
Abstract
Abstract
Background:
To analyze the early outcome of thoracoscopic repair (TR) of neonatal congenital diaphragmatic hernia (CDH) with standardized indications.
Methods:
Clinical data of 14 neonates with CDH who underwent TR from September 2013 to August 2014 were retrospectively analyzed. Selection criteria: weight beyond 2.0 kg; liver in the abdomen; no intestinal obstruction; no severe cardiopulmonary anomalies; not required high-frequency oscillatory ventilation or extracorporeal membrane oxygenation. Timing of surgery: mean arterial blood pressure normal for gestational age; preductal saturation levels of 85%–95% on fractional inspired oxygen below 50%; lactate below 3 mmol/L; urine output more than 2 mL/kg/h. Fourteen cases in the historical control group who underwent open repair (OR) with the same physiological status were reviewed for comparison.
Results:
Demographic features were similar between the TR group and OR group. The TR group had a higher intraoperative mean PaCO2 (48 ± 8 mmHg versus 39 ± 6 mmHg, P = .0024) and mean arterial pH (7.30 ± 0.06 versus 7.39 ± 0.06, P = .0005), but no differences in lactate (0.93 ± 0.16 mmol/L versus 0.98 ± 0.14 mmol/L, P = .3869). Longer operation time was found in the TR group (116 ± 27 minutes versus 74 ± 25 minutes, P = .0002). No recurrence was observed in groups within the first year of life follow-up.
Conclusions:
With selection criteria and timing, TR of CDH in neonates can be performed safely and successfully.
Introduction
T
Materials and Methods
Institutional review board approval was obtained to retrospectively review the charts of all neonates who underwent repair of Bochdalek-type CDH since May 2011, the beginning of application of standardized timing of surgery, according to the CDH EURO Consortium Consensus 10 : (1) mean arterial blood pressure normal for gestational age; (2) preductal saturation (SPO2) levels of 85%–95% on fractional inspired oxygen (FiO2) below 50%; (3) lactate below 3 mmol/L; (4) urine output more than 2 mL/kg/h. From May 2011 through August 2013, we used laparotomy approach in 17 cases with standardized timing of surgery. The selection criteria were concluded by summary of literatures6–9 and our experience in infantile CDH: (1) weight beyond 2.0 kg; (2) liver in the abdomen; (3) no intestinal obstruction; (4) no severe cardiopulmonary anomalies; (5) not required high-frequency oscillatory ventilation (HFOV) or extracorporeal membrane oxygenation (ECMO). From September 2013 through August 2014, we performed thoracoscopic procedure in 14 cases, considered as the study of TR group. There were 14 cases in the historical OR group, while three cases were excluded because of their liver herniation.
For thoracoscopic procedure, the patient was placed in the modified lateral decubitus position (more prone) with the affected side elevated (Fig. 1). The first port as scope site was placed in just below the tip of the scapula posteriorly. The other two working ports are then inserted under thoracoscopic visualization. The pneumothorax was slowly increased to 6 mmHg while monitoring for ventilator changes. The second port was placed at the medium between the scapular line and vertebral line from the level of the 5th to 7th intercostal space. The third port was inserted in the posterior axillary line from the level of 5th to 6th intercostal space (Fig. 2). The CO2 pressure was decreased to 2–4 mmHg after reduction of herniated organ. The diaphragmatic defect was identified and repaired with PROLENE or polyester fiber interrupted sutures. The posterolateral end of the defect was attached to the rib and thoracic wall when it was required. During the operation, the anesthesiologist continuously monitored vital signs and end-tidal CO2, and arterial blood gas assays were routinely used to analyze the PaCO2, pH, and lactate.
