
Abstract
Abstract
Background:
Whether splenectomy is adverse or spleen preservation offers significant advantages in distal pancreatic resection is unclear. The aim was to compare the early/late clinical results and the functional outcomes in terms of quality of life (QoL) and nutrition between conventional laparoscopic distal pancreatectomy (LDP) and laparoscopic spleen-preserving distal pancreatectomy (LSPDP).
Study Design:
Clinical data and computed tomography findings of 111 laparoscopic distal resections (79 LDPs and 32 LSPDPs) between 1999 and 2012 were retrospectively reviewed. QoL was assessed by the EORTC QLQ-C30. Body mass index and biochemical tests were examined as nutritional indices. Comparative analysis was done.
Results:
The mean follow-up was 25 months. The operation time was shorter in LSPDP (127.9 minutes vs. 158.0 minutes, P < .001). The lesion size was larger in LDP (36.8 mm vs. 27.2 mm, P < .01). Mucinous cystic neoplasm (MCN) was the most common diagnosis in LDP and intraductal papillary mucinous neoplasm (IPMN) in LSPDP. Early results showed similar hospital days and infection episodes. Nonvascular complications were more frequent in LDP owing to more fluid collections (43.0% vs. 21.9%, P = .04). The ISGPF grade B/C pancreatic fistula rates were similar (27.8% in LDP vs. 25.0% in LSPDP, P = .760). Vascular complications were more frequent in LSPDP (64.5% vs. 26.0%, P < .01). Excluding some fluid collections, none required a specific treatment. Late results demonstrated no differences in nonvascular results. Vascular complications were more frequent in LSPDP (65.6% vs. 4.2%, P < .01). The vascular complications did not require any specific treatment or have any serious sequelae. There was no overwhelming postsplenectomy infection. QoL and nutritional indices showed no difference. QoL decreased at discharge and recovered from 3 months thereafter. Nutritional indices showed a similar pattern.
Conclusion:
LDP is associated with more fluid collections and LSPDP with more vascular complications, all with a minimal clinical impact. Both methods had similar functional outcomes. Either LDP or LSPDP could be performed depending on the indication and surgeon's experiences considering the comparable results.
Introduction
T
The conventional LDP includes concomitant splenectomy. However, there have been numerous reports on the potential hazards of asplenism with respect to the issues of infection and malignancy.10–12 With this background and advances in surgical techniques, laparoscopic spleen-preserving distal pancreatectomy (LSPDP) is becoming more popular. However, the advantages of preventing infection and malignancy still remain controversial, 13 and their clinical significances are unknown. Furthermore, concomitant splenectomy is not without any advantage. Conventional LDP is technically less demanding and has oncologic advantages in borderline or low-grade malignant cases.
To date, there are only limited studies that compare the results between conventional concomitant splenectomy and spleen preservation in laparoscopic distal pancreatic resection. Therefore, the aim of this study was to compare the results of LDP and LSPDP in two aspects: clinical outcomes and functional/hematologic changes.
Materials and Methods
After approval from the Institutional Review Board, a retrospective review of prospectively collected protocol-based clinical data of patients who underwent LDP at the Seoul National University Hospital was conducted. According to the protocol of distal pancreatectomy at our institution, patients undergo follow-up computed tomography (CT) and various blood examinations between 5 and 7 days postoperatively and repeated examinations at outpatient clinic follow-ups at 3, 6, and 12 months. Between May 1999 and February 2012, 126 patients who underwent LDP were identified. Among them, 15 patients were excluded due to open conversions (n = 14) and a simultaneous laparoscopic colon surgery (n = 1). The remaining 111 patients were eligible for analysis, and their medical records were reviewed. Seventy-nine patients underwent LDP, and 32 patients underwent LSPDP. Among the 32 LSPDPs, splenic vessels were preserved in 9 cases and were sacrificed in 23. There was a trend toward LSPDP in the latter half of the cases (22/56) compared to the earlier experiences (10/55) with statistical significance (39.3% vs. 18.2%, P = .014). Among the LSPDPs, there was a trend toward splenic vessel sacrification in more recent experiences (15/16) compared to the earlier experiences (8/16), which also demonstrated significant differences (93.7% vs. 50.0%, P = .006).
During LSPDP, omentectomy is carried out along gastroepiploic vessels until the first visual contact with a vessel branching toward spleen to preserve as many short gastric vessels as possible even in splenic vessel–preserving LSPDP. This is to prevent caudal splenic infarction.
All patients routinely had one Jackson–Pratt drain inserted to cover the splenic fossa and the resection margin. The amylase level of drained fluid was routinely measured on postoperative days 1, 3, and 5 to evaluate pancreatic fistula grade. The drain was removed after a routine CT scan on postoperative day 5 if there was no evidence of fluid collection on CT scan, and the fluid amount was less than 100 mL per day without excessive elevation of amylase level.
