
Abstract
Abstract
Introduction:
The purpose of this report is to describe a tension-free repair we have used successfully in 12 patients with large hiatal defects. It is based on the creation of a web-shoelace pattern of polypropylene (Prolene®; Ethicon, Somerville, NJ) suture of the crura that functions as a barrier, with the advantages of being stronger and more economical than a mesh without the potential complications that may follow mesh repair or suture repair of a large hiatus hernia without mesh. Despite a success rate of 85%–95% reported in large series with a mid- and long-term follow-up evaluation, significant complications have been associated with hiatus hernia repair. Some of these complications include a slipped Nissen repair with intrathoracic wrap migration and hiatal hernia recurrence, resulting from inadequate closure of the crura, fundoplication disruption, or dehiscence of the hiatoplasty.
Materials and Methods:
From June 2013 to June 2014, we have used this technique on 12 patients (6 women and 6 men). Only patients with a large hiatus hernia of >4 cm were enrolled in this study. All patients underwent laparoscopic Nissen fundoplication and hiatoplasty using our technique. They were all severely symptomatic with dysphagia, retrosternal pain, gastroesophageal reflux disease, and respiratory symptoms at night.
Results:
Of the 12 patients who underwent this type of repair, all of them have reported good to excellent functional and symptomatic outcomes with minimal morbidity, no deaths, and no recurrence.
Conclusions:
It is our belief that when a correct repair of the hiatus is not achieved with three stitches, adding more sutures will not lead to a tension-free repair, and this hiatoplasty will have an increased risk of dehiscence. It is for this reason that we recommend using our technique instead of using simple nonabsorbable sutures or a prosthetic mesh.
Introduction
A
The purpose of this report is to describe a tension-free repair we have used successfully in 12 patients with large hiatal defects. It is based on the creation of a web-shoelace pattern of polypropylene (Prolene®; Ethicon, Somerville, NJ) suture of the crura that functions as a barrier, with the advantages of being stronger and more economical than a mesh without the potential complications that may follow mesh repair or suture repair of a large hiatus hernia without mesh.
Laparoscopic antireflux surgery is considered the gold standard in the treatment of gastroesophageal reflux disease with or without hiatal hernia. 1 Since the original operation described by Rudolf Nissen in 1956, 3 the Nissen fundoplication technique has had very few modifications. Closure of the crural defect has been an integral component of this procedure since its inception.
Since the first description by Dallemagne et al. 1 in 1991, the minimally invasive approach has gained worldwide popularity among surgeons.1–3 However, despite a success rate of 85%–95% reported in large series with a mid- and long-term follow-up evaluation, significant complications have been associated with hiatus hernia repair. 4 Some of these complications include a slipped Nissen repair with intrathoracic wrap migration and hiatal hernia recurrence, resulting from inadequate closure of the crura, fundoplication disruption, or dehiscence of the hiatoplasty.4–6 The initial satisfactory outcomes have been counterbalanced by a high recurrence rate complicating laparoscopic suture–only hiatus hernia repair in cases of giant hiatus hernias, reaching an incidence of up to 43% of the cases with hiatal defects over 4 cm.7,8 The application of mesh-reinforced hiatal closure has resulted in a significant reduction in recurrence rates.
