
Abstract
Abstract
This study presents a modified surgical approach to laparoscopic myotomy for achalasia using stepped dilation with a Rigiflex balloon and contrast medium under image guidance. A 10-year-old boy with persistent dysphagia and vomiting had ingested only liquids for 3 months, losing >10 kg in body weight. Barium swallow and esophageal manometry diagnosed esophageal achalasia with mild esophageal dilatation. After failed pneumatic dilatation, laparoscopic Heller myotomy with Dor fundoplication was performed. Prior to surgery, a Rigiflex balloon dilator was placed within the esophagus near the diaphragmatic hiatus. A four-port technique was used, and mobilization of the esophagus was limited to the anterior aspect. A 5-cm Heller myotomy was performed, extending another 2 cm onto the anterior gastric wall. During myotomy, the Rigiflex balloon was serially dilated from 30 to 50 mL, and filled with contrast medium under fluoroscopic image guidance in order to maintain appropriate tension on the esophagus to facilitate myotomy, and to confirm adequate myotomy with sufficient release of lower esophageal sphincter by resecting residual circular muscle fibers. Residual circular muscle fibers can be simultaneously visualized under both fluoroscopic image guidance and direct observation through the laparoscope, and they were cut precisely until the residual notch fully disappeared. Dor fundoplication was completed. The operative time was 180 minutes, and oral intake was started after esophagography on postoperative day 1. As of the 12-month follow-up, the patient has not shown any symptoms, and his postoperative course appeared satisfactory.
Introduction
A
Case Report
A 10-year-old boy was referred to Shizuoka Children's Hospital for persistent dysphagia and vomiting. During the clinical course at a primary clinic, dysphagia occurred at every meal, and he had ingested only liquids for 3 months. During this time, his body weight decreased by >10 kg. Barium swallow revealed that the esophagus was slightly dilated, with significant stasis of contrast medium in the distal esophagus (Fig. 1). Upper gastrointestinal endoscopy showed no evidence of esophagitis or esophageal tumor. A thoracic computed tomography scan also showed no evidence of cartilage formation in the esophageal wall or mediastinal tumor. Esophageal manometry revealed an increased LES pressure (35 mmHg), lack of deglutitive relaxation of the LES, and disappearance of peristaltic contractions, with abnormal synchronized contractions (Fig. 2). Based on these findings, esophageal achalasia was diagnosed.

Preoperative esophagography. Stasis of contrast medium with a significant sump formation (open-arrowheads) is confirmed.
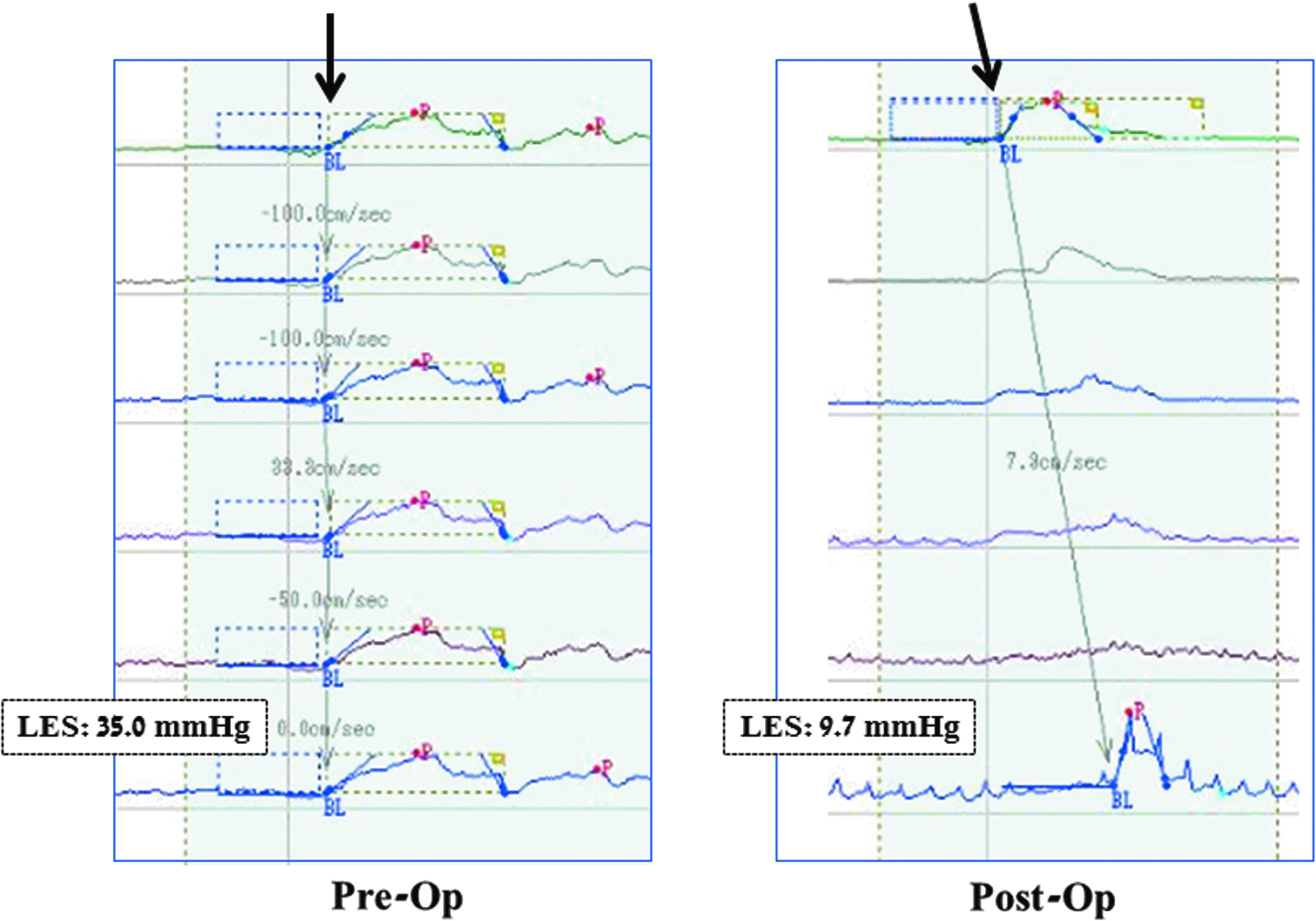
Pre- and postoperative esophageal manometry. Increased lower esophageal sphincter (LES) pressure, lack of deglutitive relaxation of the LES, and disappearance of peristaltic contractions (arrow) were revealed preoperatively (left). Decreased LES pressure, recovery of deglutitive relaxation of the LES, and normal peristaltic contractions (arrow) were confirmed postoperatively (right).