All these patients received vaccination against Pneumococcus and Haemophilus either before or after the surgery. Baseline data, such as demographic data (age, sex, diagnosis, and tumor size) and operative data (elapsed time, estimated blood loss, and intraoperative transfusion), were gathered. Patients who could not be followed up as the protocol were excluded from the analysis of late complications (n = 6).
Clinical outcomes
For clinical outcomes, early and late complications were investigated. Early complication included infection episodes, including overwhelming postsplenectomy infection (OPSI), nonvascular complications (bleeding, fluid collection, and pancreatic fistula), and vascular complications, such as portal vein (PV) thrombosis, splenic vein (SV) thrombosis, splenic artery/vein stricture, perigastric varices, collateral formation, and splenic infarction (Fig. 1). The late complication, which was defined as complications occurring after more than 3 months of operation, was also divided into nonvascular and vascular complications. The late nonvascular complication focused on endocrine/exocrine function (diabetes mellitus [DM], diarrhea, steatorrhea, and body weight change), late-onset OPSI, and recurrence. The vascular complications were assessed by an experienced radiologist specializing in the hepatobiliary–pancreas system with 3 mm thickness slice CT. Early vascular complications were investigated with CT images taken between 5 and 7 days after the operation, and the late complications were based on CT images taken after 3 months of the operation (usually 6 months). Any evident change in CT images from preoperative CT images was considered as complication regardless of the presence of clinical symptoms or clinical significance. Vague changes or findings that may be confused with CT artifacts were not considered as vascular complications.
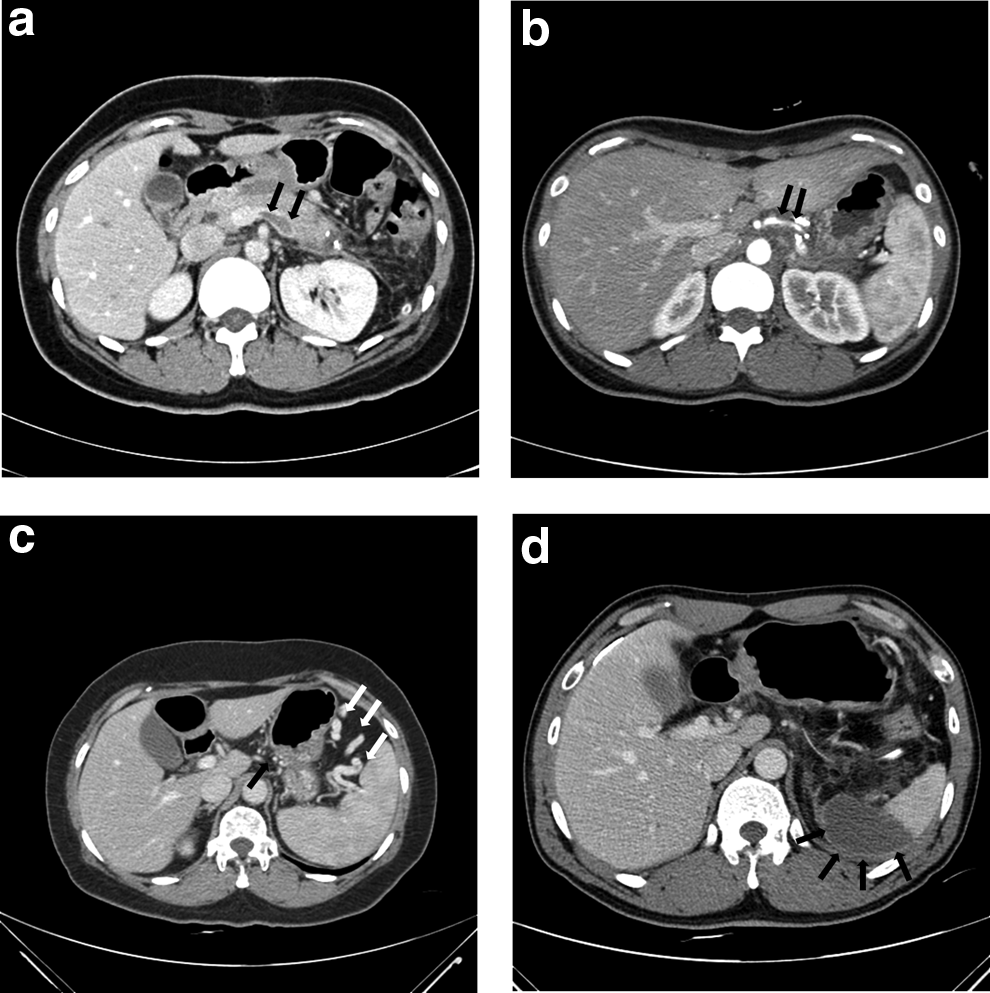
Vascular complications associated with laparoscopic distal pancreatic resections are shown.
