
Abstract
Abstract
Background:
Good indications for laparoscopic hepatectomy are still considered to be tumors located over anterolateral segments of the liver. Tumors located over the right posterior section are considered to be difficult for laparoscopic resection. In this case series, we present our experience on laparoscopic right posterior sectionectomy.
Patients and Methods:
All patient data were prospectively collected. Data on patient demographics, tumor characteristics, operative data, and postoperative outcome were collected and analyzed.
Results:
During the period of May 2010–May 2014, we performed 13 laparoscopic right posterior sectionectomies. The diagnoses were hepatocellular carcinoma in 11 patients, of which 2 were cases of colorectal liver metastasis. Median operative time was 381 minutes, and median blood loss was 1500 mL. Significant bleeding occurred in the first 5 patients. The median size of the tumor resected was 3.7 cm, and the median resection margin was 8.7 mm. Four of the 13 patients (30.8%) were cirrhotic on histological examination. There was no postoperative mortality. Median hospital stay was 7 days.
Conclusions:
Laparoscopic right posterior sectionectomy is technically demanding. A proper inflow and outflow control is mandatory for proper anatomical resection. This surgical principle should not be compromised in the era of laparoscopic hepatectomy.
Introduction
L
In our institution, since 2006 we have performed laparoscopic hepatectomy. Since then, we have performed more than 120 cases of laparoscopic hepatectomy. Our institutional experience was presented elsewhere. 9 With increasing experience in performing laparoscopic hepatectomies, since 2010 we have expanded the indications for laparoscopic hepatectomy to tumors over the right posterior section. According to our knowledge, this is the first case series of laparoscopic right posterior sectionectomy, and we present here our operative technique, methods to overcome the technical difficulties, and lessons learned during these 4 years.
Patients and Methods
