
Abstract
Abstract
Objective:
Complete resection of the pyriform sinus fistula (PSF) tract is challenging due to repeated infection and inadequate procedures. We present our experiences with intraoperative endoscopic-assisted intubation or instillation of dye through the internal opening as a guide to identify the tract.
Materials and Methods:
We retrospectively reviewed the charts of 73 consecutive patients diagnosed with PSF during 1999 until 2014 from two tertiary referral centers. Demographics, clinical presentation, imaging, treatment, and outcome were analyzed.
Results:
The intraoperative endoscopy was successfully conducted in all 73 cases. No gender predominance was observed. Of the anomalies, 94.5% were left-sided. Presenting symptoms consisted of neck abscess (n = 48), acute suppurative thyroiditis/thyroid abscess (n = 9), neck mass with or without dyspnea (n = 12), and thyroid nodule (n = 4). Barium esophagography and computed tomography scan with oral or intravenous contrast had a satisfactory positive predictive value. Partial thyroidectomy was performed on 25 cases (34.2%) if the ipsilateral thyroid was involved. Good outcome was achieved in all but 3 patients (70/73, 95.9%) during a median follow-up of 4 years (range, 8 months–14 years). Two patients developed postoperative complications: temporary vocal fold motion impairment and left-sided Horner's syndrome, respectively. PSF recurred in 1 case.
Conclusions:
A complete resection is essential for good outcomes. Intraoperative intubation or methylene blue injection by endoscopy can simplify the identification of the fistula tract during surgical exploration.
Introduction
S
Materials and Methods
Between January 1999 and June 2014, 73 children underwent endoscopic-assisted operation under the direction of an experienced surgeon (Z.L.) at two tertiary pediatric referral centers (Children's Hospital of Shanghai Jiao Tong University and Children's Hospital of Fudan University, Shanghai, China). Patients (n = 12) who refused or had not yet undergone definitive surgery were excluded from this study.
The medical records including each patient's demographics, clinical findings, operative details, and postoperative course were reviewed. The criteria used to differentiate third from fourth pharyngeal arch anomalies were used as we and others previously described.3,6 Ethical approval was obtained from the Ethics Board of the Children's Hospital of Shanghai Jiao Tong University and Children's Hospital of Fudan University. Written informed consent was obtained from the patient's parents on behalf of the child. Statistical analysis was performed using the SPSS version 17.0 software package (SPSS, Inc., Chicago, IL). A P value of < .05 was considered significant (alpha = 0.05, two-tailed).
Surgical procedures
Patients were placed supine across the table with the neck hyperextended following induction of general anesthesia with endotracheal intubation. A 5-cm transverse elliptical neck incision was made at the level of the cricoid cartilage, with a previous surgical incision used whenever possible. Subcutaneous tissue and the platysma flap were divided. The linea alba cervicalis was incised, and then the sternocleidomastoid muscle and anterior cervical strap muscles were contoured and retracted laterally. After ligation and cut of the superior thyroid artery and vein, the upper pole of the thyroid lobe is retracted medially. Meticulous exploration of the neck was performed first after mobilizing the ipsilateral thyroid. Microsurgical instruments were used during the dissection to protect vital tissues and structures. The inferior cornu of the thyroid cartilage was covered by the cricothyroid muscle. The inferior pharyngeal constrictor muscle was then dissected from the oblique line of the thyroid cartilage. The recurrent laryngeal nerve was identified until its entering the larynx around the cricothyroid joint. The posterior cricoarytenoid muscle was an appreciated landmark to remind the surgeon that damage to the recurrent laryngeal nerve might occur. In some patients, resection of inflammatory and fibrotic tissues around the inferior cornu was necessary to provide exposure of the lesion. The sinus tract was carefully sought.
