
Abstract
Abstract
Purpose:
Laparoscopic percutaneous extraperitoneal closure (LPEC) has been performed in Japan for the repair of the pediatric inguinal hernias for over a decade. However, the safety and efficacy of LPEC in neonates and infants under 1 year of age remain unknown. The aim of the present study is to elucidate the safety and efficacy of LPEC in the treatment of inguinal hernia in patients who are younger than 1 year of age.
Patients and Methods:
The medical records of the patients who underwent LPEC at Saga-Ken Medical Center Koseikan (Saga, Japan) between August 2007 and November 2012 were collected. The intraoperative findings and postoperative outcomes were retrospectively investigated. The data of the patients who were younger than 1 year of age (Group A) were compared with the data of patients who were older than 1 year of age (Group B).
Results:
During the study period, 150 LPEC procedures were performed in 112 Group A patients, whereas 607 LPEC procedures were performed in 456 Group B patients. There were no serious complications in either group. After a mean follow-up period of 50.4 ± 15.6 months (range, 28–91 months), there were no significant differences between the two groups in the operating time or the incidence of intraoperative or postoperative complications. Postoperative testicular ascent and recurrence were observed in some cases of each group.
Conclusions:
LPEC is a safe and effective procedure for the repair of an inguinal hernia, even in neonatal and infant patients who are younger than 1 year of age.
Introduction
I
Patients and Methods
Patients
We retrospectively investigated the medical records of 568 patients who underwent LPEC to repair an inguinal hernia between August 2007 and November 2012 at Saga-Ken Medical Center Koseikan (Saga, Japan). The patients were categorized into two groups: Group A was composed of 112 neonates and infants who were younger than 1 year of age, whereas Group B was composed of 456 patients who were older than 1 year of age. In the first 12 months of the present study, girls who were older than 3 years of age predominantly underwent LPEC procedures for training purposes. The operating time, intraoperative findings, and postoperative outcomes were evaluated. The data collection and analyses were carried out with the approval of the hospital's ethics committees.
