
Abstract
Abstract
Background:
Several techniques have been described for the surgical correction of rectal prolapse without any clear advantage for one technique over the other. We evaluated the use of laparoscopic suture rectopexy (LSRP) as a modality of treatment for rectal prolapse in children.
Materials and Methods:
Prospective data were collected for all children who presented to our center between 2011 and 2014 and required surgery for rectal prolapse. All children underwent LSRP with fixation of the mobilized rectum to the sacral promontory with multiple nonabsorbable sutures. The median follow-up period was 14 months (range, 6–29 months). The operative time, operative complications, length of hospital stay, and postoperative complications were recorded and analyzed.
Results:
Seventy-four patients presented with rectal prolapse during this period. Twenty patients (27%) required LSRP. Their median age at surgery was 4.4 years (range, 2–11 years), median operative time was 77.5 minutes (range, 30–150 minutes), and the median length of hospital stay was 1 day (range, 1–4 days). Only 1 patient had full-thickness recurrence that required redo surgery, and another had mucosal prolapse, which spontaneously resolved.
Conclusions:
LSRP is a safe and effective technique for treating children with full-thickness rectal prolapse with the benefits of being minimally invasive, a short hospital stay, early recovery, and low recurrence rate.
Introduction
A

Mucosal (partial-thickness) rectal prolapse.

Full-thickness rectal prolapse.
The period of conservative management for rectal prolapse needs to be varied according to the severity of the case. 4 The aim of surgical intervention is to create fibrosis between the layers of the rectum in case of mucosal prolapse or between the rectum and its neighboring posterior fascia for full-thickness prolapse. 5
There is no optimum surgical technique for treating persistent rectal prolapse. Various procedures have been described with variable levels of success, ranging from less invasive injection sclerotherapy and the Thiersch procedure to more invasive procedures for rectopexy, by the perineal, abdominal, or laparoscopic approach. 6 In this study we analyzed the use of laparoscopic suture rectopexy (LSRP), which is the primary surgical approach performed for cases of full-thickness rectal prolapse in our center.
Materials and Methods
Prospectively, over a 3-year period from 2011 to 2014, all patients who presented with rectal prolapse were included in this study.
Investigations were performed to exclude underlying causes such as constipation, parasitic infestations, malnutrition, and gastroenteritis. Stool examination was done for all children to look for parasitic infestations. Plain abdominal x-rays were performed to judge fecal loading in cases with constipation and to detect any vertebral anomalies. In addition, barium enemas were performed on all patients, looking for megasigmoid or filling defects suggestive of polyps.
As none of the patients had neurological impairment, magnetic resonance imaging of the spine was not performed for any patient.
Cystic fibrosis testing was deemed unnecessary due to the extremely low incidence in our population.
Initial management included treatment of any underlying causes. Constipation was managed with dietary modification and laxatives, malnourished children were referred to dietician specialists, and anthelminthic drugs were administered to those with parasites on stool examination.
All children with persistent rectal prolapse after successful treatment of secondary causes, as well as those who had recurrence after previous surgery, underwent LSRP.
Patients were only allowed clear fluids for 24 hours before surgery and had rectal washout the night before surgery.
Operative details
The procedure was performed with the patient under general anesthesia. With the patient supine, four ports were used for mobilization and suturing of the rectum to the sacral promontory: an umbilical port for the scope, two lateral working ports in the midclavicular line at the level of the umbilicus, and the fourth port was inserted at a higher level in the left anterior axillary line for retraction of the rectum throughout the procedure. The table was tilted head down and right side up to evacuate the pelvis and allow better exposure of the rectum.