Then, endoscopy (model GIF-160 endoscope; Olympus, Tokyo, Japan) was performed by an assistant. Light was applied as an indicator with its transillumination identified in the operative field. If the internal opening was seen in the pyriform fossa (Fig. 1A), a 3 French catheter was inserted into the tract and left it in the loci. In some cases, it was found that the catheter was could easily slip out of position, and then a volume of about 0.5–1.0 mL of diluted methylene blue was injected through the catheter into the tract (Fig. 1B). A traction suture was placed for further mobilization with gentle traction. Incision of the inferior pharyngeal constrictor muscle and exposure of the inferior cornu of thyroid cartilage might simplify the dissection of the proximal part of the fistula. The tract was traced in the cephalad direction until its expansion part was reached near the apex or base of the pyriform fossa, and then it was ligated and excised at its starting point. Finally, the fistula tract with or without its adjacent tissues (e.g., part of the thyroid, muscle, scar tissue) was removed en bloc. The incision was closed in layers with absorbable interrupting fine sutures. No drains were needed if resection was complete.
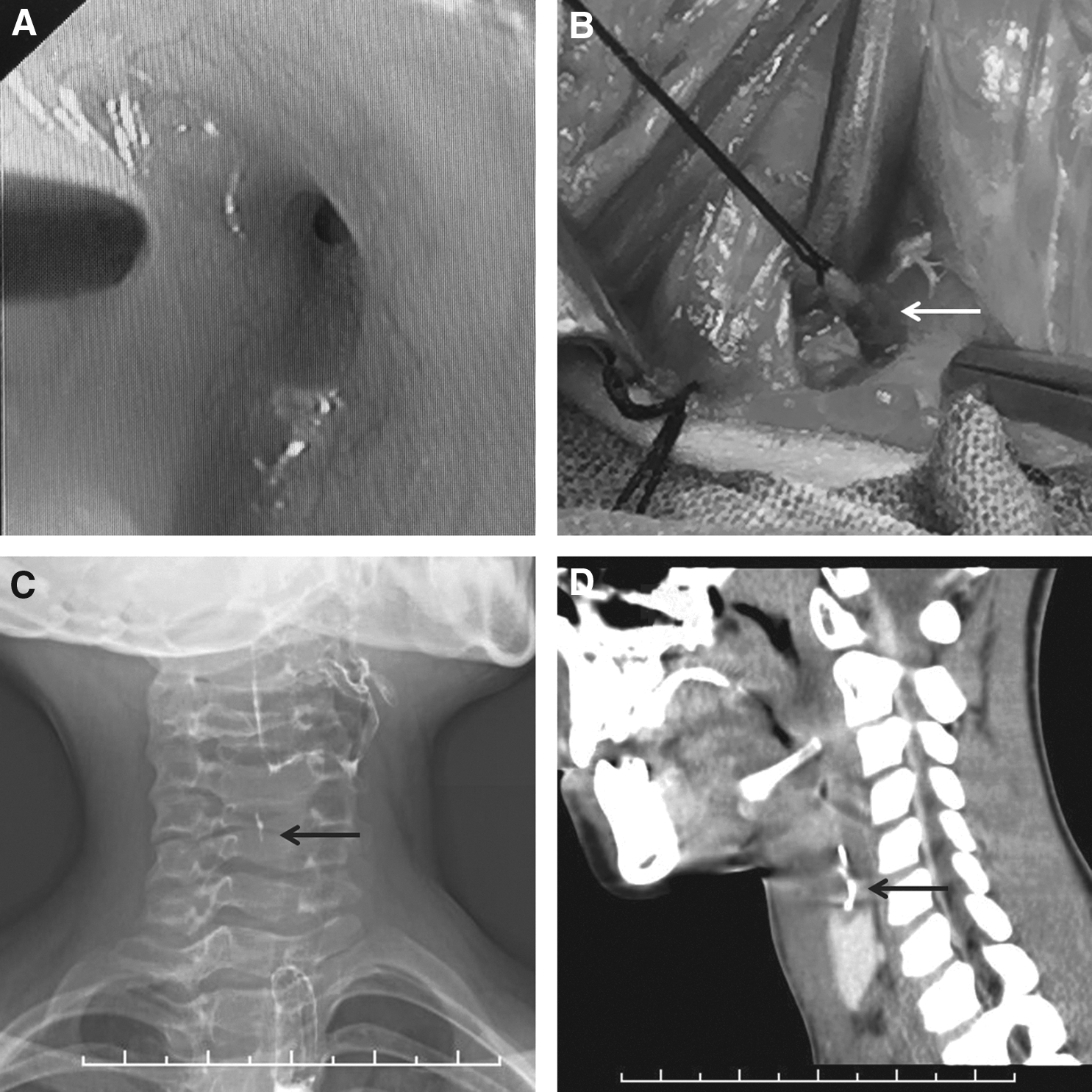
Imaging findings and intraoperative images.
