
Abstract
Abstract
Background:
Thoracoscopic repair of congenital diaphragmatic hernia (CDH) has become a popular approach. As there is an ongoing discussion on whether the benefits of the thoracoscopic repair outweigh the potential side effects, we aimed to investigate the opinion and experience of the members of the International Pediatric Endosurgery Group (IPEG) on this topic.
Materials and Methods:
An online survey was conducted between October and December 2013 on behalf of the IPEG Research Committee. All 536 IPEG members were contacted by e-mail and asked to complete an anonymous questionnaire that included 28 items on the management of CDH.
Results:
One hundred sixty-one pediatric surgeons completed the questionnaire. Contraindications to thoracoscopic repair included the following: patient on extracorporeal membrane oxygenation (ECMO) (78%); preoperative need for ECMO (42%); right-sided hernia (15%); liver in chest (32%); weight <2.5 kg (35%); and persistent right-to-left shunting (41%). Fifty-two percent of participants said that during thoracoscopic CDH repair they would tolerate any pH. In contrast, 48% indicated that they would only tolerate pH/partial pressure of CO2 (pCO2) levels down/up to 7.2/80 mm Hg (range: pH, 6.9–7.3; pCO2, 55–100 mm Hg). If a patch was needed, 39% of participants said they would continue thoracoscopically, 31% would convert, and 31% stated that the decision would depend on the size of the defect. Fifty-seven percent of participants reported recurrences after thoracoscopic repair, which occurred within 6 months in 43% of the cases, after 6 months in 37%, and both before and after in 20% of the cases. Overall, 50% of surgeons stated that CDH can be repaired equally by thoracoscopy and open approaches, and 50% disagreed with this statement.
Conclusions:
Thoracoscopic CDH repair is currently being performed by 89% of all participating IPEG members. ECMO, either active or previously, and persistent right-to-left shunting are the main deterrents to thoracoscopic repair. The fact that only 50% of surgeons stated that CDH can be repaired equally by thoracoscopy and open surgery suggests that future studies should focus on identifying the appropriate patient population.
Introduction
T
The first thoracoscopic repair of children with congenital diaphragmatic hernia (CDH) was reported by Becmeur et al. 4 in 2001. The technique was initially restricted to late-onset hernias with correction far beyond the newborn period. With increasing experience, thoracoscopy was shown to be superior to the laparoscopic approach as the insufflation of the CO2 in the thoracic cavity supported the reduction of the abdominal organs.4–6 In recent years several studies comparing open versus thoracoscopic CDH repair have been published. Three retrospective studies confirmed a shorter duration of ventilation7–9 and lower postoperative partial pressure of CO2 (pCO2) in patients who underwent thoracoscopy. 7 A retrospective comparative study demonstrated thoracoscopy resulted in shorter time to full feeds, less postoperative analgesia, and less severe complications, resulting in lower hospital charges. 7
These series emphasize the feasibility of the thoracoscopic approach; however, the heterogeneous patient selection criteria and lack of long-term outcomes leave its role undefined. Several studies on thoracoscopic procedures used historic controls and reported on faster recovery and equivalent recurrence rates. In contrast, a systematic review and meta-analysis of thoracoscopic cases found higher recurrence rates and longer operation time, compared with open surgery. 10
Some authors have recently questioned the safety of thoracoscopic CDH repair. Emerging evidence suggests that thoracoscopy in neonates could produce severe acidosis and brain hypooxygenation that could potentially impair neurologic development. 11 It is currently unclear if the benefits of thoracoscopy outweigh the potential risks. In this study, we aimed to assess the current management strategies and the opinion and experience of the members of International Pediatric Endosurgery Group (IPEG) with thoracoscopy in children with CDH.