All patient data were prospectively collected. All patients underwent chest radiography and contrast computed tomography of the abdomen. Magnetic resonance imaging and ethiodized oil (Lipiodol®; Andre Guerbet, Aulnay-Soubois, France) arteriogram were performed in selected patients. Preoperative liver function was assessed according to the Child–Pugh classification. Indocyanine green retention tests and liver volumetry were performed in selected cases when we considered the residual liver function or volume could be marginal. All procedures were performed by surgeons with expertise in hepatobiliary and laparoscopic surgery. Data on patient demographics, tumor characteristics, operative data, and postoperative outcome were collected and analyzed.
Surgical procedure
The patient was put in the left lateral position. CO2 pneumoperitoneum was established with the Hasson technique at a pressure of 10 mm Hg. Four to five trocars were used. The first port was usually a 12-mm port and inserted 5 cm above the umbilicus at the right midclavicular line. The subumbilical port was then inserted under direct vision. Further 5-mm ports were inserted at the right anterior axillary line and midline under the xiphisternum as shown in Figures 1 and 2. Diagnostic laparoscopy and laparoscopic ultrasound were then performed, and lesions were located.
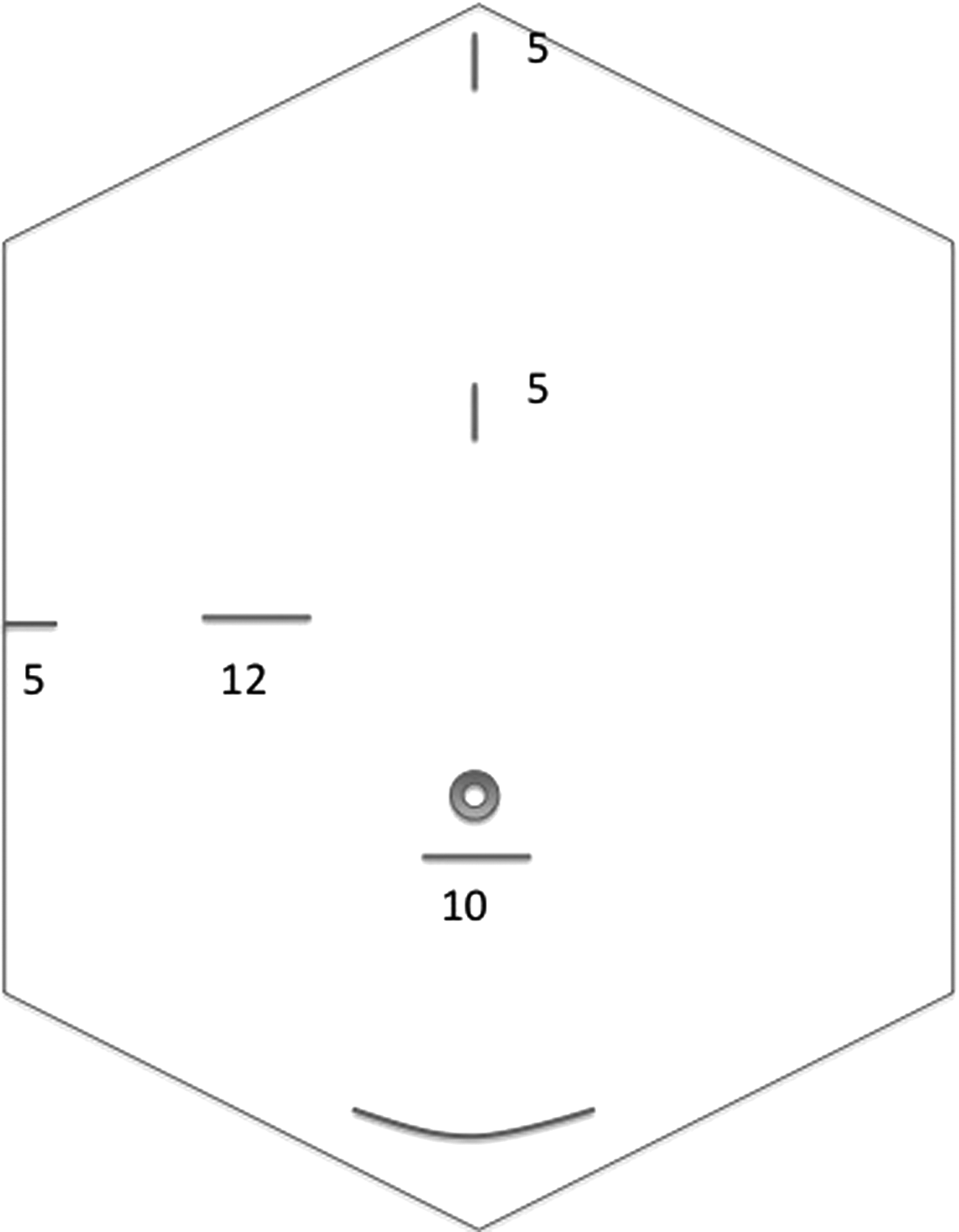
Port sites (port size is given in mm).

Clinical photograph of operative wounds.
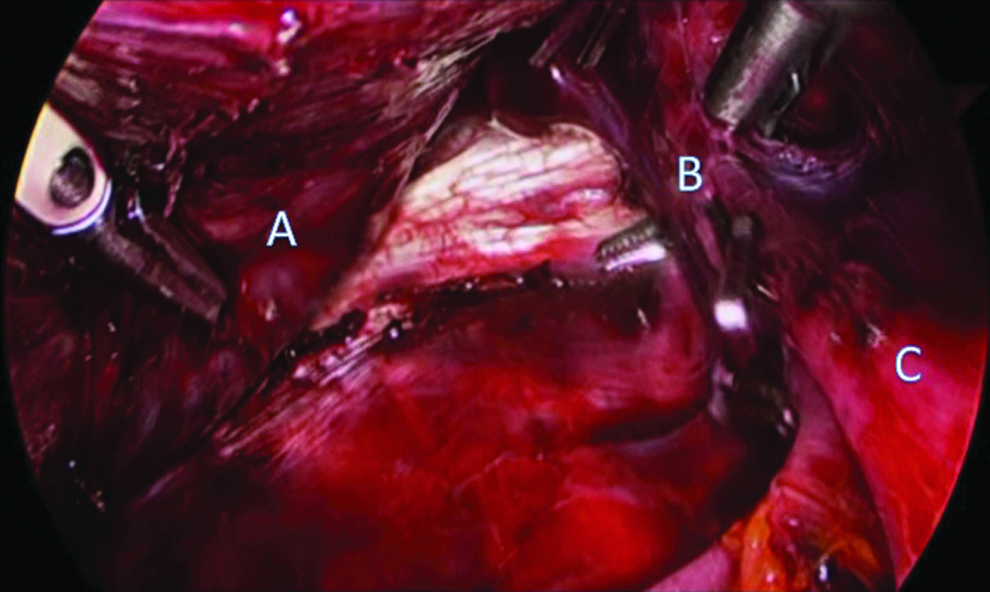
With the gallbladder resected or retracted superiorly, the right posterior Glissonian pedicle was then approached via hepatotomy with a cavitron ultrasonic surgical aspirator along the fissure of Ganz (Fig. 3). The right posterior pedicle was test-clamped and then controlled with a laparoscopic stapler or Weck® Hem-o-lok® ligation system (Teleflex®, Morrisville, NC). The right lobe of the liver was then dissected away from the inferior vena cava. Short hepatic veins were controlled with endoclips until the right hepatic vein was put in a sling with a vascular loop (Fig. 4). This vascular loop served to control bleeding from the right hepatic vein if massive hemorrhage occurred.