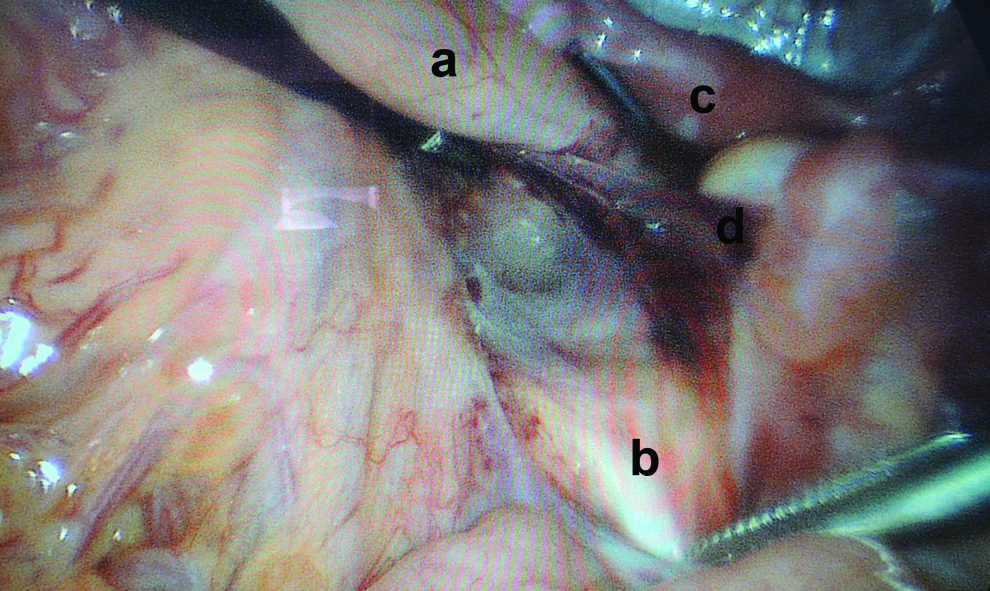
The peritoneum was incised on the right side of the rectum starting from the peritoneal reflection to the sacral promontory (Fig. 3). The right ureter was identified prior to the peritoneal incision to avoid its injury. The retrorectal space was dissected to the level of the pelvic floor (Fig. 4). This space is avascular, and minimal manipulation is needed to create the space. Polypropylene sutures were used to fix the seromuscular wall of the rectum to the periosteum of the sacral promontory, avoiding the nervi irrigens (Figs. 5 and 6). Sutures were placed low enough to keep the rectum in position without being under excessive tension. The peritoneum was then closed with absorbable sutures. We routinely added stool softeners for 1 month following surgery to avoid excessive straining.
Peritoneum incised on the right side of the rectum from the level of peritoneal reflection to the sacral promontory:
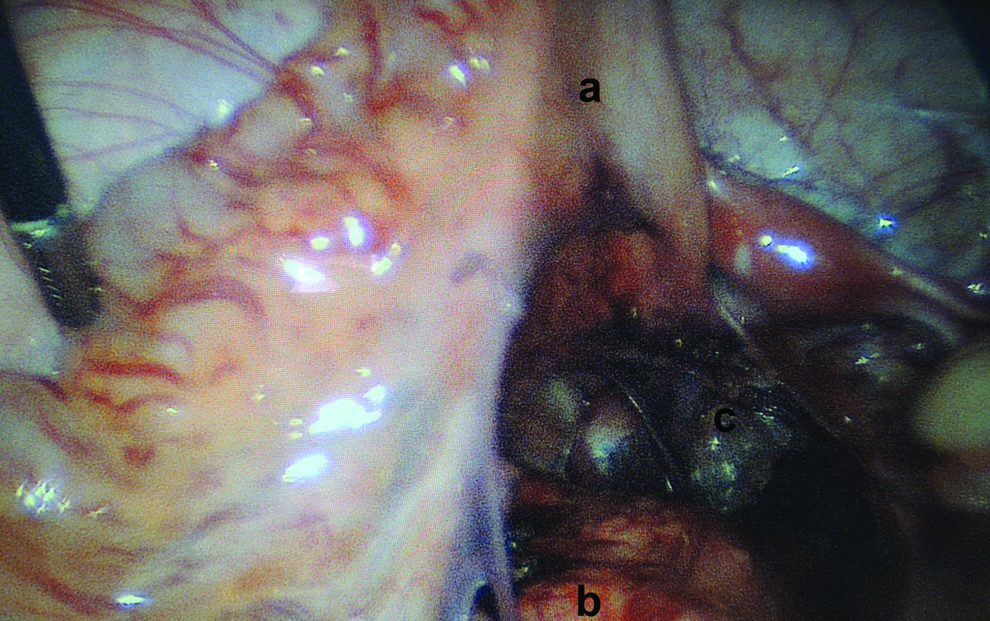
Retrorectal space dissected to the level of the pelvic floor:

Seromuscular wall of the rectum sutured to the periosteum of the sacral promontory:

The back of the rectum sutured to the periosteum of the sacral promontory:
The operative time, mean hospital stay, operative and postoperative complications, and any recurrence were recorded. After discharge all patients were followed up in an outpatient clinic at 3, 6, and 12 months after the procedure and then at yearly intervals.
Results
Seventy-four children with either complete or partial-thickness rectal prolapse presented to our center during the study period. Nine of them had had a previous injection sclerotherapy with or without the Thiersch procedure, at a different center, that had failed. All 9 of these patients had LSRP.