Materials and Methods
The survey was conducted between October and December 2013 on behalf of the IPEG Research Committee using an online provider for Web-based surveys (SurveyMonkey™ [www.SurveyMonkey.com]). All IPEG members (n = 536) were contacted by e-mail and invited to complete an anonymous questionnaire that included personal background and 28 items on the management of CDH. The invitation was sent out by e-mail with an embedded link to connect to the survey. Three reminder messages were sent during a 3-week period. Trainees/fellows were excluded from the study. A completion of all 28 items was not mandatory if the question did not apply to the respondent's practice.
The first section of the survey assessed professional background, including type of institution and volume of CDH cases. The second part assessed preoperative management of CDH, including ventilation, drugs, and extracorporeal membrane oxygenation (ECMO). The last part of the survey assessed the surgical treatment of CDH and the management of complications.
Statistical analysis
Answers were anonymously collected, converted into a database with Microsoft (Redmond, WA) Office Excel™ (version 2010), and analyzed using descriptive statistics. Fisher's exact test was performed to compare categorical variable frequencies.
Results
General information on the surgeon and the treating institution
The online questionnaire was completed by 161 of 536 (30%) IPEG members from North America (n = 87; 54%), Europe (n = 34; 21%), Asia (n = 21; 13%), Australia (n = 8; 5%), South America (n = 9; 6%), and Africa (n = 2; 1%). Their primary practice setting was a university hospital (n = 127; 79%), community hospital (n = 19; 12%), private hospital (n = 12; 7%), or “other” hospital (n = 3; 2%). Over the past 12 months preceding the survey, 23 of 161 respondents (14%) had operated on 0–2 CDH cases, 54 participants (34%) on 3–5 CDH cases, 45 surgeons (28%) on 6–9 patients with CDH, and 39 participants (24%) on 10 and more CDH cases.
Preoperative protocols for mechanical ventilation and ECMO
The routine initial ventilation type for newborns with CDH is pressure-cycled mode for 106 of 160 surgeons (66%) and high-frequency oscillatory ventilation for 45 (28%), whereas 9 (6%) use other ventilation techniques.
The treatment with ECMO is available for 103 of 161 surgeons (64%), whereas 58 (36%) have no possibility of ECMO at their institution. Regarding a potential weight limit for considering a child for ECMO, 91 of 138 respondents (66%) stated that they have a weight limit of 2 kg, 14 (10%) used a weight limit other than 2 kg, and 33 (24%) considered any patient for ECMO. If a patient is put on ECMO, 70 of 145 surgeons (48%) use a venoarterial technique, and 29 (20%) use a venovenous technique, whereas the type of ECMO is not predefined for 46 (32%). In the case that a patient cannot be weaned from ECMO, 21 of 141 respondents (15%) routinely, 74 (52%) occasionally, and 46 (33%) never perform a CDH repair with simultaneous ECMO.
Drugs in CDH management
Preoperatively, surfactant is applied routinely by 33 of 160 participating surgeons (21%) and in selected patients by 76 (48%). The following drugs to reduce persistent pulmonary hypertension are routinely used: nitric oxide (n = 58; 36%), 5-phosphodiesterase inhibitors (e.g., sildenafil) (n = 19; 12%), and prostaglandins (n = 5; 3%).
Those drugs are used in selected patients only as follows: nitric oxide (n = 89; 56%), 5-phosphodiesterase inhibitors (e.g., sildenafil) (n = 103; 64%), and prostaglandins (n = 96; 60%).
Thoracoscopic repair of CDH
Frequency of usage and contraindications
Thoracoscopic repair of CDH is performed routinely by 64 respondents (40%), occasionally by 79 (49%), and never by 18 (11%). The contraindications that the participants consider for thoracoscopic repair are listed in Figure 1.
