
Abstract
Abstract
Background:
Technologic advances and superior survival with mechanical circulatory support (MCS) have led to an expanding population that develops intraabdominal conditions requiring intervention. Whether laparoscopy can be performed without detrimental effects on hemodynamics and device function is not well described.
Materials and Methods:
Effects of laparoscopy performed on MCS were retrospectively assessed. Intraoperative hemodynamics and device function were compared with the same time interval 24 hours prior to surgery using intrapatient paired t tests. Outcomes included survival, transfusion, thromboembolic events, and infection.
Results:
Twelve patients with ventricular assist devices or total artificial hearts underwent laparoscopy from 2012 to 2014. Median follow-up was 116 days. Operations included cholecystectomy, diagnostic laparoscopy, gastrojejunostomy, and gastrostomy. There were no differences between preoperative and intraoperative mean arterial pressure, heart rate, and inotrope or vasopressor requirements (P > .05). Device fill volume, flow, rate, and power were unchanged (P > .05), whereas pulsatility index decreased by 0.2 (95% confidence interval, 0.03, 0.36) with laparoscopy (P = .03). All intraoperative fluctuations in hemodynamics and device function improved with reduction of pneumoperitoneum, adjusting device speed, or pharmacologic support. There were no operative mortalities. Thirty-day survival and survival to discharge were 75% and 50%, respectively. Despite antiplatelet therapy and preoperative international normalization ratio of 2.2 ± 0.9, there were no re-operations for bleeding, and 50% did not require transfusion. Two patients with recent cardiac surgery had thromboembolic events: one stroke and one device thrombus. None had postoperative bacteremia or driveline infection.
Conclusions:
Laparoscopy can be performed on MCS with low morbidity and mortality and minimal perturbations in hemodynamics and device function.
Introduction
O
In the United States alone, over 2500 durable MCS devices, which include left ventricular assist devices (LVADs), right ventricular assist devices, or biventricular assist devices and total artificial hearts, are implanted annually. 4 The increasing rate of device implantations reflects improved understanding of the benefit devices offer patients with advanced heart failure that began with the REMATCH study. 5 One- and 2-year survival rates with continuous flow LVADs are now 80% and 70%, and over 40% of devices are placed as destination therapy 4 for patients who are ineligible for heart transplantation, often because of advanced age or comorbidities.
As the rate of device implantation and the duration of support increase, there is an expanding population of MCS patients at risk for developing intraabdominal conditions that warrant evaluation by a general surgeon. Hemorrhage, thromboembolism, infection, and malperfusion can lead to intraabdominal pathology that may require operative intervention. Abdominal operations performed most frequently in MCS patients include cholecystectomy, appendectomy, exploratory laparotomy, hernia repairs, intestinal resections, and weight loss operations.6,7 Outcomes for LVAD patients undergoing noncardiac surgery have been favorable with equivalent 1-year survival when compared with LVAD patients not requiring noncardiac surgery and conflicting findings on survival to heart transplantation.8,9
Laparoscopy is an effective approach to the diagnosis and treatment of intraabdominal pathology. As improvements in laparoscopic equipment and technical skills have facilitated safe applications of laparoscopic surgery to treat increasingly broad conditions and patient populations, many historical contraindications to laparoscopy are no longer considered absolute. Current dogma identifies four absolute contraindications to laparoscopy—inability to tolerate laparotomy, hypovolemic shock, lack of proper surgeon training and/or experience, and lack of appropriate institutional support—as well as five relative contraindications—inability to tolerate general anesthesia, long-standing peritonitis, large abdominal or pelvic mass, massive incarcerated ventral and inguinal hernias, and severe cardiopulmonary disease. 10
Carbon dioxide pneumoperitoneum can have pronounced effects on the cardiovascular, pulmonary, and renal systems (Fig. 1). The physiologic consequences of laparoscopy, including changes in systemic vascular resistance, increased preload and afterload, reduced cardiac output, cardiac arrhythmias, hypercarbia, cephalad displacement of the diaphragm, reduced renal blood flow, release of antidiuretic hormone, and oliguria becoming an unreliable indicator of hypovolemia, were established in healthy patients not on MCS.10,11 Whether pneumoperitoneum has similar effects on the physiology of patients on MCS remains uninvestigated.
