
Abstract
Abstract
Background:
Hem-o-Lok® clips (HOLCs) (Weck® Surgical Instruments, Teleflex Medical, Durham, NC) are widely used for controlling the lateral pedicles in laparoscopic radical prostatectomy, but intravesical HOLC migrations have been reported in more and more studies. This study aimed to summarize clinical presentations, management, and outcomes of these patients.
Materials and Methods:
Six patients with intravesical HOLC migration were retrospectively identified from 750 consecutive patients who underwent robot-assisted laparoscopic prostatectomy between 2005 and 2014 performed by a single surgeon. The PubMed database was also searched for Hem-o-Lok clip migration after laparoscopic prostatectomy.
Results:
The incidence of intravesical HOLC migration in this study was 0.8% (6/750). In total, 22 patients were reported, including six from the current series. Three types of migrations were classified: Type I migration resulted in obstructive lower urinary tract symptoms 2–8 months after prostatectomy, whereas Type II migration led to stone formation, gross hematuria, or bladder spasm; in Type III migration, patients had spontaneous expulsion of the HOLC weeks after surgery.
Conclusions:
Although the incidence of intravesical HOLC migration is relatively low, Type I migration with long-term sequelae remains a concern. The use of HOLCs adjacent to anastomosis should be minimized, and any loose clip must be retrieved to reduce complications.
Introduction
T
However, since Banks et al. 2 first reported intravesical HOLC migration after LRP in 2008, more and more studies began to report different severities of intravesical migration after LRP or RALP. This study aimed to summarize clinical presentations, management, and outcomes of these patients.
Materials and Methods
Seven hundred fifty consecutive patients who underwent RALP by a single surgeon (Y.-C.O.) at the Taichung Veterans General Hospital (Taichung, Taiwan) between 2005 and 2014 were reviewed. All were diagnosed with clinically localized prostate cancer. The RALP procedure was as previously described3–6 using a four-arm standard da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA).
During the operation, the HOLC was used to ligate the lateral pedicles and to control bleeding near the neurovascular bundle. Four to six clips are usually used over each side of the lateral pedicle. Vesicourethral anastomosis was performed using the technique of Van Velthoven et al. 7 with a running 3-0 monocryl suture, which started from the 5 o'clock position and was tied together over the 11 o'clock position. A tennis racket closure was made in closing the widened bladder neck if a bladder discrepancy existed. The intraoperative anastomosis challenge test was performed to avoid urinary leakage. 8 Postoperatively, all of the patients were followed up every 3 months in the outpatient department. Intravesical HOLC migration was diagnosed in 6 patients during follow-up.
A literature review was also performed for published reports on intravesical HOLC migration after LRP or RALP. The 6 patients and published cases were summarized into three groups according to clinical course and presentations. The Hospital's Institutional Review Board approved the data collection and analysis.
Results
In the present study the incidence of intravesical HOLC migration was 0.8% (6/750). The characteristics of the 6 patients with intravesical HOLC migration revealed that 2 of these patients suffered from spontaneous passage of HOLCs, and the other patients were diagnosed by cystoscopy (Table 1). Among them, 1 patient who had received previous radiation therapy suffered from obstructive lower urinary tract syndrome 8 months after salvage RALP. Cystoscopy revealed the HOLC over the anastomosis with bladder neck contracture. Transurethral bladder neck incision with retrieval of the HOLC was performed, but he still received long-term serial dilatation due to urethral stricture.
sUsing the American Joint Committee on Cancer/Union Internationale Contre le Cancer, 7th edition for prostate cancer staging (https://cancerstaging.org/references-tools/quickreferences/Documents/ProstateSmall.pdf).
HOLC, Hem-o-lok clip; LUTS, lower urinary tract symptoms; PSA, prostate-specific antigen; RALP, robotic-assisted laparoscopic radical prostatectomy.