Functional and hematologic changes
For functional and hematologic changes, quality of life (QoL), nutritional indices, and hematologic changes were investigated. The QoL was assessed using the European Organization for Research and Treatment of Cancer (EORTC) QLQ-C30 questionnaire. 14 The questionnaires were self-reported by patients, but a trained nurse assisted anyone who was unable to complete the questionnaire. The raw data underwent linear transformation to standardize the raw scores, ranging from 0 to 100, as recommended in the EORTC QLQ-C30 scoring manual. The QoL survey was conducted preoperatively, at discharge, and then at 3, 6, and 12 months in 62 patients of the study population (40 LDPs and 22 LSPDPs).
Changes in body mass index (BMI) and serum biochemical profiles, including protein, albumin, transferrin, and prealbumin, were used as nutritional indices. The values were measured before surgery, at discharge, and then at 3, 6, and 12 months. Four patients took pancreatic enzyme replacement medication up to 3 months for subjective indigestion, but none of the patients required pancreatic enzyme afterward.
Hematologic changes were examined using white blood cell (WBC) and platelet counts before surgery, at 5 days postoperatively, and then at any period between 6 and 12 months depending on the patients' visit to clinic.
Statistical analysis
Continuous variables are presented as mean ± SEM. Continuous variables were compared using the independent the Student's t-test, and categorical variables were compared by means of the χ2 test. P values less than .05 were considered statistically significant. Statistical analysis was carried out using SPSS® 18.0 software (IBM, Armonk, NY).
Results
Demographic and operative data
The mean age of the patients was 50.0 ± 1.4 years, and female predominance (68.5%) was observed (Table 1). The mean follow-up period of the patients was 25 ± 2 months. The mean BMI was 23.8 ± 0.3 kg/m2, and DM was found preoperatively in 11.7% of the patients. None of these variables was different between the LDP and LSPDP groups. However, the size of tumor (mean: 34.0 ± 1.7 mm) was significantly smaller in the LSPDP group than in the LDP group (27.2 ± 1.9 mm vs. 36.8 ± 2.2 mm, P = .001). Although the rates of malignancy, including pancreatic cancer and neuroendocrine tumor, were not different between the LDP and LSPDP groups (22.8% and 15.6%, respectively, P = .399), the distribution of diagnosis was different (P = .038). LDP was done more frequently in mucinous cystic neoplasms and solid pseudopapillary neoplasms, and LSPDP was more frequently performed in intraductal papillary mucinous neoplasms and serous cystic neoplasms. In terms of operation, operation duration of LSPDP was significantly shorter than that of LDP (127.9 ± 7.4 minutes vs. 170.3 ± 7.5 minutes, P < .001). The length of hospital day was not different between the groups. There was one case (1.0%) of reoperation, which was due to pseudoaneurysm rupture in the preserved splenic artery.
LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy.
Clinical outcomes
Early complication
The infection episodes, such as proven pneumonia, acute pyelonephritis, and/or intraabdominal abscess formation, were more frequent in the LDP group compared to the LSPDP group but without statistical significance (15.2% vs. 3.2%, P = .102) (Table 2). There was no episode of OPSI in the LDP group. The overall immediate postoperative complication rates were similar between the groups (60.8% for the LDP group and 65.6% for the LSPDP group, P = .632). The LDP group was associated with more frequent nonvascular complications with marginal significance (48.1% vs. 28.1%, P = .054). Bleeding and pancreatic fistula rates were not different between the groups, but fluid collections with Clavien–Dindo grade 2 or higher were significantly more frequent in the LDP group (43.0% vs. 21.9%, P = .036). However, all the fluid collections resolved with only conservative management. Among the 73 patients with any grade of fluid collection, 25 patients (34.2%) had percutaneous drainage or endoscopic transgastric drainage. Between LDP and LSPDP, there was no difference in terms of intervention rate (33.9% for LDP vs. 35.3% for LSPDP, P = .917).
Fourteen infection cases in 13 patients, including 11 intraabdominal infections, 1 APN, 1 pneumonia, and 1 subcutaneous infection along drainage tube tract.
Postoperative CT was available in 104 patients.
One patient who had splenic infarction underwent splenectomy on postoperative day 10 due to splenic artery pseudoaneurysm rupture.
CT, computed tomography; LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy; OPSI, overwhelming postsplenectomy infection.
In contrast, vascular complications were more frequent in the LSPDP group (64.5% vs. 26.0%, P < .001). As was the case in nonvascular complications, none of the vascular complications required specific management.