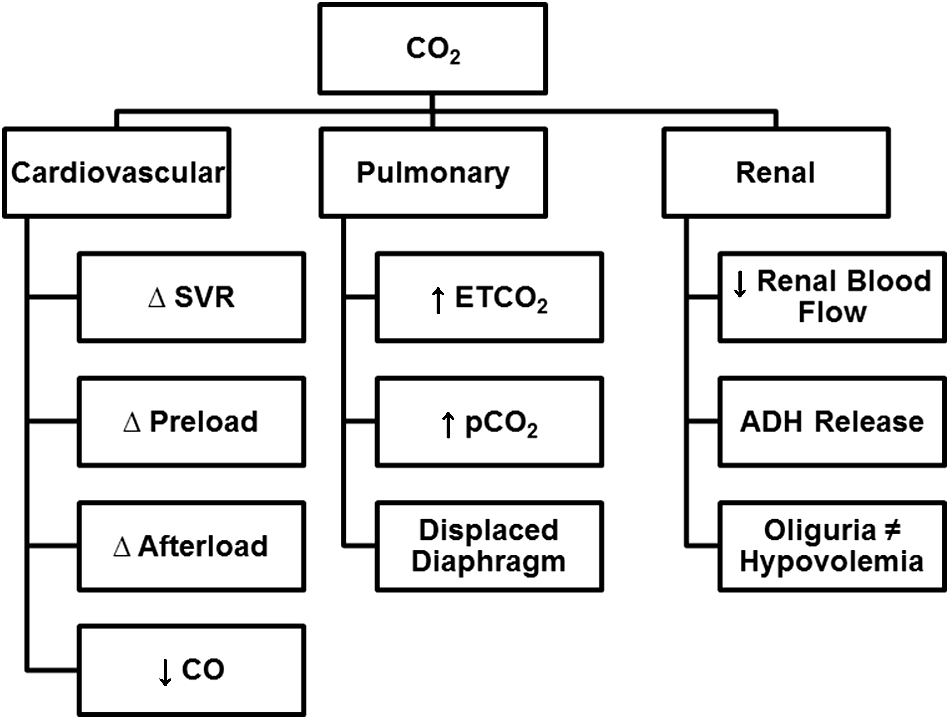
Physiologic consequences of carbon dioxide pneumoperitoneum. The physiologic changes during laparoscopic surgery are multifactorial but are largely attributed to the combined influences of peritoneal absorption of carbon dioxide, elevated intraabdominal pressures, and patient positioning. The effects on various organ systems were established in healthy patients not on mechanical circulatory support devices. Concerns that patients with advanced heart disease may be more susceptible to these changes and less able to mount appropriate compensatory responses remain are counterbalanced by a small, but growing, number of reports that laparoscopy can be safely performed in patients with mechanical circulatory support devices. ADH, antidiuretic hormone; ETCO2, end-tidal CO2; pCO2, partial pressure of CO2; SVR, systemic vascular resistance.
To explore our hypothesis that laparoscopy can be performed safely on MCS patients, we reviewed our experience with a focus on intraoperative hemodynamics, device parameters, and complications such as death, bleeding, thrombosis, or infection.
Materials and Methods
Study design
All patients with LVADs, biventricular assist devices, or total artificial hearts undergoing laparoscopic operations performed by one surgeon at Cedars-Sinai Medical Center (Los Angeles, CA) from August 2012 to April 2014 were included for retrospective analysis to characterize the effects of laparoscopy on MCS. MCS patients undergoing planned laparotomy were excluded. To account for interpatient variation in preoperative clinical status, each patient served as his or her own control: intraoperative hemodynamics and device function were compared with the same time interval 24 hours prior to surgery using intrapatient paired t tests. This study was reviewed by, approved by, and conducted in compliance with the Cedars-Sinai Institutional Review Board.