In the PubMed search, there were 16 patients who suffered from intravesical HOLC migration after LRP or RALP among 10 published articles from 2008 to 2014.2,9–17 Six of these 16 patients received LRP, and the others received RALP.
According to the clinical course and presentations, three types of intravesical migrations were determined from the total of 22 patients that included 6 from the present series (Table 2). Type I migration might result from erosion of the HOLC over the vesicourethral anastosmosis, leading to obstructive lower urinary tract symptoms 2–8 months after the prostatectomy due to bladder neck contracture. Long-term complications such as urethra stricture and urinary incontinence were reported.
HOLC, Hem-o-lok clip; LRP, laparoscopic radical prostatectomy; LUTS, lower urinary tract symptoms.
Type II migration was similar to Type I, but the erosion site of the HOLC was a little farther from the urethra. No obstructive symptoms were noted, but stone formation and gross hematuria occurred 10–81 months after the surgery.
Type III migration resulted from migration of unretrieved loose clips during the procedure. Patients complain of spontaneous expulsion of HOLCs weeks postoperatively. These three types of intravesical migration are illustrated in Figure 1.
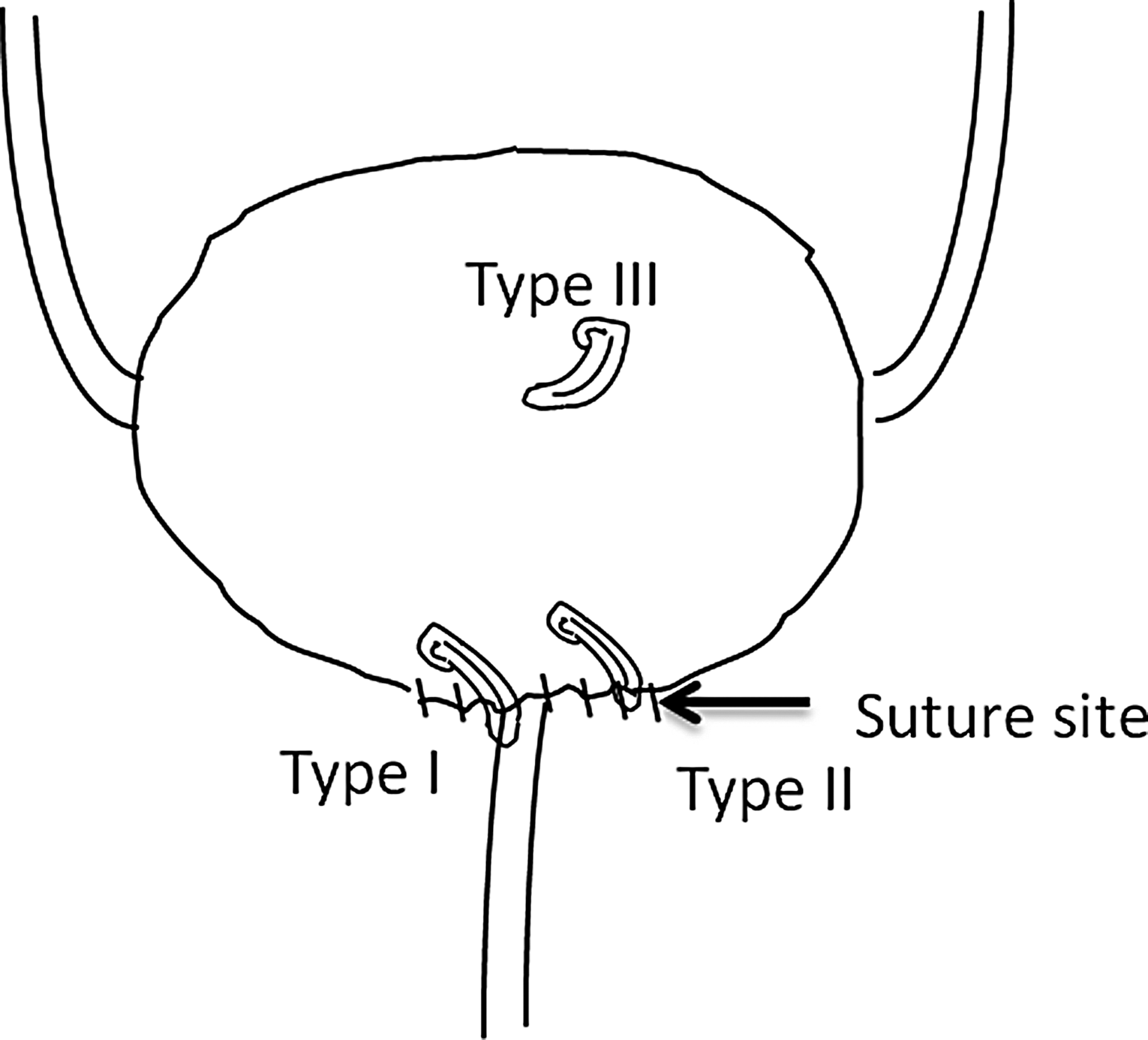
Illustrations of the three types of Hem-o-Lok clip migrations.