Initial treatment with pneumatic dilatation was not effective for the management of digestive symptoms, and a decision was made to perform laparoscopic Heller myotomy with Dor fundoplication. Before starting surgery, a Rigiflex balloon dilator (Microvasive, Watertown, MA) was placed within the esophagus near the diaphragmatic hiatus, with the positioning confirmed on fluoroscopy, to facilitate intraoperative esophageal myotomy and ensure sufficient release of the LES. The patient was placed in the supine position under general anesthesia, with the surgeon standing between the legs of the patient. Pneumoperitoneum was maintained at a pressure of 8 mmHg. A four-port technique was used. A 10-mm telescope was inserted through the umbilicus, 5-mm operating ports were inserted in the right and left hypochondrium, the stomach was retracted downward by an instrument inserted through a 5-mm port positioned to the left of the umbilicus, and the liver was retracted using a Nathanson retractor through a subxiphoid incision. Monopolar right-angled electrocautery and a harmonic scalpel (Ethicon Endo-Surgery, Blue Ash, OH) were primarily used in the operation; the phrenoesophageal membrane overlying the esophagus was divided, and the left and right crus were identified. Mobilization of the esophagus was limited to the anterior aspect, leaving the posterior attachments intact. Heller myotomy was performed using right-angled electrocautery and was 5 cm in length, extending another 2 cm onto the anterior gastric wall.
During the process, the Rigiflex balloon dilator was serially dilated from 30 to 50 mL, and again to 30 mL, and filled with contrast medium under fluoroscopic image guidance, to maintain appropriate tension on the esophagus to facilitate the myotomy, and also to confirm adequate length of the myotomy with sufficient release of the LES. The pressure exerted by the inflated Rigiflex balloon in mmHg cannot be calculated accurately from the volume of contrast medium used, and the volume of contrast medium required varies according to the size of the patient. Residual circular muscle fibers that may have been tethering the esophagus and could later lead to failure were simultaneously visualized under both fluoroscopic guidance and direct observation through the laparoscope (Fig. 3). These fibers were cut precisely under both 30 and 50 mL Regiflex balloon tension, until the residual notch disappeared on fluoroscopic images, even under lower tension from the Rigiflex balloon, such as 30 mL (Fig. 4). Dor fundoplication was accomplished with interrupted sutures; two rows of sutures joining the gastric fundus and divided esophageal muscle were inserted, each consisting of three stitches (Fig. 5). The operative time was 180 minutes, and blood loss was minimal.