Results
In this series (Table 1), we had 73 patients (38 males; male:female ratio, 1.09:1) with a median age at the time of initial onset and accurate diagnosis of 3 years (range, 0–11 years) (82.2% of the children were under 5 years old) and 5 years (range, 12 months–13 years), respectively. The anomalies were on the left side in 69 cases (94.5%), right side in 2 cases, and both sides in 2 cases. The clinical presentations were neck abscess (n = 48, 65.8%), acute suppurative thyroiditis/thyroid abscess (n = 9, 12.3%), neck mass with or without dyspnea (n = 12, 16.4%), and thyroid nodule (n = 4, 5.5%). Among this group, there were 20 third pharyngeal anomalies and 52 fourth pharyngeal anomalies; we were unable to define the embryologic origin of the discrete tract in 1 case, given the extensive scarring during the surgical exploration. Before endoscopic-assisted operation, initial surgical procedures included incision and drainage in 62 cases (median, 2; range, 1–12) and traditional open-neck in 16 cases (median, 1; range, 1–2). Repeated incision and drainage, after initially failed operations (incision and drainage or open), were performed in 44 cases. One girl was misdiagnosed as having lymph node tuberculosis at another hospital and received antituberculous therapy (isoniazid and rifampicin) for 3 months with no effect.
AST, acute suppurative thyroiditis; PPV, positive predictive value.
Barium esophagography in the noninfected period showed the sinus tract in 100% of cases (Fig. 1C). The positive predictive value (PPV) of other diagnostic modalities was 93.7% (15/16) for oral-contrast computed tomography (CT) (Fig. 1D), 67.5% (27/40) for intravenous contrast-enhanced CT, 46.1% (6/13) for non-contrast CT, and 10.4% (5/48) for sonography. Magnetic resonance imaging (MRI) and pharyngoscopy also had satisfactory PPV (66.7% [2/3] and and 75% [3/4], respectively) but were not widely used in this series. Thyroid function was reported normal in most tested cases (15/16, 93.7%); 1 patient had slight hyperthyroidism, and no medical therapy was needed. Isotope thyroid scan (n = 6), X-ray of the neck (n = 2), and fine-needle aspiration (n = 2) did not contribute to the diagnosis in any of the cases.
The intraoperative endoscopy was successfully conducted in all cases. Partial thyroidectomy was performed on 25 cases (34.2%) if the ipsilateral thyroid was involved. Histopathologic examination of the specimen revealed a tract lined with stratified squamous epithelium or ciliated columnar epithelium, with or without inflammatory and fibrotic tissues. A drain was placed for 24–48 hours in 27 cases.
Good outcome was defined as complete excision of the lesion with no recurrence and no postoperative complications. This was achieved in all but 3 patients (70/73, 95.9%) during a median follow-up of 4 years (range, 8 months–14 years). The surgical pathology report of the recurrent case showed that no epithelial-lined tract was present in the specimen. The boy was re-admitted with neck swelling 6 months after surgery. A repeat barium swallow demonstrated the persistence of the sinus tract. The patient was managed conservatively with antibiotics intravenously (ceftriaxone and metronidazole) and is waiting for definitive operation. Two patients developed postoperative complications: temporary vocal fold motion impairment (voice hoarseness) and left-sided Horner's syndrome (ptosis and miosis), respectively. Two patients (2/8, 25%) who underwent open surgery without endoscopic assistance (during 1990 and 1998) experienced recurrence in our hospitals. There was a statistically significant difference between these two groups (Fisher's exact test, P = .025).