Nevertheless, one of the most debated issues has been the risk of complications related to the use of the prosthetic mesh, such as erosion or migration of the mesh into the esophagus or stomach, as well as the development of fibrotic strictures, causing a high rate of dysphagia symptoms, which are the main drawbacks discouraging wide application of mesh hiatoplasty.9,10 Mesh-related complications have been reported with both permanent and biologic mesh placed at the hiatus,10,11 with an incidence rate varying from 0.1% to 20% in the world literature.11–15 The failure rate of all antireflux procedures, both open and laparoscopic, is reported to be 10%, ranging from 3% to 30%.16–18
Anatomical causes of failure and recurrence of a hiatus hernia
Both anatomic and ultrastructural characteristics of the hiatal crus as well as the mean diameter of the hiatal defect seem to play a key role in the development of these types of complications. 19 The crus, particularly the right crus, consists of soft parallel muscular fibers reinforced with few or no tendons, which easily tears if grasped or sutured.
Poor satellite cells and extracellular content may lead to a weakness in the formation of scar tissue. In addition, crural closure generates lateral tension proportional to the hiatal defect diameter, which may lead to disruption of hiatal repair during vigorous inspiratory movements of the diaphragm, such as forceful vomiting, coughing, or constipation.18,19
The cornerstone of our technical innovation has been the use of a handmade Prolene web using nylon 2-0 suture material, free of tension between the left and the right pillars, easy to perform, loose, flexible, and free of tension, with the advantage of being low cost and avoiding the development of adhesions and fibrosis from less fibrotic reaction, less inflammation, and less irritation to the exposed esophageal tissue.
Materials and Methods
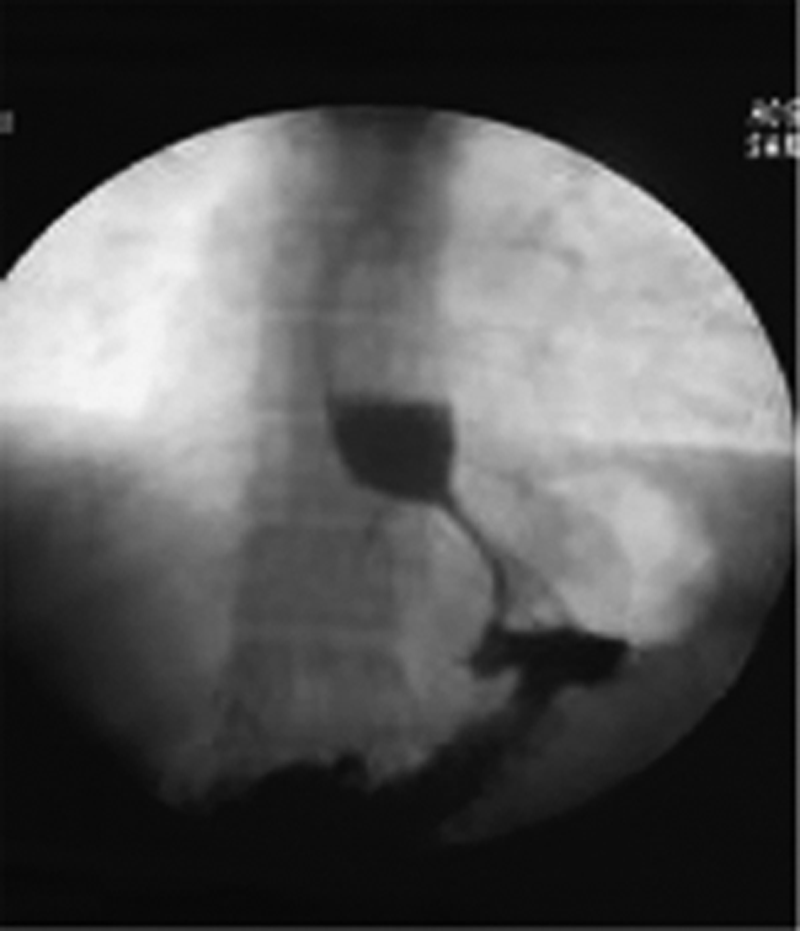
From June 2013 to June 2014, we have used this technique on 12 patients. All patients underwent laparoscopic Nissen fundoplication and hiatoplasty using our technique. There were six women and six men, with a mean age of 61.2 years (range, 19–84 years). Only patients with a large hiatus hernia of >4 cm were enrolled in this study. Patients with a hiatus hernia of <4 cm were not included. All the patients (100%) had a giant hiatus hernia with severe esophagitis demonstrated by endoscopy and esophagogram. They were all severely symptomatic with dysphagia, retrosternal pain, gastroesophageal reflux disease, and respiratory symptoms at night. One patient had a recurrent hernia with wrap migration into the chest, only 4 months after the original surgery (Figs. 1 and 2). The median hiatal defect was 4 cm (range, 4–5 cm). All the patients underwent a standard preoperative workup including physical examination, blood analysis, upper gastrointestinal barium meal X-ray study, and esophagogastroduodenoscopy with biopsy.
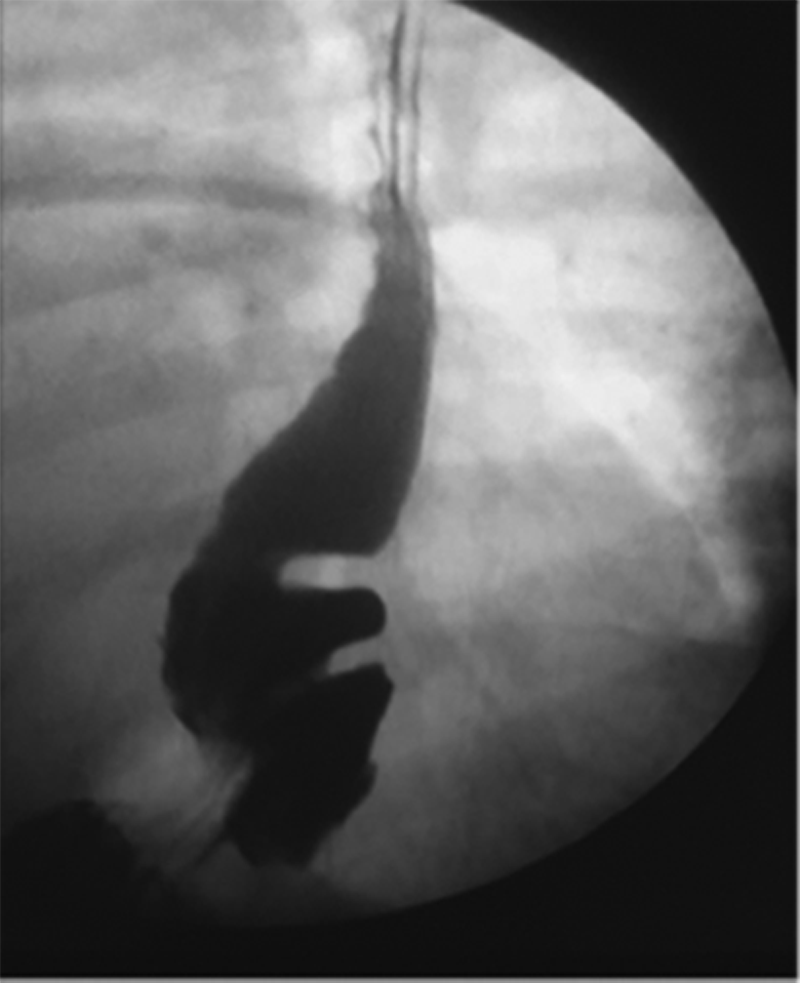
Wrap migration into the chest.

