. Yet, there were no significant differences in the amount of intraoperative bleeding or in the complication rates. Furthermore, the resumption of diet and the length of postoperative hospital stay were significantly shortened. Our study results are in accordance with those of previous studies regarding laparoscopic surgery for transverse colon cancer. Although there are difficulties in using laparoscopic surgery in transverse colon cancer, there are also general advantages for its use in transverse colon cancer.
For postoperative complications, there were no significant differences between the two groups (P = .390). A notable result is that chylous ascites developed in 9 of the 102 patients (8.8%). In previous articles chylous ascites occurrences were reported as 5.2% for the laparoscopic surgery group by Han et al. 12 and 4.3% in the open surgery group by Kim et al. 15 Chylous ascites after laparoscopic surgery for colon cancer is associated with extensive lymph node dissection, 24 and the preference of our study's surgeons to use electrocautery in lymph node dissection may have contributed to the relatively high occurrence. The patients in our study recovered well from chylous ascites without any other symptoms after 1 or 2 days of a nil per os diet and a subsequent low-fat diet.
The conversion rate of 18.2% reported by Schlata et al. 6 (the authors who first reported on laparoscopic transverse colon cancer surgery) is as high as the rates reported by the COLOR study group 3 and the COST study group 4 regarding other sites of colon cancer. After the initial report of Schlata et al., 6 other studies reported a conversion rate ranging from 2% to 5%. Compared with these results, a relatively higher conversion rate of 6.3% was observed in our study. Conversion is associated with adverse short-term results, such as increased morbidity or longer hospital stay, 25 and is reported to have an adverse effect on long-term outcomes, such as DFS and OS.4,26 Therefore, because laparoscopic surgery is difficult and the conversion rate is relatively high in transverse colon cancer, detailed preoperative planning and cautious selection in operative methods are essential for decreasing the conversion rate.
Regarding the long-term survival, we found no significant differences in OS or DFS between the LAC and OC groups. However, the LAC group showed a tendency toward decreased DFS and OS. This may be explained by the following mechanisms. The LAC group includes the surgeons' learning curve period. Conversions and longer operation time would have had adverse impacts on long-term outcome. Confounding factors on survival also include the significantly older age of the LAC group. The retrospective nature and small sample size of this study allow the risk of a type II error.
Five previous studies reported that the 5-year survival rates for transverse colon cancer after laparoscopic surgery are as follows: stage II OS was 87.7%–93.7%, and DFS was 85.5%–94.4%; stage III OS was 64.2%–88.2%, and DFS was 53.3%–79.1%. These results are in accordance with our results (Table 5). The noninferiority of laparoscopic surgery compared with open surgery for transverse colon cancer is also similarly observed with regard to the long-term survival results reported for other sites of colon cancers.
This represents the mean, not the median, follow-up period for this study.
DFS, disease-free survival; OS, overall survival.
Compared with previous studies about laparoscopic resection for transverse colon cancer, this study presents the longest follow-up period. In addition, strict exclusion criteria were applied, the confounding factors were controlled, and then the results of laparoscopic resection for transverse colon cancer were compared from those with open transverse colon cancer surgery performed in the same time period. Therefore, this study provides evidence for the application of laparoscopic surgery for transverse colon cancer as an alternative surgical method to open surgery. Study limitations are the small patient number and single-center retrospective study design. Further multicenter, prospective randomized studies are warranted.
Conclusions
For transverse colon cancer treatment, laparoscopic surgery has better short-term outcomes than open surgery. In long-term survival, significant differences were not observed. Therefore, laparoscopic surgery can be a useful alternative to open surgery in transverse colon cancer, as it is for sites of other colon cancers.
Footnotes
Disclosure Statement
No competing financial interests exist.