Late complication
One hundred five patients were followed up for a median period of 25 months (Table 3). Endocrine function in terms of glucose control impairment or improvement was not different between the LDP and LSPDP groups. Glucose control impairment newly developed or aggravated in 12 patients (16.4%) in the LDP group and 4 patients (12.5%) in the LSPDP group (P = .771). Two patients of the 11 DM patients (18.2%) improved after LDP, whereas none of the 2 DM patients showed improvement after LSPDP; however, significance was not found (P = .000). None of the patients complained of diarrhea or steatorrhea. The proportions of patients who experienced weight loss or abdominal symptom were not different between the groups (P = .872 and P = .639, respectively). There was not a single case of OPSI after discharge in the LDP group. There were no evidences of recurrence during the follow-up period.
CT taken between 3 and 12 months postoperatively was available in 104 patients.
CT, computed tomography; DM, diabetes mellitus; LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy; OPSI, overwhelming postsplenectomy infection.
Of the 104 patients with follow-up CT, vascular complication was significantly more common in the LSPDP group (65.6%) than in the LDP group (4.2%, P < .001). This was due to more frequent perigastric varices (28.1%), collateral formation (53.1%), and splenic infarction (6.3%) after LSPDP. The late vascular complication did not require any specific treatments and did not lead to any sequelae.
Functional and hematologic changes
The general trend of QoL evaluated through the EORTC QLQ-C30 questionnaire showed a rapid decline after operation and recovery to baseline at 3-month period and thereafter. This trend was observed in both the LDP and LSPDP groups. The global health status/QoL score showed no difference between the LDP and LSPDP groups (Fig. 2).
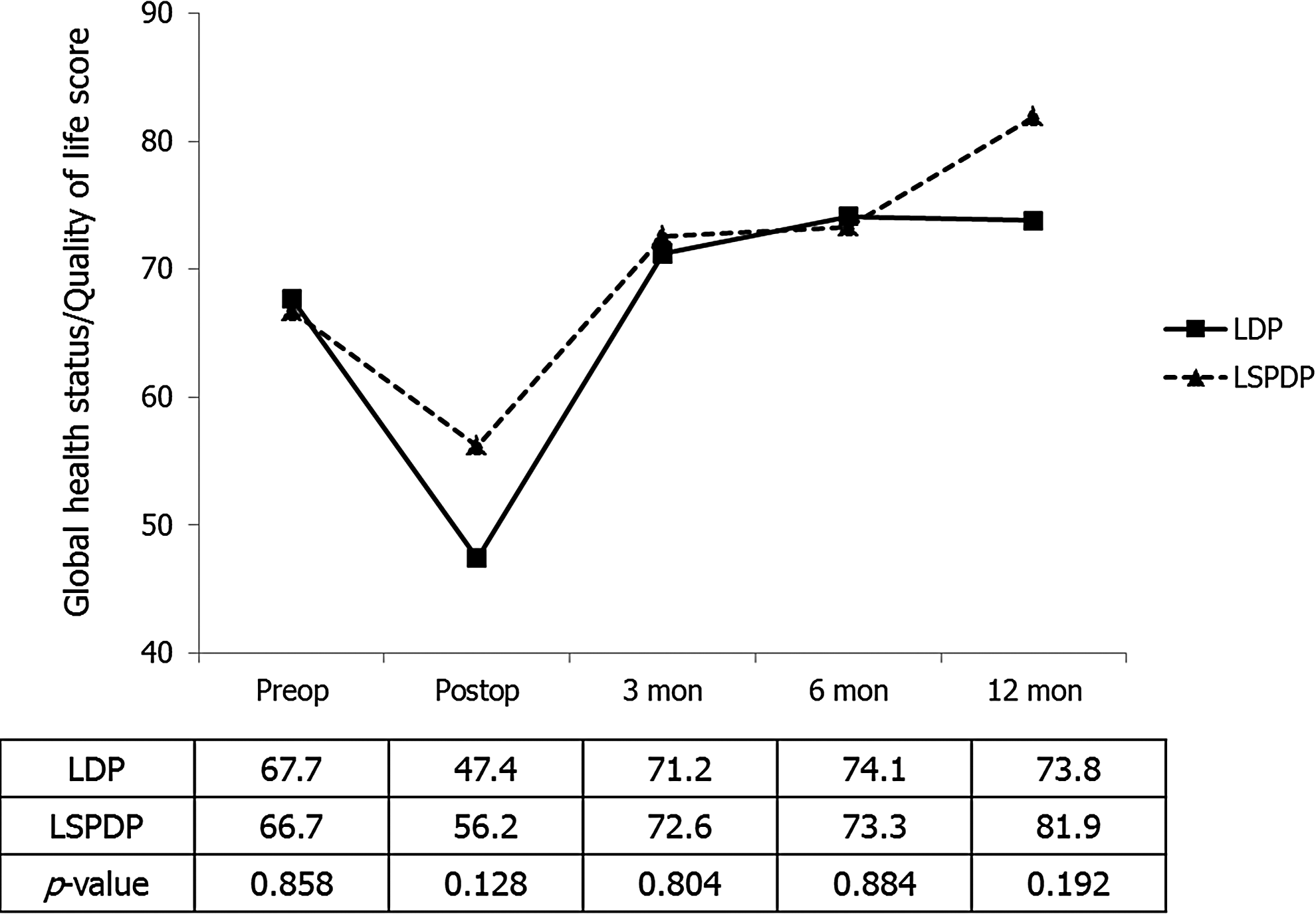
The trend of patients' conceived quality of life, as evaluated by the EORTC QLQ-C30 questionnaire, is illustrated. The scores were not different at any point of evaluation. LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy.