Of the remaining 65 patients, 18 failed to respond to conservative management. Seven of these patients had mucosal prolapse that was successfully treated by injection sclerotherapy. The remaining 11 children underwent LSRP, so a total of 20 children (27%) had LSRP.
Median age at time of surgery was 4.4 years (range, 2–11 years). Male predominance (7:3) was noted.
The frequency of occurrence of rectal prolapse was variable. However, most of the patients reported the prolapse happened only with passing stools. One patient had a prolapse occurring spontaneously without straining. Presenting symptoms are shown in Table 1.
The stool microscopy was positive for parasites (Giardia lamblia, Entrobius vermicularis, Entamoeba histolytica) in 4 cases (20%), necessitating treatment with antihelminthics. Three children had constipation, and two were malnourished. Twelve (60%) children were reported to be using rural toilets, which involves acquiring a squatting position, predisposing them to rectal prolapse.
Barium enema was performed on all patients and showed no abnormality.
Median operative time was 77.5 minutes (range, 30–150 minutes). No intraoperative complications were encountered. One procedure was converted to open due to equipment failure. One case was augmented by a Thiersch procedure due to an extremely patulous anus secondary to persistent prolapse.
Feeding was initiated in the immediate postoperative period. Most children tolerated feeds well except for 2 patients who had postoperative ileus; 1 of them was found to have a port-site hernia, which was repaired. Median length of hospital stay was 1 day (range, 1–4 days).
One patient had a full-thickness recurrence and required a redo surgery 3 months after the initial surgery. Another patient had a partial mucosal prolapse that resolved spontaneously.
Discussion
The most common predisposing factors for rectal prolapse in developed countries are constipation and cystic fibrosis, whereas in developing countries, malnutrition, diarrheal illnesses, parasitic infestations, and faulty toilet training (whether too early or due to the use of rural toilets) are the main causes. 1
The finding of a megasigmoid on barium enema would influence the type of procedure performed, as one would consider the need for sigmoid resection in addition to the rectopexy. However, none of our patients had any abnormalities detected on barium enema. Therefore we no longer routinely perform barium enema, limiting its use only in children with intractable constipation, thereby preventing unnecessary radiation exposure.
We performed LSRP with two or three nonabsorbable sutures to fix the rectum to the sacral promontory. The number of sutures used did not influence the outcome as the sutures were meant to keep the rectum in place until sufficient fibrosis has occurred. However, the use of two sutures shortened our operative time without changing the outcome. Our operative times were comparable to those in similar studies.4,7
We divided the peritoneum on the right side of the rectum and performed retrorectal dissection. We found it unnecessary to do complete mobilization of the rectum as good results were obtained with minimal rectal mobilization. Puri 8 reported good results with a similar surgical technique avoiding complete rectal mobilization.
Our overall recurrence is 1 in 20 patients (5%) and 1 case of partial (mucosal) rectal prolapse (5%), which was comparable with contemporary studies. Ismail et al. 7 reported no recurrences in their series. Potter et al. 4 reported one full-thickness recurrence (5%) and two partial-thickness recurrences (11%).
Randall et al. 9 reported a 0% success rate with LSRP. It remains unclear if this was due to performing the procedure on a different cohort of patients who were older (median age at operation was 14 years), different predisposing factors (mainly constipation and solitary rectal ulcer), or having had a longer median follow-up revealing more recurrences.
Other less invasive procedures, such as injection sclerotherapy with or without the Thiersch anal encirclement procedure, have been used for treatment of rectal prolapse, with a reported success rate of approximately 90% after three injections in some series.6,10 Although these procedures are simple and less invasive, they are not without complications such as anal pain, stricture, ischiorectal abscess, and fistula. 1 They also have a higher recurrence rate requiring the procedures to be repeated, subjecting the child to multiple general anesthetics. In addition, they are not suitable for patients with full-thickness rectal prolapse.
We believe that intervention for rectal prolapse should be tailored according to the type of prolapse, as well as the experience of the surgeon. LSRP is a safe and effective technique for managing full-thickness rectal prolapse in children. It is currently performed as a day case procedure in our center.
This study has limitations of being a single-center observational study, with a relatively short follow-up. However, the promising results of this technique when compared with contemporary techniques have to be acknowledged.
Conclusions
LSRP is an effective technique for treating children with full-thickness rectal prolapse. It has the benefit of a low recurrence rate and with surgeon expertise could be performed as a day case procedure.
Footnotes
Acknowledgments
We thank Mr. A. Niyogi, Miss L. Gavens, and Mrs. M. Alhusseiny for their helpful comments on the manuscript.
Disclosure Statement
No competing financial interests exist.