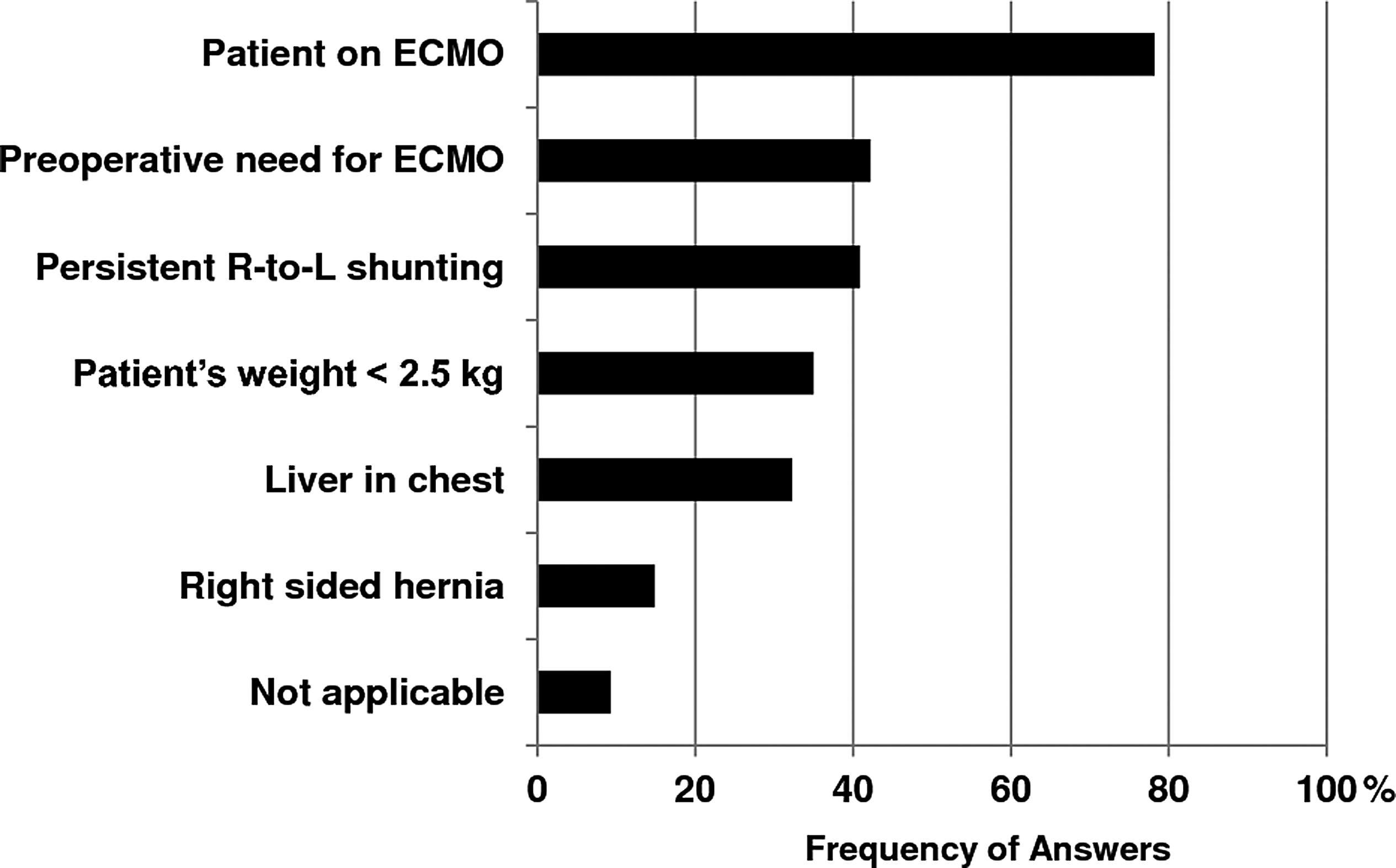
Answers to the question “What do you consider as contraindications for thoracoscopic repair? (Choose all that apply).” ECMO, extracorporeal membrane oxygenation; R-to-L, right-to-left.
