
Abstract
Abstract
The importance of port closure after laparoscopic surgeries is emphasized by the extensive number of techniques being described for the same. Even so, the search for a simple, time-saving, and effective technique still continues. One commonly overlooked factor is the obliquity of laparoscopic ports, which makes direct visualization of the rectus fascia through the skin incision difficult. Also, our patients, mostly of Indian ethnicity, tend to have relatively thick subcutaneous fat that again acts as a constraint during port closure. We have described a simple and effective method of laparoscopic port closure using Moynihan's aneurysm needle and a skin hook. This technique is particularly advantageous in the above-mentioned scenarios. We have been successfully using this technique in our institution for the past 6 years, and we have not encountered any case of port-site hernia. Our technique does not require expensive instruments or the need for visualization via a camera.
Introduction
T
Umbilical ports used universally in laparoscopic surgeries are most vulnerable for port-site hernias (PSHs) owing to the thinness of the umbilical skin and low vascularity of the linea alba. Umbilical hernias make up 25% of the port-site hernias. 1 Hence it is vital to obtain a proper closure of umbilical ports. An overlooked fact is that laparoscopic ports, especially periumbilical ones, tend to have an oblique course of entry into the peritoneum compared with the perfect vertical entry described in most of the illustrations. This acts as a constraint, while port closure as most of the techniques described does not tend to take this obliquity to account.
The skin incisions necessary for placement of trocars should be as small as possible to prevent gas leakage. In most cases, it is difficult to visualize the fascia through these small incisions. Standard suture technique can be difficult and often involves blind closure of the defect.2,3 Also, manipulation of the trocars during extensive procedures tends to enlarge the opening in the abdominal wall and fascia, mandating a perfect port closure. 2
We describe a technique of laparoscopic port closure using a Moynihan's aneurysm needle and a skin hook. We have been successfully using this technique in our institution for the past 6 years, during which we have not encountered any case of PSH. Our technique does not require expensive instruments or the need for visualization via a camera.
Review of the Literature
We did a comprehensive review of the extracorporeal techniques described for port closure.
Shah et al. 4 have described a technique using a skin hook and direct suturing of the rectus using a heavy-caliber needle. Our study population comprised mainly middle-aged women of Indian ethnicity with above average subcutaneous fat density. Direct suturing using a needle holding forceps was cumbersome as the distance between the skin and rectus fascia was increased in most of our patients. Thus, we have made use of an aneurysm needle in addition with the skin hook.
Botea et al. 5 have described a similar technique using tissue-holding forceps to hold the fascia and direct closure using a needle holder. This technique too falls short when it comes to a thick abdominal wall, where direct visualization to pick up the sheath with a tissue holder is quite difficult.
Materials and Methods
Our procedure makes use of a Moynihan's aneurysm needle, a skin hook, 2-0 polyglactin 910 (Vicryl®; Ethicon, Somerville, NJ) suture material, and artery forceps.
Technique
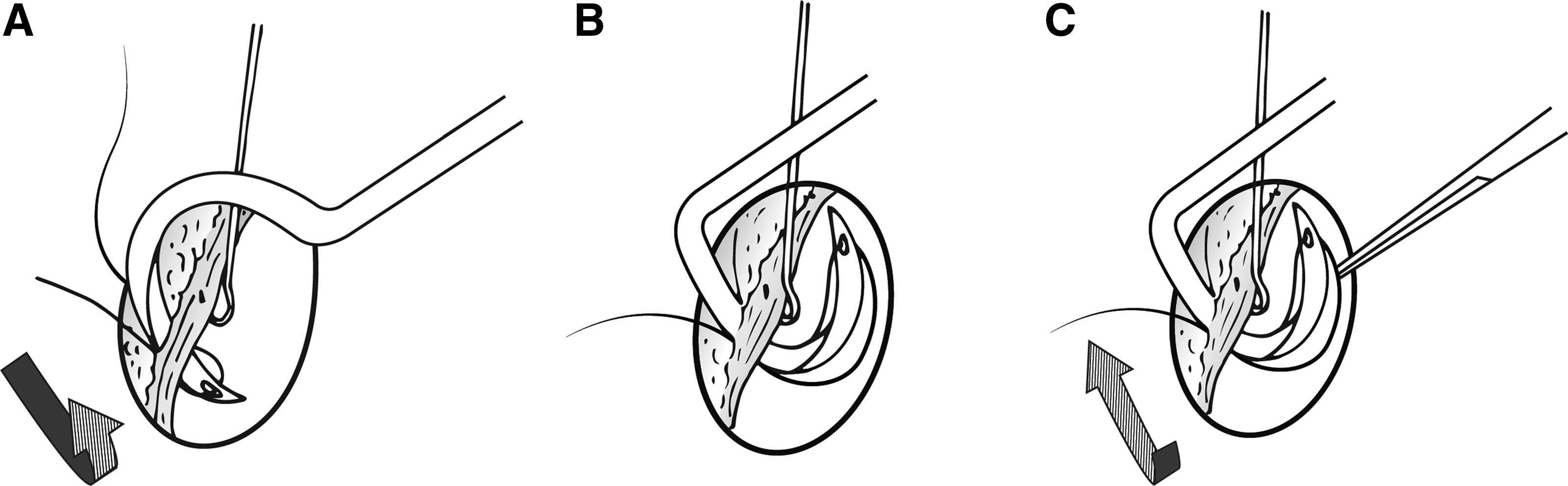
The technique is illustrated in Figures 1 and 2.