Intraoperative fluoroscopic imaging (left) and laparoscopic view (right) of esophageal myotomy. Residual circular muscle fibers were visualized on fluoroscopic images (arrow) and laparoscopic direct view (arrow) with a Rigiflex balloon dilator pressure of 50 mL.
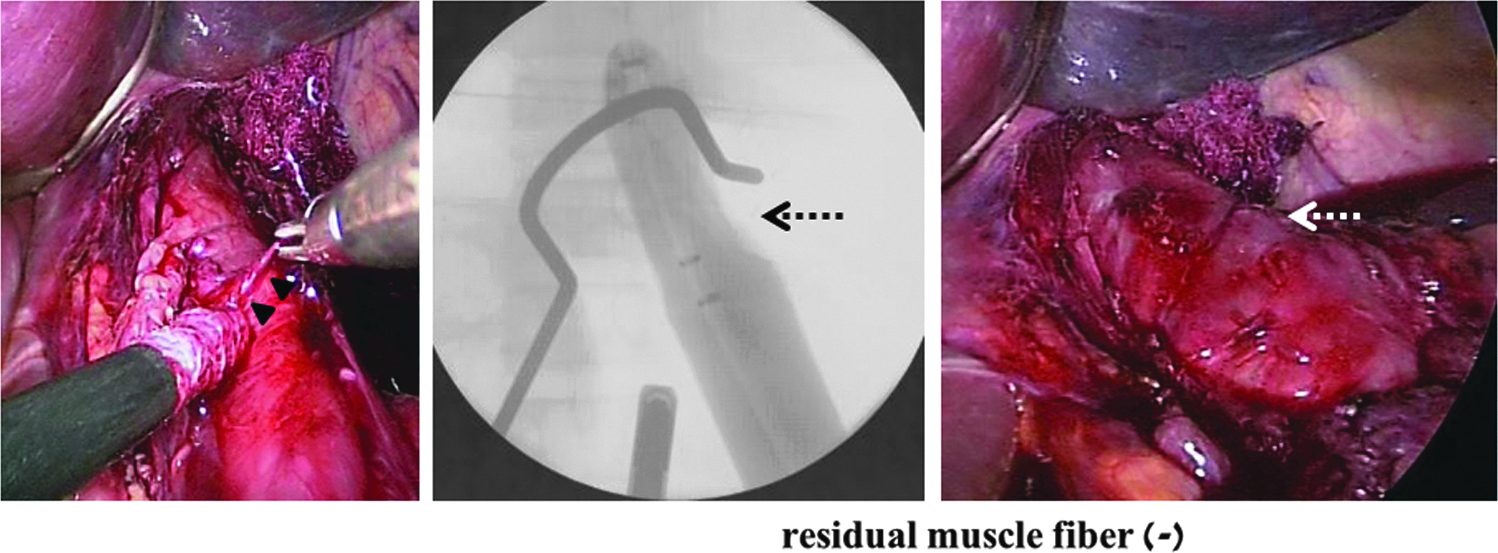
Intraoperative fluoroscopic imaging (middle) and laparoscopic view (right) of esophageal myotomy, after residual circular muscle fibers (arrowheads) cutting. After residual muscle fibers (arrowheads) were cut (left), no residual notch could be seen (dotted arrows) both in fluoloscopic imaging (middle) and laparoscopic view (right), even at low pressure, such as at 30-mL balloon dilation.