Discussion
The nomenclature and classification of pharyngeal anomalies (sinus, cyst, and fistula) are controversial due to its complicated embryological development.7–9 None of the patients in this study followed the theoretical pathways of the third or fourth pharyngeal arch anomaly. It is difficult to determine the origin of the tract without meticulous neck exploration. Clinical presentations of PSF vary with age.1,2,10 Newborns may present with a noninfectious neck cyst, which can compress the trachea and cause stridor and respiratory embarrassment. In contrast, PSF presents in young children as recurrent neck abscess or acute suppurative thyroiditis following an episode of upper respiratory infection. Cervical cutaneous fistula develops only in late childhood. The formation of an external fistula is always the result of repeated infection and surgical management. Because the thyroid is well known to resist infections due to its anatomic and physiologic characteristics, 11 diagnosis of PSF should be suspected in children with acute thyroiditis, especially on the left side. Other entities to be considered in the differential diagnosis include lymphadenitis, tuberculosis, ectopic thyroid, thyroglossal duct anomaly, lymphatic malformation, dermoid cyst, teratoma, lymphoma, etc.12,13
Various diagnostic modalities, including sonography, barium swallow, CT, MRI, and pharyngoscopy, can be used alone or in combination to establish the accurate diagnosis. Sonography is often used as a screening method. We found barium swallow had an excellent PPV in demonstrating the fistula tract when performed during a quiescent period. CT scan with oral or intravenous contrast is also widely used in our hospitals. The presence of a gas pocket within the upper pole of the involved thyroid lobe is thought to be pathognomonic of a PSF tract. MRI may be useful in showing the inflammatory lesion but cannot offer any particular advantage over other imaging methods.14,15 In a meta-analysis, direct pharyngoscopy has been reported having a good PPV (90%). 2 However, pharyngoscopy/microlaryngoscopy is not widely performed in this series because of our limited experience and its requirement of general anesthesia.
The definitive treatment of PSF involves complete resection of the tract performed 8–12 weeks after resolution of the acute infection. Intraoperative endoscopic visualization of the internal opening with subsequent intubation or injection can facilitate the external dissection. In some cases, the sinus tract opening might not be found easily during the first examination. Manipulation of the mucosa and suction of the secretions can be helpful in identifying the opening. Although some tracts could be found without the help of endoscopy, they were further confirmed by the dye. Identification of the recurrent laryngeal nerve during the surgical exploration is sometimes necessary. The sinus tract could penetrate the thyroid cartilage near the inferior cornu, the inferior pharyngeal constrictor muscle, or the cricothyroid membrane when it emerged from the larynx. Incision of the inferior pharyngeal constrictor muscle and exposure of the inferior cornu of thyroid cartilage can help the dissection of the proximal part of the fistula. Based on the anatomy and embryology of the developmental tract in relation to the thyroid, 16 it is rational to perform partial thyroidectomy or hemithyroidectomy (if needed). The recurrence rate in this study is 1.4% (1/73), which is lower than that of open surgery without endoscopic assistance. Failure to excise the tract at a high level might be the cause. It is interesting that Shino et al. 17 reported a case of PSF with double tracts in a 13-year-old girl. The aim should be to achieve complete surgical removal of the tract in its entirety.
Turning to the issue of outcome, 2 patients developed postoperative complications in this study. Vocal fold immobility is always temporary, whereas true vocal fold paralysis is rare. However, the symptoms of Horner's syndrome did not recover after a follow-up of 2 years. Iatrogenic injury to the sympathetic nervous system or other vital tissues should be avoided during surgery. Endoscopic cauterization is reported having a high success rate (91%) and few complications.9,18,19 Hence, endoscopic obliteration of PSF might be a safe alternative to open surgery.
In conclusion, correct diagnosis of PSF is important to avoid inadequate surgery and multiple procedures. A complete resection is essential for good outcomes. Also, intraoperative intubation or instillation of dye by endoscopy can simplify the identification of the fistula tract during exploration.
Footnotes
Acknowledgments
This work was supported by grant 15ZR1434200 from Shanghai Science and Technology Commission.
Disclosure Statement
No competing financial interests exist.