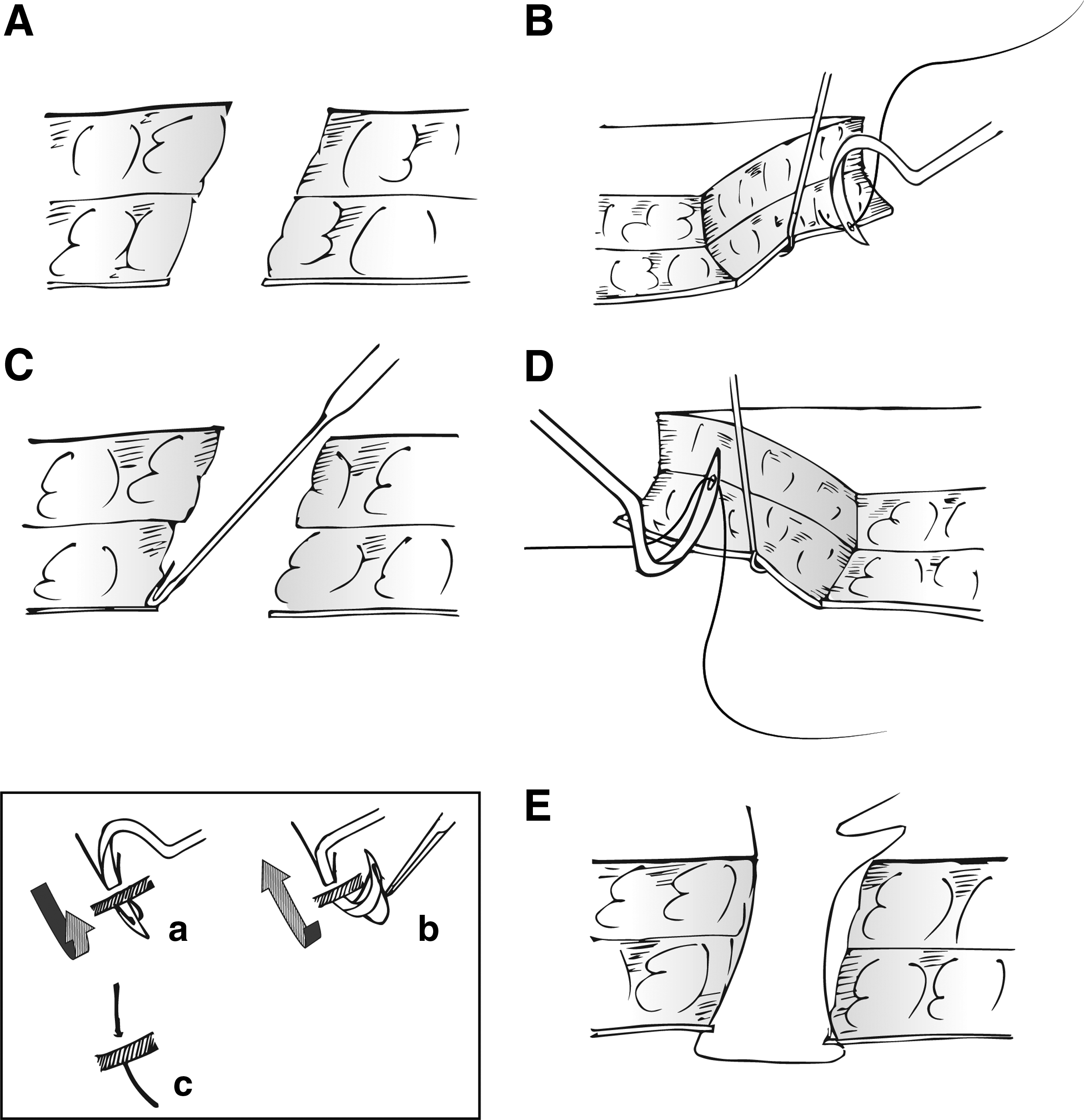
1. The obliquity of the port and the distance of fascia from the skin are judged primarily using palpation by the tip of the little finger.
2. A skin hook, rotated to 90° from its functional position, is then passed through the port and rotated back to hook the rectus sheath.
3. A loaded Moynihan's aneurysm needle is then passed though the taut sheath as shown. Further rotation in the same axis exposes the tip of the needle to the front.
4. The needle is dethreaded using a straight artery forceps, and the needle is retracted along the same axis.
5. The end of the thread is passed into the needle again, and the procedure is repeated in the opposite side.
6. The rectus sheath is held up and closed in the usual manner.
Discussion
Proper port closure after laparoscopic surgeries is vital for the prevention of PSHs. Although ports as small as 3 mm are associated with PSHs, ports of 10 mm and more in size are more commonly involved. More than 29 methods have been described for port closure. 1
Port closure techniques range from using specialized devices designed for the same to a standard skin closing technique. Shaher 3 has reviewed 15 techniques in addition to classical hand-sutured closure and classified them into three groups: (a) techniques that use assistance from the abdomen, (b) techniques that use extracorporeal assistance, and (c) closure techniques that can be performed with or without visualization.
Our technique ensures complete fascial closure while having the least chance of causing injury to intraperitoneal structures. The skin hook, which is inserted blindly to hold the rectus, is initially rotated 90° from its functional position so as to not injure the underlying structures. Lifting the sheath to make it taut prevents a blind insertion of the needle. The aneurysm needle by design avoids the hassles of suturing with a needle holder like needle rotation and slippage. The thick caliber of the aneurysm needle easily allows entry into the sheath, and the tip can be easily rotated to the front compared with locating the tip of a standard needle through the port tunnel.
An aneurysm needle is an inexpensive instrument used regularly in general surgery. We have described a new application for the same in laparoscopic port closure. This technique is being routinely used in our institute, and we find it very convenient compared with using a needle holder. This advantage is definitely evident in the case of umbilical ports where the port is obliquely placed and in well-built individuals with thick subcutaneous fat.
Footnotes
Disclosure Statement
No competing financial interests exist.