
Abstract
Abstract
Background:
To report a series of children with pelviureteric junction obstruction (PUJO) due to lower polar crossing vessels who underwent laparoscopic vascular transposition. In order to confirm the relief of the obstruction and avoid unnecessary additional procedures, we suggest performing an intraoperative measure of the ureteral opening pressure.
Patients and Methods:
From January 2007 and January 2014, 11 children underwent laparoscopy to treat well-documented PUJO by polar vessels. In the first 7 cases, children underwent a careful dissection of the polar vessels that were transposed cranially in the pelvis. In the last 4 cases, a percutaneous needle was inserted into the renal pelvis, and the ureteral opening pressure was obtained intraoperatively, before and after the vascular hitch procedure, in 3 cases. No vascular relocation was necessary except in 1 case with a polar vessel unrelated to the obstruction.
Results:
The laparoscopic procedure was feasible in all cases. Median operative time was 90 minutes without intraoperative complications. In the last 3 cases, a decrease in the renal pelvic pressure was demonstrated just after releasing the ureter from the polar vessels, confirming the extrinsic obstruction. In 1 case, the intraoperative pelvic pressure measurement showed that there was no vascular compression but that obstruction was due to renal rotation. During follow-up (range, 12–96 months) all patients reported resolution of their symptoms, nine children showed a decrease in the hydronephrosis grade, and all but one with poor function had improved drainage on diuretic renography.
Conclusions:
Intraoperative measurement of ureteral opening pressure may help to confirm that the vascular hitch procedure has relieved the pelvic obstruction, precluding the need for dismembered procedures. We believe that in some doubtful cases, with the addition of intraoperative pelvic pressure measurement, vascular hitch may be considered a safe procedure to treat selected cases of PUJO in children.
Introduction
C
Nevertheless, some children with persistent or increasing hydronephrosis, low relative renal function on scintigraphy, or urinary tract infection (UTI) breakthrough while on conservative treatment need to be operated on. Open dismembered Anderson–Hynes pyeloplasty is the gold standard procedure to treat PUJO in children, but the laparoscopic approach has shown similar outcomes. 4 Laparoscopic pyeloureteral anastomosis in small children remains a challenging task, although robotic pyeloplasty has been felt to be technically easier. 5 PUJO due to crossing vessels, frequently observed in adults, is a rare condition in neonates and has a slight incidence in older children. 6 There is a lack of consensus regarding the surgical treatment of this vascular anomaly. Although some authors have proposed dismembered pyeloplasty to exclude intrinsic associated anomalies, others, in order to minimize technical difficulties and improve outcomes, have described simpler procedures that do not involve pyeloureteral anastomosis, like pyelopexy, the Fenger procedure, or vascular transposition.7–9
Here our purpose is to report the long-term follow-up of children who underwent laparoscopic vascular transposition and to suggest an uncomplicated intraoperative test to confirm the relief of the obstruction.
Patients and Methods
From January 2007 and January 2014, 11 children (five boys and six girls) were included in this study. All anatomical relationships between lower pole crossing vessels and PUJ were classified according to Schneider et al. 10 Surgical indications included two or more of the following conditions: presence of meaningful clinical symptoms, obstruction on diuretic renogram (diethylenetriaminepentacetate [DTPA]), decrease on relative renal function (dimercaptosuccinic acid), or worsening of hydronephrosis on follow-up. The median age at presentation was 96 months (range, 36–168 months). None of the children had prenatal diagnosis. All had high-grade hydronephrosis (GIII–GIV) according to the Society of Fetal Urology classification. 11 Six patients presented with pain, and in 5 patients UTI was the presenting symptom. In one child incidental hydronephrosis was diagnosed during screening for melanoma metastasis. Median preoperative relative renal function was 26% (range, 10%–45%). Only one child showed intermittent obstruction on DTPA. Six were clearly obstructed, and three were indeterminate (Table 1).
Type according to Schneider et al. 10
DMSA, dimercaptosuccinic acid; DTPA, diethylenetriaminepentacetate; Int, intermittent; LK, left kidney, Ob, obstructed; RK, right kidney; RRF, relative renal function; Und, undetermined; Uno, unobstructed; US, ultrasound grade (G) (according to the Society of Fetal Urology 11 ); UTI, urinary tract infection.
Our institutional review board approved this work, and all parents provided informed consent.
Surgical technique
Our technique of laparoscopic vascular transposition consisted of mobilization of the lower polar vessels via the transperitoneal approach in a modified lateral decubitus (45°) with the child placed at the edge of the surgical table. After careful dissection of the vascular bundle and release of ureteral adhesions, we observed the decrease of size of the renal pelvis. Sequentially, the polar vessel was sutured in a tunnel formed by an invagination of the anterior pelvic wall as described in the Chapman procedure.9,10,12–14 One tip is to pass the first suture transparietally, stabilizing and fixing the vascular bundle into the pelvic tunnel to assist the remaining suture.