Dissection of the right posterior hepatic Glissonian pedicle. A, fissure of Ganz; B, right posterior hepatic pedicle; C, right main hepatic pedicle.
Dissection of the right hepatic vein. A, right lobe of the liver; B, right hepatic vein sling by right angle dissector; C, inferior vena cava.
The right lobe of the liver was now retracted and fully mobilized by division of the right triangular ligament. The parenchymal transection was then performed along the line of ischemia with the combination of the cavitron ultrasonic surgical aspirator and Harmonic® shears (Ethicon Endo-Surgery, Cincinnati, OH). After the terminal branch of the right hepatic vein was identified, parenchymal transection was completed along and to the right of the right hepatic vein. The right hepatic vein was preserved. Minor hemorrhage was controlled by bipolar diathermy, and large vessels were controlled with the Hem-o-lok ligation system or a laparoscopic stapler. The Pringle maneuver was not used.
The specimen was retrieved through a Pfannenstiel incision in a tissue retrieval bag (Espiner Medical, Clevedon, United Kingdom). Tissue glue (Tisseel®; Baxter, Vienna, Austria) was applied selectively. Abdominal drains were inserted as needed.
Results
During the period of May 2010–May 2014, we performed 13 laparoscopic right posterior sectionectomies. There were 12 male patients and 1 female patient with a median age of 64 years (interquartile range [IQR], 57.5–73 years). Eleven of them suffered from hepatocellular carcinoma (HCC); the remaining patient had colorectal liver metastasis. The details are listed in Table 1.
CLM, colorectal liver metastasis; HCC, hepatocellular carcinoma.
Three operations were converted to the open procedure, resulting in a conversion rate of 23%. One case was related to significant bleeding from the right hepatic vein, and the other 2 cases were related to unclear anatomy.
Median operative time was 381 minutes (IQR, 302.5–489.5 minutes), and median blood loss was 1500 mL (IQR, 300–1850 mL). The transfusion rate was 38.5% (5/13). Four of these 5 patients requiring transfusion were among the first 5 cases of the series.
The median size of the tumor resected was 3.7 cm (range, 1.5–7.5 cm), and the median resection margin was 8.7 mm (range, 3–50 mm). One of the specimen had a particularly wide margin of 5 cm because the tumor was located just posterior to the right posterior pedicle, so a large volume of normal liver was sacrificed. Four of the 13 patients (30.8%) were cirrhotic on histological examination.
There was no postoperative mortality. One patient suffered from duodenal perforation after the original operation that required relaparotomy, and this resulted in a significantly longer hospital stay (72 days). One patient suffered from ascitic leakage from a wound, and 1 patient had a minor bile leak. Both of them were treated conservatively without any radiological or surgical intervention. Median hospital stay was 7 days (IQR, 6–19.5 days).
Discussion
Laparoscopic liver resection is a technically demanding operation that requires a team of surgeons experienced in both laparoscopic and open liver surgery. With the improvement in laparoscopic instruments and growing experience in laparoscopic and liver surgery, more studies with favorable results have been reported.10–13 However, most were limited resections involving at most one or two peripheral segments (Couinaud segments 2–6). Laparoscopic resection was considered not indicated for lesions located at right posterior sections. 3
Previous studies demonstrated that anatomical resection for tumors, especially HCC, resulted in a definite survival benefit. 14 It was probably related to the characteristics of tumor spread via the portal venous system. To combine the benefits of laparoscopic surgery and anatomical resection, a proper technique for resecting a lesion located at the right posterior section should be developed for the maximal benefit of patients.