Insufflation pressure and intraoperative monitoring of potential hypercapnia and acidosis
The initial pressure level for CO2 insufflation during thoracoscopy is 1–2 mm Hg for 20 of 155 (13%), 3–4 mm Hg for 92 (59%), 5–7 mm Hg for 38 (25%), and 8 mm Hg and higher for 5 (3%) participants.
In response to the question of “During thoracoscopy, what is the lowest pH and CO2 that you believe is tolerable?” 77 of 148 participants (52%) answered that the pH did not influence them, and 75 (51%) of surgeons stated that they tolerate any level CO2 intraoperatively. In contrast, 71 (48%) of participants said that they have a certain level of pH, and 73 (49%) have a level of pCO2, that they consider their lowest/highest tolerable value.
One hundred fourteen of 157 respondents (73%) stated that recent reports on significant hypercapnia and severe acidosis during thoracoscopic CDH repair made them change their management. Fifty-one participants (32%) responded that they now consider different patients suitable for CDH repair, 54 (34%) said that they now use lower starting pressures or converted earlier to open repair, and 6 participating IPEG members (4%) stopped performing thoracoscopic CDH repair.
Patch repair
If the size of defect will require a patch, 60 of 154 respondents (39%) continue to repair thoracoscopically, 47 (31%) convert to an open procedure, and 47 (31%) make this decision based on the size of defect. In case of conversion, 114 surgeons (74%) convert to laparotomy, and 40 (26%) convert to thoracotomy.
The patch material use is heterogenous; 139 of 161 respondents (86%) use nonabsorbable meshes (polytetrafluoroethylene [Goretex]), polypropylene [Marlex], polyethylene terephthalate [Dacron], and silicone [Silastic]), and 38 (24%) repair the defect with biosynthetic materials (e.g., Surgisis, SIS, Alloderm, LifeCell). Abdominal wall muscle flaps (e.g., internal oblique and transversalis abdominal muscles) are fashioned by 13 surgeons (8%), and 3 (2%) use thoracic wall musculature (e.g., latissimus dorsi and serratus anterior muscles).
Several authors suggested that the placement of a patch in a dome-shaped fashion has advantages. In the current survey 61 of 161 respondents (38%) stated that these reports have affected their technique, whereas 100 surgeons (62%) are influenced.
Recurrence after thoracoscopic CDH repair
The majority of 144 respondents (n = 82; 57%) had experienced recurrence. Of the last five thoracoscopic CDH repairs by each participant, the following recurrence rates were reported: none (n = 65; 45%), one (n = 51; 35%), two to four (n = 8; 6%), and five (none). Twenty respondents (14%) stated they could not remember their recurrence rate. Recurrences occurred within 6 months in 46 of 107 cases (43%), after 6 months in 40 (37%), and both before and after 6 months in 21 (20%).
Quality of CDH repair
Overall, 79 of 158 surgeons (50%) stated that CDH can be repaired equally by thoracoscopy and open thoracotomy, and 78 (50%) disagreed with this statement.
Other intraoperative aspects
In case of a hernia sac, 125 of 161 participants (78%) resect the sac, and 36 participants (22%) leave it in place. The preferred suture materials were Ethibond/Mersilene (66%), Prolene (16%), and silk (14%). Less frequently used sutures are Vicryl, PDS, and others (4%). A chest tube is placed at the end of the operation routinely by 48 (30%), never by 59 (37%), and dependent on the repair by 54 (34%) of the respondents.
Discussion
The optimal surgical approach for CDH repair is controversial. Although the benefits of thoracoscopy in small children have been well documented, technical difficulties and reports on increased recurrence rates and hemodynamic side effects of the capnothorax prevent some centers from performing CDH repairs thoracoscopically. In light of the conflicting recommendations, this survey aimed to identify the preferred surgical strategy of the IPEG members, a group that was established as a venue to showcase advanced endoscopic techniques and the application of new developments.
The vast majority of the participants from all continents worked in academic institutions and had performed three or more CDH repairs in the last 12 months. The advanced level of surgical care was also documented by the availability of ECMO to more than 60% of the participants.