Operative approach and anesthetic technique
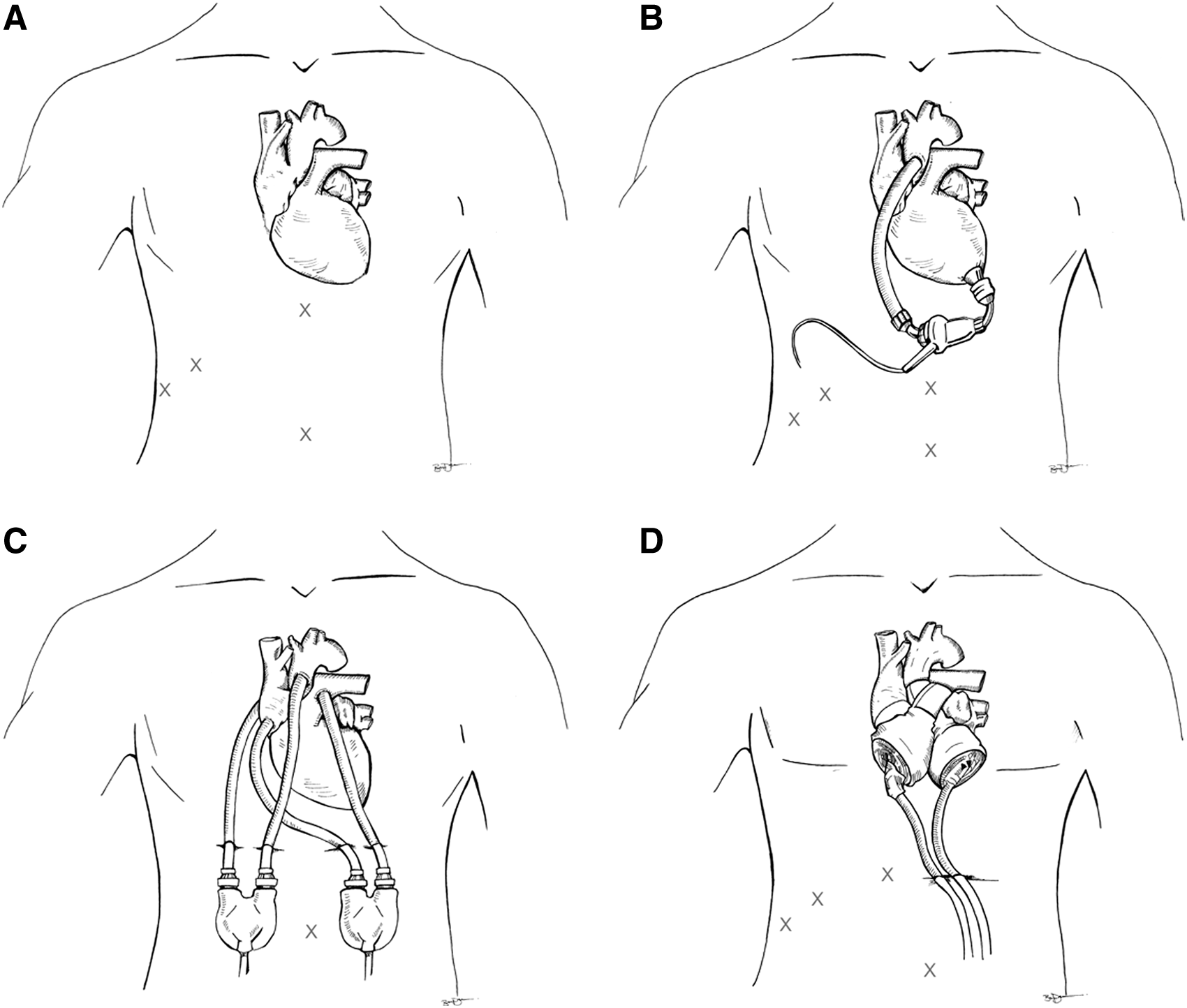
All operations were performed with cardiac anesthesia and perfusion teams. Anticoagulation and antiplatelet therapies were not routinely maintained; warfarin was reversed with fresh frozen plasma selectively. All patients underwent general anesthesia with endotracheal intubation and were positioned supine in a reverse Trendelenburg position. All patients underwent arterial line placement; central venous and pulmonary artery catheters were used selectively. Intravenous fluids were minimized, with 3 of the 12 patients receiving no crystalloid or colloid and 4 of the 12 receiving less than 500 mL (mean volume of fluids administered, 550 ± 541 mL). Drivelines were prepped and draped within the operative field. Preoperative antibiotics were administered prior to skin incision. Carbon dioxide pneumoperitoneum was delivered via a Veress needle to achieve pressures of 12–15 mm Hg. The positions of trocar sites were modified based on the location of drivelines (Fig. 2). Fasciae for all trocar sites ≥10 mm were closed, and skin was closed with absorbable monofilament suture.