In terms of nutritional indices, the mean change in BMI was not different between the LDP and LSPDP groups before surgery, at discharge, and at 3, 6, and 12 months (Fig. 3). Other biochemical profiles, such as protein, albumin, transferrin, and prealbumin, showed similar patterns with the QoL scores (Fig. 4). There were no differences between the LDP and LSPDP groups at any time point.
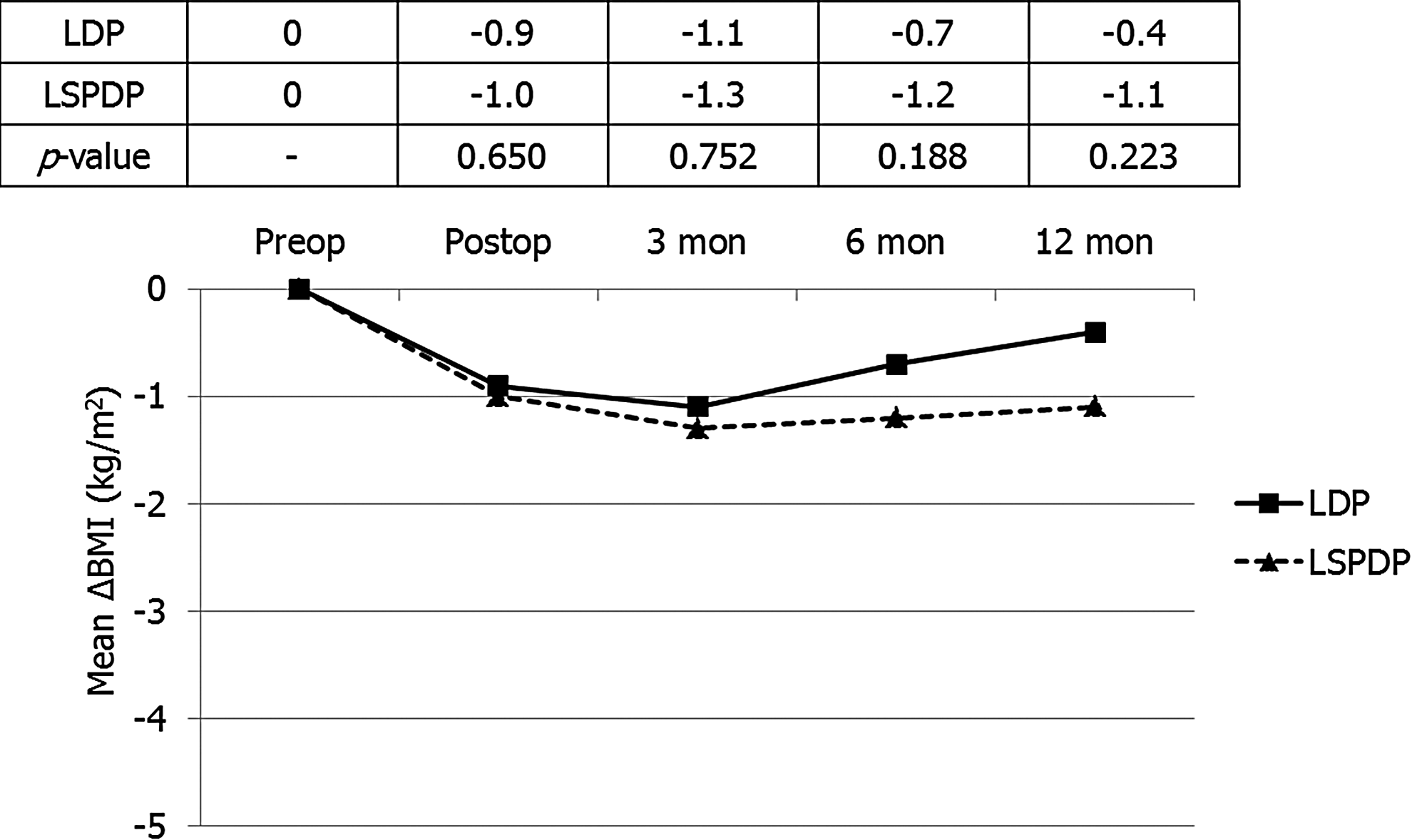
The mean change in body mass index at interval periods of the LDP and LSPDP groups shows no significant differences at any time point. LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy.