In the first 7 cases we performed laparoscopic vascular transposition alone, without any additional procedures; however, in the last 4 cases, in order to confirm release of the obstruction and to exclude intrinsic PUJ anomalies, we performed an intraoperative pelvic pressure measurement as previously described. 15 In brief, with laparoscopic visualization and prior to ureteral dissection, a fine-needle was inserted percutaneously into the renal pelvis, and the ureteral opening pressure was evaluated three times using a water column device. The needle was left in place while the procedure was completed, and then another measurement was taken (Fig. 1). We assumed, in agreement with other authors,15,16 that if the opening pressure was lower than 14 cm of water, then the junction was considered unobstructed. No double J stent was inserted, and the bladder catheter was removed before discharge.

Illustration of the intraoperative view. Note that the needle does not interfere with the procedure. A, water column; B, dilated pelvis.
Success after procedure was defined as resolution of symptoms (UTI or pain), improvement of hydronephrosis, and/or increased elimination on diuretic renography.
Results
Laparoscopic vascular relocation was feasible in all cases without conversion or intraoperative complications. Median operative time was 90 minutes (range, 60–120 minutes). We found three children with type 2 anatomical variation and seven with type 3, and only one was type 1 in a well-documented digital video appraisal. In the last 4 cases, the intraoperative pelvic pressure was measured, and in 3 cases, it decreased immediately after releasing the ureter from the polar vessels, thus confirming the extrinsic obstruction. In the remaining child (with a type 1 variation) we found the polar vessels without PUJ or ureteral compression. In Case 8, with a type 3 malformation (prolapsed pelvis), the ureteral opening pressure was initially 24 cm of water and dropped to 6 cm after ureteral release and vascular cranial fixation. In only 1 case of type 1 malformation (Case 10), a polar vessel was found without ureteral relationship, and renal rotation was responsible for ureteral compression. The ureteral opening pressure was 7 cm of water initially and went down to 3 cm of water after pelvic and renal fixation. In the last case (Case 11 [type 3]), the pressure dropped from 15 to 6 cm of water after ureterolysis, and only a vascular hitch was performed (Fig. 2).
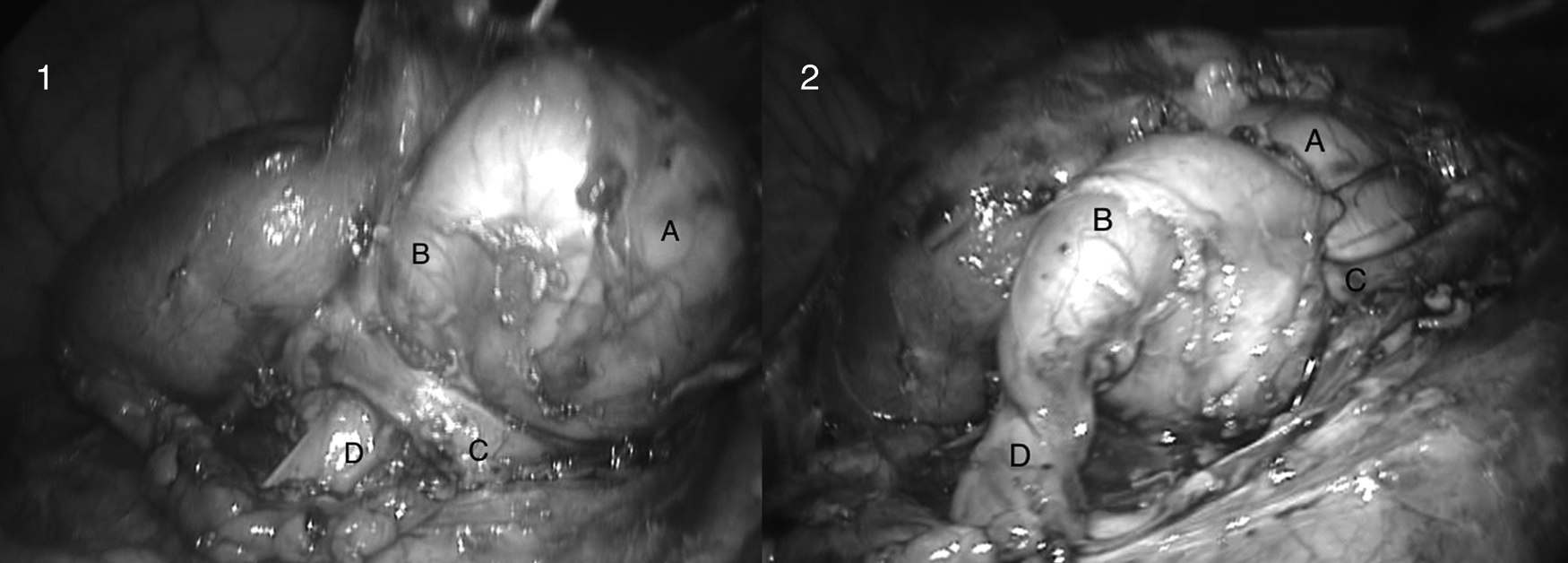
Photographic representation of Case 11.