Outcomes
Hemodynamic and device parameter data recorded by anesthesiologists, perfusion technologists, and cardiac surgery intensive care nurses were collected. Postoperative outcomes and major adverse events, including patient survival, re-operation for bleeding, need for transfusion, thromboembolic events, or infections, were also analyzed. Thromboembolic events included stroke, defined as the presence of any neurologic deficit and/or computed tomography findings consistent with intracranial hemorrhage or ischemic stroke, and device-associated thrombus identified by echocardiography. Infections were defined as clinically suspected or culture-proven infection requiring antibiotic treatment or opening of a wound and were categorized as bacteremia, urinary tract infection, pneumonia, abdominal surgical site infection, or driveline infection.
Statistical analysis
Continuous variables are expressed as the mean ± standard deviation or median (range) values, and categorical variables are presented as count (%). Differences between preoperative and intraoperative parameters were assessed by paired Student's t tests with significance defined as two-tailed P values < .05. The statistical analysis was performed using GraphPad Prism 5 for Windows (GraphPad Software, San Diego, CA).
Results
Twelve patients with ventricular assist devices or total artificial hearts underwent laparoscopy. Median follow-up was 116 (3–371) days. The types of device and operations performed are summarized in Table 1, and preoperative patient characteristics are given in Table 2. Median procedure time was 2 hours 23 minutes (53 minutes–4 hours 12 minutes). There was a single conversion to the open procedure.
BiVAD, biventricular assist device; LVAD, left ventricular assist device; TAH, total artificial heart.
BMI, body mass index; BTT, bridge to transplantation; F, female; ICM, ischemic cardiomyopathy; INR, international normalized ratio; INTERMACS, Interagency Registry for Mechanically Assisted Circulatory Support; M, male; MCS, mechanical circulatory support; NICM, nonischemic cardiomyopathy.
At baseline, average heart rate was 83.2 ± 18.04 beats/minute, mean arterial pressure was 77.02 ± 10.89 mm Hg, inotrope requirement was 2.5 ± 5.00 μg/minute, and vasopressor requirement was 0.01 ± 0.02 U/minute. There were no differences between preoperative and intraoperative heart rate, mean arterial pressure, or inotrope or vasopressor requirements (Table 3) (P values = .23–.45). Device fill volume, flow, rate, and power were unchanged (P values = .20–.93), whereas pulsatility index decreased by 0.2 (95% confidence interval, 0.03, 0.36) with laparoscopy (P = .03) (Table 3). All intraoperative fluctuations in hemodynamics and device function improved with reduction of pneumoperitoneum, adjusting device speed, or pharmacologic support. There were no device power interruptions due to electrocautery interference. Of 5 patients on inotropic or pressor support prior to surgery, 1 (20%) required a brief increase in support (epinephrine raised from 1.5 to 2.5 μg/minute), 1 (20%) tolerated intraoperative reduction of support, and 3 (60%) were stable without adjustments of pharmacologic support. Two of the 7 patients not on inotropes or pressors were given intraoperative inotropes.
Mean difference >0 corresponds to a decrease in the parameter with laparoscopy.
Significant difference.
bpm, beats per minute; CI, confidence interval; HR, heart rate; MAP, mean arterial pressure; rpm, revolutions per minute.
There were no operative mortalities. Thirty-day survival and survival to discharge were 75% and 50%, respectively. Despite antiplatelet therapy and preoperative international normalization ratio of 2.2 ± 0.9, there were no re-operations for bleeding, and 50% did not require transfusion 48 hours before, during, or after surgery. Two patients with recent cardiac surgery had thromboembolic events: one stroke and one device thrombus. No patient had postoperative bacteremia, urinary tract infection, pneumonia, or driveline infection. Two patients had superficial surgical-site infections: one at the umbilical trocar site that resolved after opening of the incision and one at the gastrostomy tube site that resolved with local wound care.