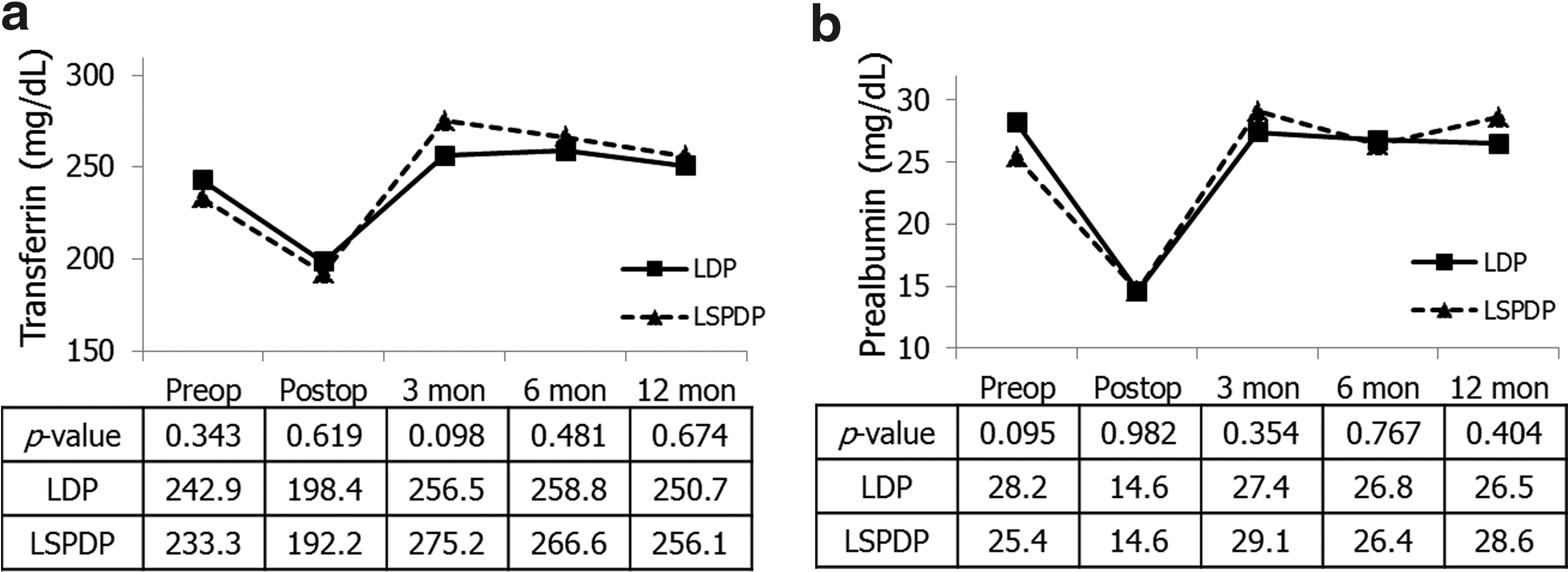
The change in nutritional biochemical profiles over time showed similar trends, and the differences between the LDP and LSPDP groups were not significant or clinically negligible.
Hematologically, WBC counts tended to rise at postoperative day 5 and then decline after 6 months in both the LDP and LSPDP groups. However, the mean elevated level postoperatively (10,400 vs. 7800 cells/mm3, P < .001) and the mean recovered level after 6 months (7400 vs. 5500 cells/mm3, P = .001) were significantly higher in the LDP group (Fig. 5a). The platelet count was significantly elevated at postoperative day 5 and remained elevated after 6 months in the LDP group, whereas it remained close to the baseline in the LSPDP group. The platelet count was significantly higher in the LDP group postoperatively (323,000 vs. 222,000 cells/mm3, P < .001) and after 6 months (312,000 vs. 189,000 cells/mm3, P < .001) compared to the LSPDP group (Fig. 5b).

The trend and differences of (
Differences among SPDPs in relation to splenic vessel preservation
Among the 32 LSPDPs, splenic vessel–preserving LSPDP (sp-LSPDP) was performed in 9 patients (28.1%) and splenic vessel–sacrificing LSPDP (ss-LSPDP) in 23 patients (71.9%). Demographics, in terms of age, sex, BMI, preoperative DM, size, and distribution of diagnosis, were not different between the groups (P = .945, .681, .125, .490, .308, and .207, respectively). The estimated blood loss (250.0 mL for sp-SPDP vs. 182.5 mL for ss-SPDP, P = .444) and the need for transfusion (0% in sp-LSPDP vs. 4.3% in ss-LSPDP, P = 1.000) were also not different. However, the operation duration was significantly shorter in ss-LSPDP than in sp-LSPDP (118.6 minutes vs. 151.7 minutes, P = .043).