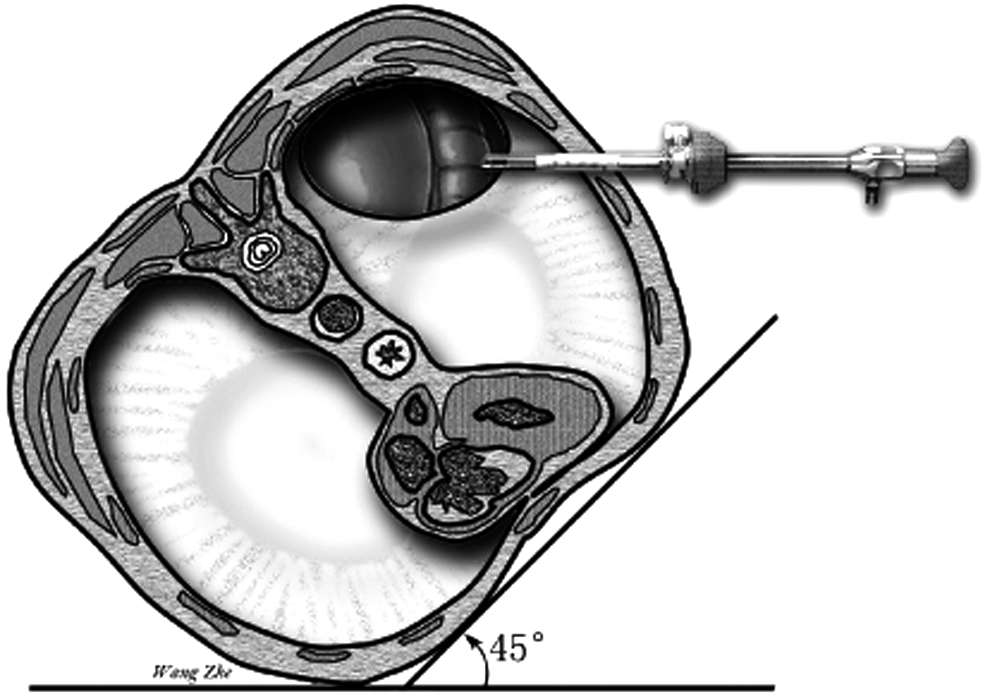
Illustration of modified lateral decubitus position (more prone) with the left-side diaphragmatic hernia.

Demonstration of trocar placement (scope site indicated by triangle; working port indicated by dot).
We analyzed continuous data using Student's t-test or Mann–Whitney U test with SPSS. Categorical variables were analyzed using χ2 or Fisher exact test. Significance was set at a P value of less than .05.
Results
In the TR group, 14 cases underwent surgery with standardized indications. In historical cases, there were 17 newborns experiencing the same timing with the TR group and three of them excluded to match the anatomic criteria (without liver herniation) as the TR group. The rest of the 14 cases were selected as the OR group for comparison in this study.
All data are shown in Table 1. There were no important differences in demographic and preoperative characteristics between the TR and OR group. During the operation, although the lactate did not differ between groups, those undergoing TR suffered hypercapnia, shown by higher mean PaCO2 and lower mean pH in the arterial blood gas test. There were no significant differences of area of diaphragmatic defect and rate of hernia sac between groups, but the patients in TR group had a longer mean operative time (P = .0002). The differences of mean ventilator time and mean duration to bowel movement recovery did not reach statistical significance.
OR, open repair; SD, standard deviation, TR, thoracoscopic repair.
The types of complications for the two groups are illustrated in Table 2. One thoracoscopic procedure was converted to open because of the bleeding of splenic laceration. No gastrointestinal perforation occurred in both groups. There was one case suffering pneumothorax in TR group as well as OR group. Wound infection was not found in TR but one in OR group. To better compare the earlier outcome in two groups, complications in the first year of life were analyzed. No recurrent case was observed in two groups. The incidence of bowel obstruction was same between the TR and OR group. One case suffered recurrent pneumonia at 5 and 10 months old in the TR group.
Follow-up within the first year of life.
Defined as more than twice pneumonia.
OR, open repair; TR, thoracoscopic repair.