The management of preoperative pulmonary hypertension remains challenging because treatment decisions continue to depend largely on evidence from adult studies and the clinical experience of pediatric experts. 12 However, the majority of respondents use the following drugs routinely or at least in selected patients: nitric oxide (92%), 5-phosphodiesterase inhibitors (76%), surfactant (69%), and prostaglandins (63%). This indicates that all these medications are considered to have a role in preoperative management of pulmonary hypertension.
One of the main controversies regarding the technique of CDH repair is whether thoracoscopy is safe and effective. In a recent pilot prospective randomized trial, thoracoscopic CDH repair was associated with prolonged and severe intraoperative hypercapnia and acidosis, compared with open repair. 11 The high levels of hypercapnia and acidosis were of such concern that the trial's Data Monitoring and Ethics Committee advised that thoracoscopic repair of CDH should no longer be performed with this type of conventional insufflation and ventilation at this institution. A neurodevelopmental follow-up of these infants is currently under way to determine the effects of the hypercapnia and acidosis in the long term. 11 However, the conclusion of this study was not uniformly accepted, as opponents questioned the study design including rather high insufflation pressures (7–9 mm Hg). Moreover, other authors reported on no significant intraoperative pCO2 changes and shortened postoperative ventilation in selected patients after CDH repair.9,13 In this survey the impact of the trial was specifically addressed. It is interesting that the vast majority of the participants (72%) stated that this report made them change their approach and management of CDH, which indicates that IPEG members keep up with the current literature in their field. Nevertheless, an even higher percentage of the participants (89%) continue to perform thoracoscopic CDH repair at least in selected patients. The changes included patient selection criteria and insufflation regimens, with only 4% of the participants stating that they stopped performing thoracoscopic CDH repair.
Recurrence is another source of contention with thoracoscopic CDH repair. Although some authors reported an increased recurrence rate of thoracoscopic repair,8,10 others have failed to detect this.7–9,14 The concern some have raised about the recurrences with thoracoscopy is the fact that most repairs completed thoracoscopically are the smaller defects, which rarely recur after open repair. However, based on the retrospective data available, with the selection bias and the numerous differences in techniques and management it appears difficult to come to a clear conclusion regarding this complication. The participants reported on recurrences, which happened both directly after the operation as well as during late follow-up. It appears that the obvious benefits of thoracoscopic CDH repair have to be weighed up against technical limitations as about 50% of the endoscopic surgeons contend that CDH cannot be repaired equally by thoracoscopic and open repair. But, despite the awareness of potential pitfalls and the willingness to reconsider the most appropriate surgical approach, it appears that the individual experience of the participants drives them to perform thoracoscopic CDH repair at least after careful patient selection. The majority of surgeons refrain from thoracoscopy in patients on ECMO, and the history of ECMO is the second most common contraindication for a thoracoscopic repair. But, as well, large defects requiring patch repairs lead to conversion in all (31%) or at least in some cases (another 31% of participants). Thus the selection of the patients who benefit from thoracoscopy appears crucial.
Despite offering a general picture of the current practice of thoracoscopic CDH repair among IPEG members, we are aware of limitations of our study. There could have been a bias in selecting the surgeons as not all members responded. In addition, we can only assume that the participants provided honest answers. Finally, certain information such as recurrence rates could have a potential bias in patient selection.
Conclusions
Thoracoscopic CDH repair is currently being performed by 89% of all participating IPEG members. The need for ECMO and persistent right-to-left shunting are the main deterrents to thoracoscopic repair. Fifty-seven percent of participants had experienced recurrences after thoracoscopic repair. The fact that only 50% of surgeons stated that CDH can be repaired equally by thoracoscopy and open surgery suggests that future studies should focus on identifying the appropriate patient population.
Footnotes
Disclosure Statement
No competing financial interests exist.