The infection rates were not different with only 1 episode of intraabdominal abscess in ss-LSPDP (4.3%, P = 1.000), and there were no episodes of OPSI. The rates of early nonvascular complications, which include postoperative bleeding, complicated fluid collection, and pancreatic fistula, were equivocal between sp- and ss-LSPDP (11.1% vs. 34.8%, P = .383). Late complications were also not different in terms of aggravated glucose control (P = .303), weight loss (P = .237), and abdominal discomfort/pain (P = 1.000).
The early vascular complication rate was higher in ss-LSPDP (72.7%) compared to sp-LSPDP (55.6%), but it was not significant (P = .417). The higher vascular complication rate was due to more frequent splenic infarct in ss-LSPDP (45.4%) than in sp-LSPDP (11.1%, P = .106). In terms of late vascular complications, ss-LSPDP had a higher complication rate (82.6%) than sp-LSPDP (25.0%) with statistical significance (P = .006). The frequencies of PV and SV thrombosis, SV stricture, perigastric varices, and splenic infarct were comparable between the two methods. However, collateral formation was by far more frequent in ss-LSPDP (69.6%) compared to sp-LSPDP (12.5%, P = .011), resulting in significantly higher late vascular complication rate of ss-LSPDP.
Discussion
Whether spleen preservation is worthwhile is still controversial. The proponents of spleen preservation asserted on reduced risk of OPSI, infection, malignancies, hematologic disorder, and DM after spleen preservation.15,16 In contrast, opponents of spleen preservation pointed out technical intricacy, time consumptiveness, and increased blood loss as a shortcoming of spleen preservation. 17 While most of the reports comparing distal pancreatectomy and SPDP were on open surgery,10,18–21 there are now a couple of articles investigating the role of spleen preserving in laparoscopic distal pancreatic resection.13,22
Zhao et al. 13 concluded that LSPDP is safe and feasible with comparable morbidity and outcome to the conventional LDP through a review of clinical outcomes focusing on morbidities. Choi et al. 22 further investigated the role of spleen preservation by assessing the QoL of the patients in whom they found that patients who underwent LDP appeared to have more impairment in QoL. As surgery affects QoL considerably, we agree that other aspects than clinical outcomes should be assessed. Therefore, we compared the results of LDP and LSPDP in various aspects in an effort to find a superior method. We assessed and compared with respect to early and late clinical outcomes, QoL, nutritional indices, and hematologic changes.
The early clinical outcome of this study shows that LDP yields more nonvascular complications, whereas LSPDP yields more vascular complications. The high incidence of nonvascular complications of LDP is due to higher incidence of fluid collections. This is thought to be due to more space formed in the left upper quadrant by removing the spleen. In contrast, vascular complication was higher in LSPDP, as shown in Table 2. However, LDP is not without any vascular complications. LDP was more frequently associated with PV and SV thrombosis. At any rate, all the fluid collections resolved with only conservative management (with or without percutaneous drainage), and none of the vascular complications required specific management. Therefore, the early clinical outcome shows that both methods have pros and cons, clinical significances of which are minimal.
The late clinical outcome showed that the two surgical methods had similar results in terms of endocrine/exocrine function, OPSI, and recurrences. However, LSPDP was associated with more vascular complications (Table 3). Collateral formation, perigastric varices, and splenic infarct may be considered as consequences of spleen preservation in LSPDP using the Warshaw's technique rather than a true complication. Furthermore, none of the cases needed a specific treatment, and there were no related adverse sequelae, such as varices bleeding or splenic necrosis.
Of the vascular complications, unexpectedly high incidence of PV and SV thrombosis was noted in the early clinical results. During a routine CT taken at postoperative 5–7 days, a total of 10.6% and 16.3% of PV thrombosis and SV thrombosis were noted. All but one case occurred in the LDP group. This may be due to stagnation of blood flow in the remnant SV stump and elongation or thromboembolism from the SV thrombosis. In particular, thrombocytosis was more common in the LDP group, which may result in further hypercoagulable state. These two factors may have a synergistic effect to form thrombosis. A recent study noted 6% incidence of PV thrombosis after LDP with concurrent splenectomy. 23 However, in this study, patients did not have a routine CT check postoperatively, and patients were examined only after symptom development, which may lead to underreporting of asymptomatic PV thrombosis. All the patients in this study were asymptomatic. Considering the 2.9% PV thrombosis rate in the late clinical results, which is comparable to the 6% of the results of the Mayo Medical Center, 23 there is a possibility of high incidence of undetected PV and SV thrombosis after LDP.
The result of the EORTC QLQ-C30 questionnaire indicated that the perceived QoL was not different at all time points between the LDP and LSPDP groups. Choi et al. 22 demonstrated a better QoL after LSPDP through a survey. However, this survey was self-developed, and its internal and external validations were not done. To overcome this shortcoming, a validated questionnaire developed by the EORTC was used in the study. In addition, the questionnaire was done at various periods to assess the QoL in the short and long terms.