Discussion
The HOLC is widely used in laparoscopic surgery because of its secure clamping and easy application. However, a few studies have reported on the erosion or migration of this nonabsorbable clip into the common bile duct, rectum, ureter, duodenum, and urinary bladder.18–22 Among these, intravesical migration after LRP or RALP is the most frequently reported. The present study summarized all published reports about intravesical HOLC migration after LRP or RALP and classified them into three groups according to clinical severity.
The exact incidence of intravesical HOLC migration after LRP or RALP is still unknown. Blumenthal et al. 9 reported 3 cases of HOLC migration from 524 consecutive patients after RALP (3/524 [0.57%]). Yi et al. 15 reported 2 cases from 153 patients after LRP or RALP (2/202 [1%]). In the present series, the incidence is 0.8% (6/750), which is close to those of previous studies. The incidence may actually be higher than in the present report because Type II migration may be underestimated due to some asymptomatic patients.
Intravesical HOLC migration is a rare complication, and most of the studies regarding LRP or RALP complications do not mention it. 3 However, it seems to play an important role in bladder neck contracture after vesicourethral anastomosis.9,15 The mechanism of HOLC migration is currently unclear, but the number of patients with migration to the urinary bladder after LRP or RALP is much more than the number of patients with migration to other organs. Moreover, Zeng et al. 23 also report intraneobladder HOLC migration after laparoscopic radical cystectomy with orthotopic neobladder, implying that vesicourethral anastomosis results in an increased possibility of HOLC migration.
The relatively weak tissue over the vesicourethral anastomosis may facilitate HOLC erosion and eventual migration into the bladder. If erosion occurs over the vesicourethral anastomosis, it causes Type I migration with obstructive symptoms. If the erosion occurs over the reconstructive site of a tennis racket closure, it causes Type II migration. The unretrieved loose clips may directly drop into the bladder during the operation, which causes Type III migration. Due to low incidence, it is difficult to find variables that are predictive of HOLC migration. But, in our series, 2 of the 6 patients with HOLC migration received radiation therapy before or after operation. Radiation therapy might increase the risk of poor healing of the vesicourethral anastomosis. In addition, because 4 patients with HOLC migration were from the last 350 patients, the surgeon's experience might not be related to this complication.
In this study, Type I and Type II migrations occurred 2–8 months and 10–81 months after surgery, respectively. Absorbable clips, such as Laparo-Clip® (Davis and Geck, Danbury, CT), which can degrade within 6 months, 24 may reduce these complications, although there is no current study to support this.
The incidence of intravesical HOLC migration is relatively low, but Type I migration with long-term sequelae is still a concern. The use of an HOLC adjacent to the anastomosis should be minimized, and loose clips should be retrieved to reduce complications.
Footnotes
Disclosure Statement
No competing financial interests exist.