Recurrent hernia with wrap migration into the chest, 4 months after the original surgery.
Patients demonstrating severe esophagitis at endoscopy that proved responsive to proton pump inhibitors as well as those who presented with a large hiatus hernia demonstrated by gastrointestinal barium meal X-ray and with severe symptoms such as heartburn, regurgitation to the throat, vomiting, and respiratory symptoms were usually not required to undergo esophageal pH assessment. 19
Postoperative follow-up was performed at 2 weeks and 1, 3, 6, and 12 months so far. An upper gastrointestinal barium meal X-ray study was performed at 3 months. Hiatal hernia or gastroesophageal reflux disease symptom recurrences including dysphagia and pain complications were investigated.
Operative technique
The technique was standardized for all patients and included a laparoscopic five-port approach. Exclusive use is made of the laparosonic coagulating shears (Ultracision®; Ethicon Endo-Surgery, Cincinnati, OH) throughout the procedure for surgical cutting, coagulation, and tissue dissection. The first step is dissection of the phrenogastric attachment. The short gastric vessels are routinely divided to facilitate a 2.0–2.5-cm “floppy wrap” according to the principles described by DeMeester et al. 16 The mobility of the fundus is then enhanced by excision of the fat pad found at the angle of His. The anatomical “bare area” of the stomach posteriorly is then extensively mobilized.
The gastrohepatic omentum is divided, with attention paid to preserving the hepatic branch of the vagus nerve. In brief, the laparosonic coagulating shears are used to dissect the hiatal slings of both the left pillar first and then the right pillar to create a posterior esophageal window. A Penrose drain is then passed around the distal esophagus, and the esophagus is then dissected circumferentially. The mediastinum is then entered posterior to the esophagus, and the anterior and posterior vagus nerves are identified and left attached to the esophagus. The esophagus is then very gently mobilized extensively in the chest to enable up to 3 cm of tension-free intraabdominal esophagus. The key point in the surgical repair in the hiatoplasty is to use a nonabsorbable 2-0 Prolene suture. The first step in the procedure is to anchor the Prolene suture to the inferior “V” where the right crus and the left crus meet in the inferior middle line (Fig. 3).