All children were discharged 1 or 2 days after the surgery. Follow-up (range, 12–96 months) showed complete resolution of symptoms (UTI or pain), and decrease in hydronephrosis grade was seen in nine children (81.8%). Although none of the children displayed significant improvement in relative renal function, all but one showed improved drainage on diuretic renogram (DTPA) and became unobstructed. Preoperatively, this child (Case 9) had a poor function and an undetermined diuretic renogram but during postoperative follow-up has achieved resolution of symptoms and ultrasound improvement.
Discussion
The relationship between lower polar vessel and hydronephrosis was first described by Von Rokitansky in 1842 (as reported by Smith et al. 9 ). Since then, many authors have been trying to elucidate this anomaly. The obstruction of the PUJ by crossing polar vessels is intermittent and must be suspected in older children with recurrent renal colic pain and hydronephrosis. The renal function may be normal in children with PUJO without UTI.6,9,17 In our series, only three children had preserved function, probably because of the high prevalence of UTI. Similar results have been reported by Hacker et al., 6 who found that children with PUJO by polar vessels had decreased relative renal function and delayed surgical management.
Different techniques have been used to treat this condition. As decribed by Smith et al., 9 Hellstrom (in 1949) proposed mobilization and perivascular fixation of the crossing vessel, while Chapman (in 1959) described ureterolysis combined with lower polar vessel mobilization and cranial fixation within a pelvic tunnel.
In the modern era, Smith et al. 9 (in 1982) revisited the Chapman procedure with good results. The authors followed up 19 patients for a period of 5–20 years with 90% of resolution of symptoms. Meng and Stoller 18 (in 2003) were the first authors to report vascular relocation using the Hellstrom technique via the laparoscopic approach. They reported this procedure in nine adults, with resolution in all cases. These authors observed that the herniation and subsequent ureteral kinking were responsible for the obstruction and stated that changing the geometry may be enough to alleviate the obstacle. 18 Another important observation is the existence of several anatomic variations as studied by Sampaio. 19 These double vascular bundles form a vascular window and could facilitate a PUJ prolapse with increasing obstruction. 9 Vascular compression in these cases is not in the PUJ but in the proximal ureter (Fig. 3), creating an ureteral bend like a swan-neck ureter. 10 Therefore, the junction is certainly healthy, and correcting the herniation is all that is needed.10,12,13 This observation is supported by histological analysis of the PUJ and crossing vessels. Normal muscle density was found and suggests an inherently different PUJ configuration between intrinsic and extrinsic obstruction. 20

Laparoscopic view of the pelviureteric junction (PUJ) away from the ureteral kinking (type 3).
Functional assessment of crossing vessels as an etiology of PUJO was proposed by Stern et al. 21 They performed an intraoperative Whitaker test in 10 adults with PUJO before and after vascular mobilization and established a straight relationship between the crossing vessels and extrinsic obstruction. Despite not having performed vascular mobilization, but dismembered pyeloplasty, they suggested that the Hellstrom's procedure is warranted. 21 Our previous experience performing antegrade pelvic pressure measurements allowed the use of the modified Whitaker test in the intraoperative period. 15 Some authors have suggested the use of pelvic distension with saline by direct puncture of the pelvis or intravenous hyperhydration and diuretics to confirm pelvic emptying.10,12 Our contribution is to render this subjective analysis (pelvic emptying) into objective parameters, objectively evaluating the pelvic emptying pressure. It is clear, however, that this simple and reproducible “bedside” test should be performed only in doubtful cases, like, for instance, a type 2 anomaly. When an obvious and clear vascular ureteral compression with a prolapsed normal PUJ (type 3) is found, it is enough to perform only ureterolysis and vascular hitch without any dismembered procedures.
One of the great advantages of the vascular hitch procedure is to preserve the integrity of the urinary tract, eliminating the risk of leakage or urinoma and preserving the pyeloureteral motility and ureteral peristalsis. In several cases, it was possible to observe the pyeloureteral peristalsis after the vascular hitch procedure. Also, there is no need for double J stents and therefore no necessity for an additional anesthesia to remove it.22,23
We totally agree with many authors regarding the necessity of more convincing evidence of ureteral unblocking after laparoscopy vascular transposition. However, after more than 50 years of follow-up since Hellstrom first demonstrated comparable outcomes of this procedure to conventional dismembered surgery and after a recent comprehensive review of the anatomic vascular variations that can be treated by this procedure, 11 we feel comfortable offering this procedure to our pediatric patients.
Conclusions
The association of a dynamic, objective demonstration of pelvic emptying with the precise anatomical localization of the crossing vessels and PUJ provided by the laparoscopic approach was associated, in this series, with very favorable outcomes. These findings allow us to conclude that laparoscopic vascular transposition (or just a vascular hitch) may be a safe, feasible, and attractive alternative to treat obstructed hydronephrosis due to polar vessels. Nevertheless, prospective and multi-institutional controlled studies must be conducted to consolidate this judgment.
Footnotes
Disclosure Statement
No competing financial interests exist.