Operative techniques
The LPEC procedure was performed as previously described. 11 During the study period, all of the procedures were performed randomly by three pediatric surgeons.
The patient was placed in the supine position under endotracheal general anesthesia. The operating surgeon stood on the left side of the patient; the assistant stood opposite the surgeon. A small longitudinal incision was made on the umbilicus to introduce an expandable port to gain access to the peritoneal cavity. Following the establishment of pneumoperitoneum by the insufflation of carbon dioxide (6 mm Hg; 1 L/minute flow), a 5-mm 30° telescope was inserted through an umbilical port.
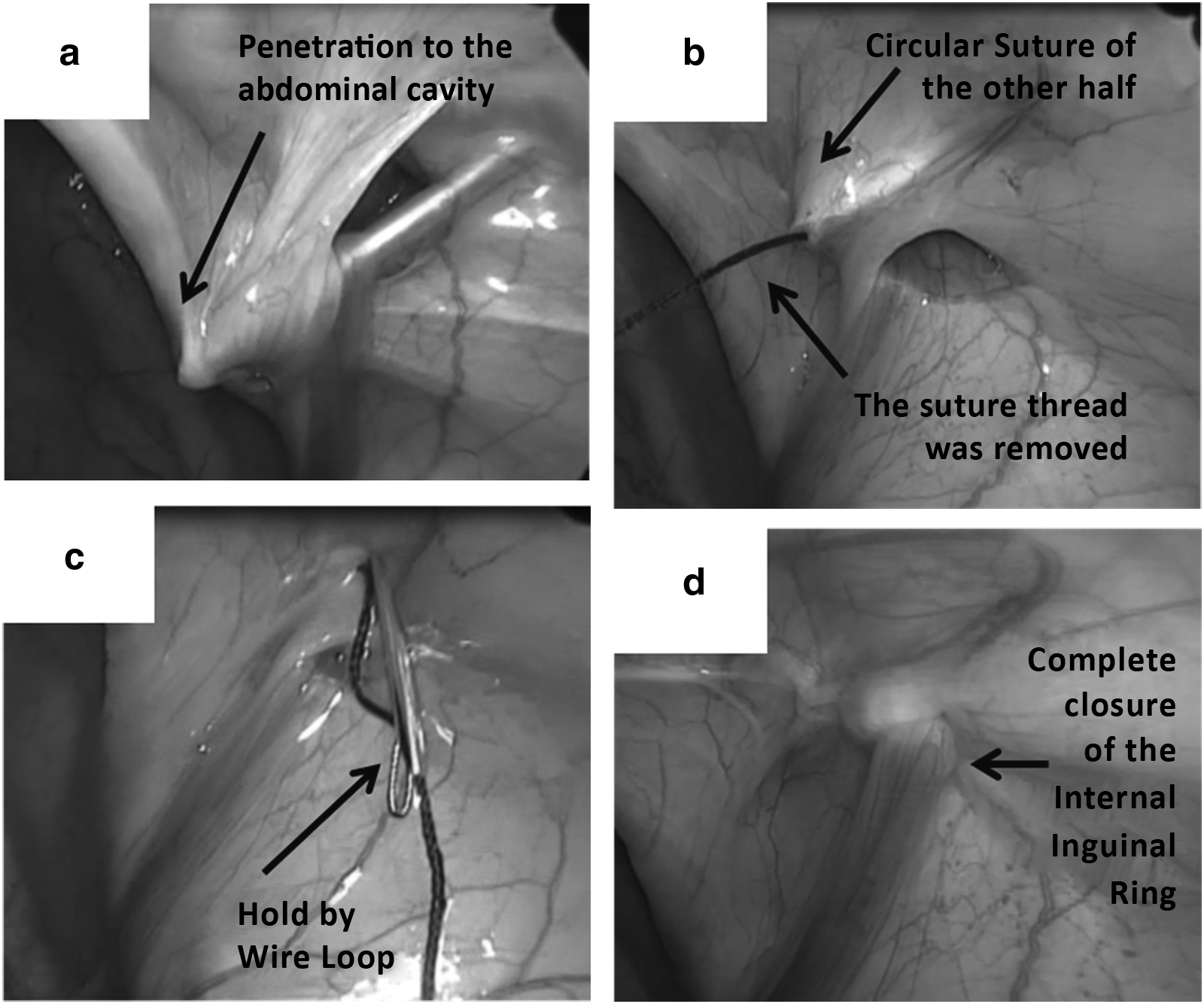
The patient was then placed in a slight Trendelenburg position, and a 19-gauge LPEC needle (Lapaherclosure™; Hakko Medical Co., Tokyo, Japan) with a wire loop holding a 2-0 nonabsorbable thread at the tip of the needle (Fig. 1) was inserted through the abdominal wall at the midpoint of the right or left inguinal line. The surgeons then extraperitoneally manipulated the LPEC needle (Fig. 2). For the circuit suturing around the internal inguinal orifice, extraperitoneal dissection was performed by the LPEC needle from the anterior to the posterior edge of the internal inguinal orifice. At the halfway point of the circuit suturing, the suture thread was temporarily removed from the needle in the abdominal cavity, and the LPEC needle was pulled to the anterior edge of the internal inguinal orifice and then pushed forward again (extraperitoneally) to the opposite side of the internal orifice. The suture thread was then picked up by the wire loop inside the LPEC needle, and both ends of the thread were pulled up together and tied extracorporeally. The internal inguinal ring was then completely closed (Fig. 3). During the closure of the internal inguinal orifice, great care was taken not to involve the spermatic ducts and vessels.