Along with the perceived QoL, various nutritional indices were examined to evaluate functional changes. The mean BMI decreased after surgery in both groups. The BMI of the LDP group showed a slow recovery, but that of the LSPDP group showed a little recovery. However, the statistical significances were not found. Nutrition-related biochemical profiles were investigated. All biochemical markers, which include protein, albumin, transferrin, and prealbumin, showed a similar pattern: decreased level at discharge and recovered level from 3 months and beyond. This pattern was equally observed in both groups. Therefore, it may be carefully concluded that the biochemical profiles do not differ between the LDP and LSPDP groups.
Hematologic evaluation through WBC and platelet counts demonstrated that the WBC counts fluctuated to a lesser degree and the platelet counts were maintained at a similar level in LSPDP. In contrast, the WBC counts fluctuated to a greater degree and the platelet counts was elevated and maintained at a higher level in LDP patient. This shows that LSPDP offers a better hematologic stability over LDP in statistics. One practical disadvantage of hematologic instability may be confusion in postoperative care. Fever is often accompanied in the immediate postoperative period, and the excessively elevated WBC may warrant unnecessary radiologic examinations and antibiotics. Another theoretical disadvantage may be the risk of thrombosis in patients with thrombocytosis. However, the actual clinical significance of hematologic stability remains to be uncovered.
In addition, the proponents of spleen preservation often mention the superior immunity and less vulnerability to infection.10,16,22 However, our results showed that infection rates were insignificant at both early and late periods, and there were no cases of OPSI. However, it must be added that, even though the infection rate was statistically insignificant, 12 of the 13 infection episodes occurred in the LDP group (infection rate of 16.4%), whereas only one episode occurred in the LSPDP group (3.2%). However, as 11 episodes are intraabdominal infections, they are most likely associated with a higher rate of intraabdominal fluid collections in LDP, which makes the interpretation of this result difficult. To better grasp the effect of splenectomy on infection, more basic science research and well-designed clinical investigation are needed.
In contrast, opponents of spleen preservation claim a shorter operation time with concomitant splenectomy. 17 The mean elapsed operation time in this study was shorter in LSPDP. One possible explanation is the simplicity of the Warshaw's technique, which does not require splenic vessel preservation. Another is the effect of selection bias since LSPDP is performed in much simpler diagnosis and lesions leading to less complicated operation. Anyhow, the time disadvantage of LSPDP should not be taken into consideration anymore.
Whether vessel preservation in SPDP is an important issue has been under debate for a long time since Warshaw's publication 24 on splenic vessel ligation proximally and distally. Beane et al. reported that the splenic vessel–preserved group had advantage over conventional distal pancreatectomy, whereas the splenic vessel–sacrificed group provided no short-term advantage over conventional distal pancreatectomy. 25 A subgroup analysis in the current study revealed no significant difference between vessel-preserved and vessel-sacrificed groups except for splenic infarct and collateral formation, which had a minimal clinical impact. However, the current study has only a limited number of vessel-preserved LSPDPs compared to the matched population of Beane et al. In addition, unlike the study by Beane et al., only laparoscopically operated patients were taken under consideration, which may result in different results. Further study is needed to weigh the clinical implication of vessel preservation in SPDP.
In summary, the early clinical outcome can be said to be equivocal as each of the methods has its strengths and weaknesses. The perceived QoL and the nutritional indices were also equivocal in both methods. LDP was superior in terms of late outcome with fewer complications, but the clinical significance of the late vascular complications after LSPDP is very low. In contrast, the LSPDP group was hematologically more stable than the LSPDP group, but the clinical significance is not evident (Table 4).
LDP, laparoscopic distal pancreatectomy; LSPDP, laparoscopic spleen-preserving distal pancreatectomy; WBC, white blood cell.
The limitation of this study is the retrospective nature. In addition, the heterogeneity of the LDP and LSPDP groups resulting from the difference in indication in selecting operative method limits the generalization of the current results. Furthermore, because the indicative diagnoses of LDP are relatively benign in nature, the follow-up periods are rather short. Thus, future study assessing the true long-term results is needed.
In conclusion, LDP and LSPDP have each of their own advantages and disadvantages. The clinical and functional outcomes are similar. Furthermore, the clinical importance of the disadvantages of each method is deemed to be minimal. Therefore, the use of either technique may be feasible, and the selection of method can be determined by the diagnosis, tumor location, associated inflammation, and the surgeon's experiences.
Footnotes
Acknowledgment
This study was supported by a grant from the National Research and Development Program for Cancer Control, Ministry of Health and Welfare, Korea (no. 1120310).
Disclosure Statement
No competing financial interests exist.