Discussion
The feasibility to perform thoracoscopic CDH repair in neonates was first reported in 2003. 11 Later, Schaarschmidt et al. found that in a suitable neonate, TR and inflation-assisted reduction of thoracic contents were a more effective access to Bochdalek-type CDH than laparoscopy or laparotomy. 12 Shah et al. preferred thoracoscopy for neonatal Bochdalek hernias because of its better view with adequate working space, even without carbon dioxide (CO2) insufflations, due to hypoplastic lung and after reduction of the herniated organs.7,13 The application of TR for neonatal CDH has increased substantially over the past decade. However, a recent systematic review and meta-analysis showed that thoracoscopic CDH repair in neonates has higher recurrence rates and longer operative times, but similar survival and patch usage compared with open surgery. 3 Therefore, to gain good outcomes, it was suggested that CDH repair with thoracoscopy should be performed in the neonates with a small-sized diaphragmatic defect, stable hemodynamics, and without additional anomalies. 14 However, there is still lack of consensus for the indication of TR CDH in neonates. 5
The consensus of timing of surgery was reported in 2010
10
and it was applied in our medical center since 2011. The reasons for conversion and higher recurrence rate in TR included large diaphragmatic defect size, inability of visceral reduction, and solid organ laceration according to the retrospective studies with large samples (over 20 cases).15–17
Therefore, we concluded the standardized indications, including timing of surgery and selection criteria for starting TR CDH in neonates:
(1) Weight beyond 2000 g. There might be not enough working space in chest cavity in the babies with lower weight. Gourlay et al. have attempted to perform thoracoscopy in a 1.9 kg patient but failed finally.
18
In the retrospective studies, the weight of all the cases with TR successfully was beyond 2.0 kg.2,6,7,9,19 (2) Liver in the abdomen. Some reports have shown that liver herniation might be the most frequent reasons for conversion due to its association with a large-sized defect or inability of reduction.2,7,8 (3) No intestinal obstruction. The intestinal malformations were hard to be corrected thoracoscopically. Therefore, excretion of meconium should be observed before surgery and a gastrointestinal contrast study could be performed when necessary. (4) No severe cardiopulmonary anomalies. Severe cardiopulmonary status without adequate respiratory reserve might result in hypercapnia, acidosis, and contribute to the failure to tolerate thoracoscopy.
6
McHoney et al. have reported that the intraoperative mean PaCO2 and mean pH were similar between open and thoracoscopy groups when all patients with cardiovascular stability.
20
However, a recent pilot randomized controlled trial indicated that TR of CDH was associated with prolonged and severe intraoperative hypercapnia and acidosis compared to open procedure.
21
Interestingly, due to selection criteria, those TR cases in our study experienced mild hypercapnia and acidosis, although shown higher mean PaCO2 and lower mean pH compared with OR group. (5) Not required HFOV or ECMO. It was reported thoracoscopic repair was not safe and not easy when the patient with HFOV or ECMO.
8
In this study, 13 cases underwent TR successfully except one case converting to open because of splenic bleeding. Although the intraoperative mean lactate did not differ between groups, those undergoing TR suffered hypercapnia, indicated by higher mean PaCO2 and lower mean pH. The insufflation pressure has been considered to be associated with hypercapnia. Decreasing CO2 pressure after reduction of herniated organ might help to relieve the intraoperative hypercapnia. There were no differences in mean ventilator time and mean duration to bowel movement recovery in two groups. It suggests that there is no important impact in the recovery of pulmonary and intestinal function when newborns received thoracoscopy. No recurrence was found within the first year of life. There was one patient who suffered bowel obstruction at 10 months old in the TR group, and in retrospect, this case had been converted to open in the previous operation. One recurrent pneumonia was observed in groups. It seems that thoracoscopy might not affect the early outcome.
Some surgeons have found these selection criteria unnecessary over the past few years,2,18 some emphasized the stability of cardiopulmonary status before thoracoscopy, 9 and some developed the applicability of thoracoscopy in HFOV cases. 22 Nevertheless, it is believed that TR of neonatal CDH is safe and feasible when in the selected cases at the beginning of this procedure.14,19 The standardized indications in this study, including selection criteria and timing of surgery, could be a set of countermeasures that can be used for surgeons who still consider this technique as a deterrent to neonatal CDH. We do believe that a wider extension of thoracoscopic CDH repair in neonates may be acceptable with the improvement of surgical techniques and perioperative management. A randomized trial is still necessary to assess the effect of thoracoscopy on long-term outcome.
Footnotes
Acknowledgments
We appreciate the opinions we received when this issue was presented at the 48th Annual Meeting of the Pacific Association of Pediatric Surgeons, Jeju, South Korea, May 17–21, 2015, and Prof. Mike K. Chen from Children's of Alabama, Alabama, USA.
Disclosure Statement
No competing financial interests exist.