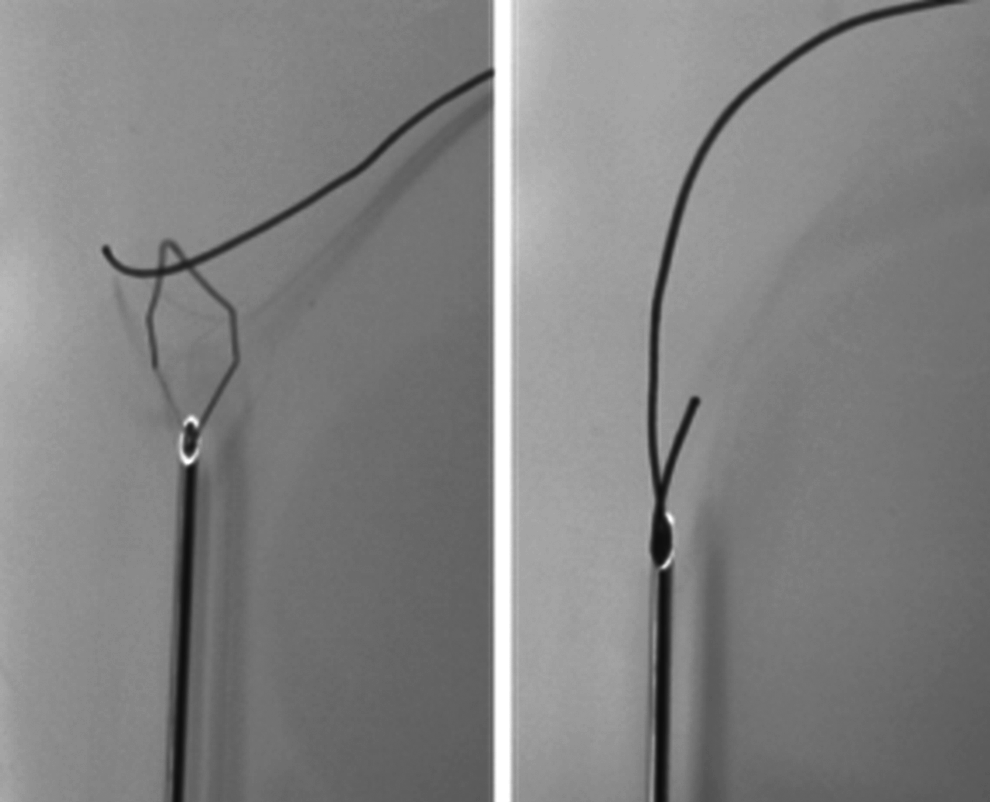
A 19-gauge laparoscopic percutaneous extraperitoneal closure needle (Lapaherclosure) with a wire loop at the tip of the needle threaded with a 2-0 nonabsorbable thread.

A 19-gauge laparoscopic percutaneous extraperitoneal closure needle threaded with a 2-0 nonabsorbable thread was inserted through the abdominal wall at the midpoint of the right or left inguinal line.
With regard to intraoperative positive contralateral processus vaginalis, the positive contralateral processus vaginalis was closed when air bubbles appeared from an open internal inguinal ring when the inguinal region was compressed, which suggested a remaining long processus vaginalis.
Statistical analysis
The results are expressed as mean ± standard deviation values. Fisher's exact test and Student's t test were used to evaluate the significance of the differences between Groups A and B. P values of <.05 were considered to be statistically significant.
Results
Patient characteristics and clinical details (Table 1)
The patients' characteristics and clinical details are shown in Table 1. During the 5-year 5-month period from August 2007 to December 2012, in total, 757 LPEC procedures were performed in 568 patients. The mean body weights of the patients in Groups A and B were 6.1 ± 1.8 kg (range, 2.4–11.6 kg) and 16.5 ± 7.4 kg (range, 7–53 kg), respectively. In Group A, the youngest patient was 22 days old, and the smallest body weight was 2.4 kg. In Group B, only 3 patients were older than 15 years of age. The rate of bilateral hernias was significantly higher in Group A than in Group B (P < .05), whereas the rate of contralateral patent processus vaginalis tended to be higher in Group B than in Group A (P = .07).
LPEC, laparoscopic percutaneous extraperitoneal closure.