We identified some technical points in accomplishing total laparoscopic right posterior sectionectomy. First, retraction of the right lobe of the liver from the abdominal wall was best achieved by gravity with the patient in the full left lateral position. While keeping the resected liver fixed to the retroperitoneum, the gravitational pull would pull the remnant liver to expose the cut surface. Moreover, the transection plane would become vertical, facilitating liver parenchymal transection from a caudal approach. This technique was well described in one of the previous case reports from Japan. 7
Second, we aimed at anatomical resection with both inflow and outflow control. For inflow, we adopted the intrahepatic Glissonian approach as suggested by Machado et al. 15 We approached the right posterior Glissonian sheath intrahepatically, rather then dissecting it out extrahepatically. In 2 patients, we converted because of the uncertain anatomy. The reason was that our hepatotomy was too peripherally placed because we were afraid of damaging the right anterior Glissonian sheath if the dissection was too close to the hilum. Hence only segment 6 of the Glissonian branch was dissected. In subsequent patients, once the right posterior Glissonian sheath was exposed, the sheath was carefully dissected proximally toward the hilum so that the right anterior Glissonian sheath could also be exposed. It was at this juncture that we could pass a vascular loop to encircle the right posterior pedicle for temporary control.
Demonstration of the right hepatic vein was important because (1) anatomical resection was required for HCC and (2) the parenchymal transection plane for right posterior sectionectomy is not a flat plane. We tried to gain access to the right hepatic vein before parenchymal transection so that we can control it if massive hemorrhage occurs, which is a major criticism of the laparoscopic approach to right posterior sectionectomy.3,16 Parenchymal transection was performed along and to the right of the right hepatic vein. In this way, we both ensured anatomical resection and also decreased the blood loss by direct vision and controlled the draining veins into the right hepatic vein without damaging the main right hepatic vein itself. Nonetheless, venous connections to the right anterior liver segments could not be totally controlled, and we had one conversion because of this complication. To further decrease hepatic vein bleeding, we used the strategy of variable intraperitoneal pressure as we used during hemihepatectomy. 17
Our conversion rate was 23%, and all were performed in the early stage of our experience. Our conversion rate was comparable to previous reports for laparoscopic major hepatectomies.18–20 In a study by Pearce et al., 19 the conversion rate for laparoscopic right hepatectomy decreased from 36% to 6% with increasing experience. Our previous case series of our first 100 cases of laparoscopic hepatectomy also showed similar improvement of conversion rate from 14% for the first 50 cases to 2% for the latter 50 cases. 9 We believe that our experience in laparoscopic right posterior sectionectomy was still in the middle phase of the learning curve and that the conversion rate would improve with experience.
One patient had experienced duodenal perforation after the operation that resulted in a significantly longer hospital stay for this patient (72 days). He was managed successfully with a second laparotomy, and there were no other long-term consequences. However, this patient reminded us that despite having well-experienced laparoscopic surgeons, we should not forget the importance of meticulous technique during the operation and the risk of injury to other organs outside of our visual field during laparoscopy.
On the other hand, laparoscopic hepatectomy for malignant tumors, especially HCC, had two other problems. First, these patients were mostly hepatitis carriers with a cirrhotic background, which results in more bleeding and difficult retraction during laparoscopic liver resection. On the other hand, for HCC, anatomical resections had better prognosis. 5 The application of anatomical right posterior sectionectomy was essential for HCC located in the right posterior section.
Previous studies showed that laparoscopic resection of HCC over posteriosuperior segments resulted in longer operative time and longer hospital stay, along with a tendency toward a higher rate of conversion and greater blood loss. 21 The large parenchymal transection surface for right posterior sectionectomy predisposes to more bleeding. Our study concurred in the concern for blood loss in laparoscopic right posterior sectionectomies as the right hepatic veins or its branches were difficult to visualize and control laparoscopically. Recently, we have started to insert one or two more ports in the right 10th intercostal space so that we could have a better visualization of the right hepatic vein where we were dissecting toward the inferior vena cava. In our series, the amount of blood loss was significant in our early experience. Apart from experience during the early learning phase, it might be contributed by the higher (30.8%) cirrhotic rate among our patients. Pringle's maneuver was not used because all of our patients had selective inflow control before parenchymal transection, and blood losses were mainly from hepatic venous branches.
Yet, there are still concerns for oncological safety. Despite the routine use of intraoperative ultrasonography, achieving a tumor-free margin in the deep portion of the liver remains a challenge, especially for posteriorly located tumors. 21 We have successfully achieved R0 resection for all patients because we strictly followed the anatomical plane along and to the right of the right hepatic vein with the guidance of frequent intraoperative ultrasonography during parenchymal transection. The price to pay is more bleeding.
Conclusions
In summary, our case series confirmed that laparoscopic right posterior sectionectomy is feasible and safe but remains a technically challenging procedure. Proper inflow and outflow control is mandatory for anatomical resection. This surgical principle should not be compromised in the era of laparoscopic hepatectomy. Further studies with larger numbers of patients and longer follow-up periods are required to delineate the benefit and appropriate case selection for laparoscopic right posterior sectionectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.