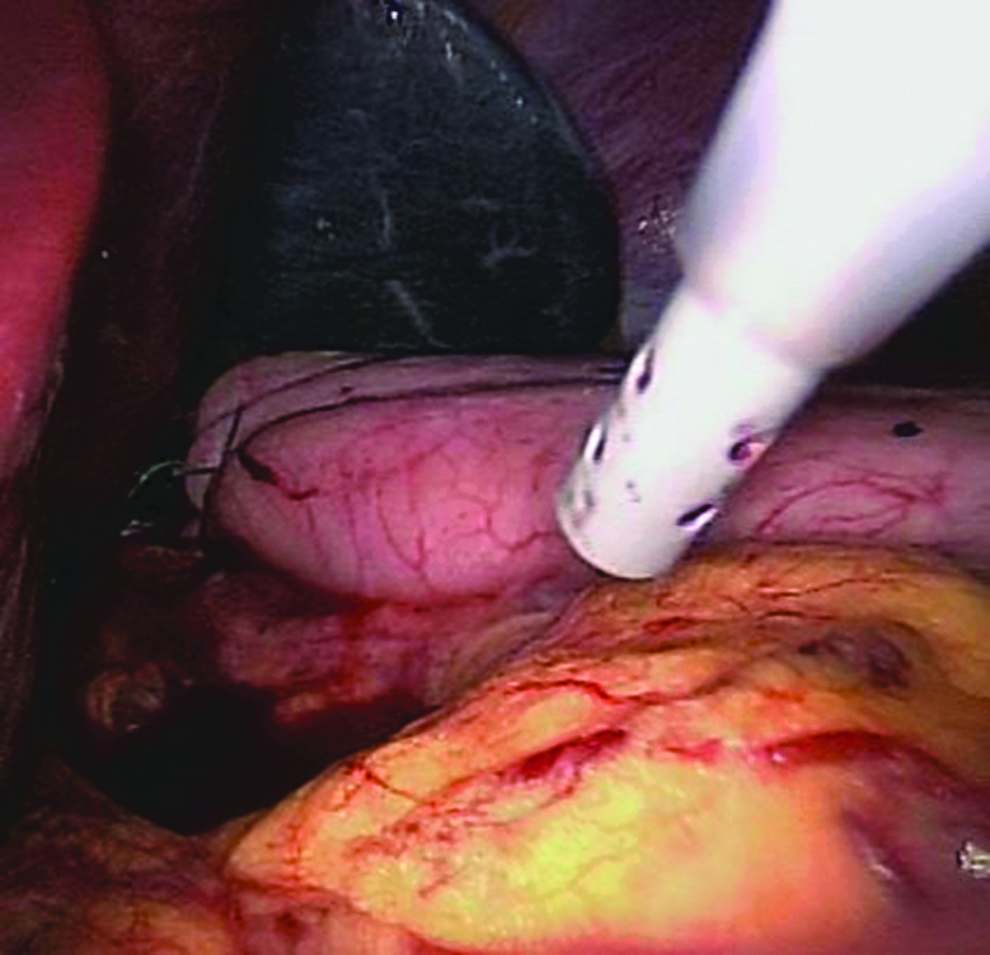
Dor fundoplication. Two rows of sutures are inserted to join the gastric fundus and divided esophageal muscle, with each row consisting of three stitches.
Passage of liquids and solids was smooth, and no gastroesophageal reflux was observed on esophagography on postoperative day 1, so oral intake was resumed after esophagography. No postoperative complications were encountered, and subjective symptoms completely disappeared. Postoperative esophageal manometry showed decreased LES pressure (9.7 mmHg), recovery of deglutitive relaxation of the LES, and normal peristaltic contractions (Fig. 2). As of the 12-month follow-up, the patient has not shown any symptoms and was satisfied with his postoperative course.
Discussion
In the treatment of achalasia, incomplete myotomy can lead to recurrent dysphagia, necessitating reoperation or pneumatic dilations. Two series have reported persistent high pressures in 34% and 45% of patients who were considered from laparoscopic and endoscopic evidence to have undergone adequate myotomy.5,6 Despite the fact that the myotomy is regularly lengthened, by as much as 4 cm to the esophagus and >2 cm to the distal gastric side, the three largest recent series of children treated with Heller myotomy reported that dysphagia occurred in approximately 25% of patients.7–9 It is therefore believed that the cause of incomplete myotomy includes not only a gastric component of the LES or inadequate dissection up the proximal esophagus resulting in residual high-pressure zones, but also residual muscle fibers that may be missed during the laparoscopic myotomy. Such muscle fibers may tether the esophagus, leading to later failure.
The use of a Rigiflex balloon dilator across the gastroesophageal junction during Heller myotomy has been reported as useful, with inflation and deflation of the balloon making the myotomy much easier and allowing better visualization and cutting of residual muscular fibers. 10 In addition, a contrast medium (gastrografin) was used instead of air to fill the Rigiflex balloon dilator, and the balloon was inflated by degrees, from 30 to 50 mL, and again from 50 to 30 mL, so that residual muscle fibers could be precisely visualized and adequate release of the LES could be confirmed both under fluoroscopic guidance and on the laparoscopic monitor.
Footnotes
Disclosure Statement
No competing financial interests exist.