The first step in the procedure is to anchor the Prolene suture to the inferior “V” where the right crus and the left crus meet in the inferior middle line.
An end thread of 3 cm is left on purpose, so we can use it to tie the end stitch to it (Fig. 4).

An end thread of 3 cm is left on purpose, so we can use it to tie at the end stitch to it.
We tailor a continuous suture where each stitch is placed in the lateral aspect of the left crus (Figs. 5 and 6) and crossing upward to the medial aspect of the left crus and from the medial aspect of the right crus to the lateral aspect of the right crus, forming a web-shoelace pattern (Figs. 6–8), making sure that when pulling the stitch we leave it loose and free of tension (Fig. 8).

We tailor a continuous suture where each stitch is placed in the lateral aspect of the left crus and crossing upward to the medial aspect of the left crus.

Continuous suture where each stitch is placed from the lateral aspect of the right crus and crossing upward to the medial aspect of the right crus and from the medial aspect of the left crus to the lateral aspect of the left crus, forming a web-shoelace pattern.

When pulling the stitch we make sure to leave it loose and free of tension.

Prolene in a web-shoelace pattern. It is important not to pull the thread strongly as it would defeat the purpose of the web.
It is important not to pull the thread strongly, as this would defeat the purpose of the web. When we get close to the posterior wall of the esophagus, we leave a small space between the posterior esophagus and the upper edge of the web. We turn the suturing downward the same way until we reach the end thread, where we tie the last knot (Fig. 9).

When we get close to the posterior wall of the esophagus, we leave a small space between the posterior esophagus and the upper edge of the web. When turning the suturing downward, do it in the same way until reaching the end thread, where the last knot is tied.
The end result is a Prolene web-shoelace pattern that is easy to implement, that is loose, flexible, and free of tension, and that gives free mobility to the crus during inspiratory movements of the diaphragm or forceful movements such as vomiting, retching, or straining, as well as free movements of the esophagus during swallowing.
This Prolene web-shoelace pattern is low-cost, avoids the development of adhesions, and produces less fibrotic reaction and less irritation to the exposed esophageal tissue.
After complete mobilization, a portion of the fundus is pulled by a Babcock clamp behind the esophagus and then released, testing the tension of the wrap. The 360° wrap is secured loosely around the esophagus using three stiches of 2-0 nonabsorbable Prolene sutures between the anterior stomach and the posterior fundic wrap, with one incorporating the anterior esophageal wall to maintain the intraabdominal esophageal segment and discourage wrap slippage.
The repair is calibrated in males with a 38 French bougie and in small females with a 36 French bougie. The pneumoperitoneum was allowed to escape, and all wounds are closed with subcuticular absorbable sutures.
Results
Of the 12 patients who underwent this type of repair, all of them have reported good to excellent functional and symptomatic outcomes with minimal morbidity and no deaths. We have followed up the patients at 2 weeks, 1 month, 3 months, and 6 months after surgery. After that, we have had contact with all of them by telephone. All of them have reported no dysphagia or heartburn in the early or late postoperative period. Endoscopy was performed in 6 patients, 6 months after surgery, all of whom are maintaining the intraabdominal esophageal repair in place. Upper gastrointestinal X-ray study and endoscopy confirmed this (Figs. 10 and 11). There has been no recurrence.
Postoperative upper gastrointestinal X-ray study and endoscopy. The intraabdominal esophageal repair is maintained in place.

Postoperative endoscopy where the Nissen fundoplication repair is maintained in place.
Discussion
Why avoid the use of mesh?
Recent techniques of surgical repair have described the use of mesh in an attempt to decrease recurrence rates. Stadlhuber et al. 9 found 17 of 28 mesh repairs required secondary operations. All had developed mesh erosion, 6 cases developed stenosis, and 5 cases developed fibrosis. Esophagectomy was required in 6 cases and gastrectomy in 3 cases. There was no apparent relationship between the types of mesh used primarily (including biological). 9 Tatum et al. 11 reported 2 cases of mesh esophageal perforation requiring total gastrectomy.
No ideal surgical technique for large hiatus hernias has been reported. Preferably, the ideal operation should have low morbidity and low recurrence rates, no mortality, and no requirement for the use of mesh, with elimination of the risk of strangulation and dysphagia and, most importantly, a sustained improvement in quality of life of the patient.
It is our belief that when a correct repair of the hiatus is not achieved with three stitches, adding more sutures will not lead to a tension-free repair, and this hiatoplasty will have an increased risk of dehiscence. In giant hiatal hernias over 4 cm in diameter, three sutures are usually not enough to close the crural defect; therefore adding more sutures will result in a tense repair with high probability of failure. It is for this reason that we recommend using our technique instead of using simple nonabsorbable sutures or a prosthetic mesh.
Why Prolene sutures?
Prolene has a minimal tissue reaction and has an excellent flexibility; the surface is extraordinary soft, which avoids the development of tension, adhesions, and fibrosis reaction with less irritation to the exposed esophageal tissue. The soft web will be covered by granulation tissue in 2 days, which will give permanent support. Other advantages include that it is easy to perform and much more economical when compared with a mesh.20–22
Prolene has proven to cause much less reactive effect in instances of all types of hernia repairs, causing minimal postoperative pain and having less analgesic requirements, and is even used in ophthalmological surgery as polyglactin sutures, which resulted in slightly more conjunctival reaction in the early postoperative period compared with nylon sutures.20–22
Conclusions
An innovative web-shoelace–like pattern suture technique for closure of giant hiatus hernias is presented. No complications or recurrences have occurred. We recommend that, when faced by a large hiatal defect, the use of this alternative technique is superior to the use of mesh, to repair the hiatus with three stitches or not closing the defect at all.
Footnotes
Disclosure Statement
No competing financial interests exist.