Discussion
In the largest study to date describing the experience of laparoscopy performed on MCS patients, we found that laparoscopy was both feasible and safe to perform in MCS patients. Previous reports of applications of laparoscopy to MCS patients were similarly encouraging but were limited to single patient case reports and very small case series (Table 4). Although prior reports have stated that laparoscopy was well tolerated, our study is the first to report and quantitatively analyze whether hemodynamics and device parameters change with laparoscopy. Our sample represents a diverse cohort of MCS patients with multiple types of devices and inclusion of patients who were clinically stable or unstable prior to surgery.
BiVAD, biventricular assist device; HMII, Heartmate II; LVAD, left ventricular assist device.
We identified a small but statistically significant decrease in the pulsatility index associated with pneumoperitoneum. The pulsatility index is calculated as ([flowmaximum – flowminimum]/flowmean) × 10 and ranges from 1 to 10. It represents the magnitude of the flow pulse generated by an LVAD through each cardiac cycle and reflects the balance between ventricular contractility and the degree of unloading. The pulsatility index is dependent on LVAD speed and preload. The magnitude of the reduction in pulsatility index we observed (0.2) was less than our prospectively assigned threshold for clinical relevance of 0.5. Although the reduction was small in magnitude, this change was consistent with the effects of pneumoperitoneum described in non-MCS patients, which include preload reduction. If the pulsatility index were to decrease during laparoscopy in association with hypotension or reduced flow, appropriate responses include looking for bleeding, reducing insufflation pressures, leveling the bed if the patient is in reverse Trendelenburg position, giving volume, and obtaining an echocardiogram. In an otherwise hemodynamically stable patient with a decrease in pulsatility index, transesophageal echocardiography is a useful adjunct to assess for evidence of hypovolemia or right ventricular depression to further guide management.
We believe that a well-coordinated team approach to perioperative care is an important element in ensuring the best outcomes for MCS patients in need of abdominal operations. Our team approach included close coordination of perioperative care with the MCS team, as well as performing all operations with the assistance of cardiac anesthesiologists in a cardiac operating room with a perfusionist present and the cardiac surgeon immediately available if questions about device function or driveline positions arose. Modifications in traditional laparoscopic port placement are sometimes necessary to avoid the drivelines.
Decisions concerning perioperative management of anticoagulation and antiplatelet therapy should be based on the input of the MCS team and the operating surgeon. The 2013 International Society for Heart and Lung Transplantation guidelines for MCS patient requiring noncardiac surgery recommend continuation of anticoagulation and antiplatelet therapies if bleeding risk is low, holding with or without a heparin bridge if warranted by risk of bleeding, reversal of warfarin with fresh frozen plasma or vitamin K if needed for emergency procedures, and resuming anticoagulation and antiplatelet therapy when risk of surgical bleeding is acceptable. 3 Historically, coagulopathy was considered a contraindication to laparoscopy, but this has largely fallen out of favor as meticulous surgical technique and advanced instruments have facilitated the safe application of laparoscopy patients with cirrhosis and hematologic disorders. 21 Previous studies, in which open approaches were more frequent, described bleeding as the most common complication.8,9 Although the risk of bleeding could be a major limitation to performing laparoscopy on MCS, we did not find this to be a problem. In our series, we found that meticulous attention to hemostasis facilitated avoidance of withholding or reversing anticoagulation or antiplatelet therapy without leading to any re-operations for bleeding. Because MCS patients are at elevated risk of thromboembolic events, withholding or reversing anticoagulation and antiplatelet therapy could lead devastating complications, such as pump thrombosis or stroke.
Study limitations
Our study is subject to the inherent limitations of a small retrospective case series, although this series of 12 patients is considerably larger than any previous report (previous sample sizes, n = 1–3; Table 4). At the time of these operations, laparoscopy was our preferred approach for any abdominal operation in MCS patients, which reduces the potential for selection bias. Future randomized, prospective studies with an open laparotomy control group or retrospective comparisons of open and laparoscopic operations with propensity matching will be important to validate our findings.
Conclusions
Laparoscopy can be performed on MCS with low morbidity and mortality and minimal perturbations in hemodynamics and device function. This is the first study to quantify the effects of pneumoperitoneum for patients on MCS.
Footnotes
Acknowledgments
Disclosure Statement
F.A. is a consultant for SynCardia Systems. H.R., D.R., L.C., F.E., J.M., K.I., T.Y., N.D., and A.A. declare no competing financial interests exist.