Operative time in Groups A and B (Table 2)
The details of the operative time are shown in Table 2. The operative time, which was the time from the umbilical incision until wound closure, was evaluated in 87 cases in Group A and 433 cases in Group B. Cases in which the LPEC procedure was performed in combination with other operative procedures, such as orchidopexy for undescending testis, umbilicoplasty for umbilical hernia, and extraction of the urachal remnant and posthioplasty for phimosis, were excluded. There were no significant differences in the operative times of the two groups or in the operative times of male and female patients.
Time is in minutes.
Postoperative outcomes (Table 3)
There were no serious perioperative complications of Clavien-Dindo classification 12 Grade II or more in either group. The mean follow-up period was 50.4 ± 15.6 months (range, 28–91 months). There were no significant differences between the two groups in the rate of recurrence (P = .70), the rate of metachronous contralateral hernia in unilateral cases (P = .90), or the incidence of infective complications (P = .59). Umbilical port-site hernias occurred in both groups due to the insufficient closure of the umbilical fascia in early cases (P = .99). Postoperative testicular ascent was observed on the side of the operation at 11.6 ± 5.7 months (range, 7–21 months) after the LPEC procedure in 4 of 98 (4.1%) rings of males in Group A and 2 of 225 (0.9%) rings of males in Group B (P = .07). The ascending testes were located just above the scrotum and could be pulled into the scrotum manually; they did not quickly go up again after release. Transscrotal orchiopexy was successfully performed in each of these cases. During the orchiopexy, the remaining processus vaginalis was found to have adhered to the spermatic cord.
MCH, metachronous contralateral hernia; UPH, umbilical port-site hernia.
The postoperative cosmetic results were excellent in both groups (Fig. 4).

The excellent cosmetic results 1 month after laparoscopic percutaneous extraperitoneal closure.
Discussion
Laparoscopic inguinal herniorrhaphy has been successfully performed in children since the initial reports describing laparoscopic pediatric inguinal herniorrhaphy.3,13 Although some authors have reported a higher rate of recurrence in laparoscopic inguinal herniorrhaphy in comparison with traditional open surgery, many authors have reported the advantages of laparoscopic inguinal hernia repair in pediatric patients, which include a better esthetic outcome, less pain, early recovery, and a higher rate of detection of contralateral patent processus vaginalis (which reduces the rate of metachronous contralateral hernia in unilateral cases).14,15 In an analysis of the data from 2,699 pediatric patients identified in 10 comparative studies, Alzahem 14 reported a higher rate of recurrence in patients who underwent laparoscopic inguinal herniorrhaphy (4%) in comparison with those who underwent open herniorrhaphy (2%).
It has been suggested that neonatal inguinal herniorrhaphy is a potentially difficult procedure 16 and that the risk of damaging the spermatic ducts and vessels is considerably greater in male patients who are younger than 1 year of age because the elements are very small and the thin sac severely adheres to the vas and vessels. 17 An increased incidence of postoperative recurrence and testicular atrophy has been reported in infants younger than 1 year of age after traditional open surgery for inguinal hernia.16,18 Therefore a higher rate of complications, including the increased incidence of recurrence, was expected after laparoscopic inguinal hernia repair in the neonates and young infants of this age group. However, recent articles that described studies of laparoscopic inguinal hernia repair have shown a lower rate of recurrence and a rate of postoperative complications that is comparable to that in patients who are older than 1 year of age (Table 4).19–21 The reason for the lower rate of recurrence in younger patients remains unknown. These findings were similar to the results of our present study in which we found a relatively lower rate of recurrence in Group A (0.7%) than in Group B (1.6%) (P = .37). In the present study we found no significant differences between the two groups with regard to operation time, hernia recurrence, incidence of metachronous contralateral hernia, or other postoperative complications.
The characteristic findings in the postoperative outcomes were a higher rate of postoperative testicular ascent (4.1%) in the Group A patients than in the Group B patients (0.9%) (P = .07).
Several authors have reported the incidence of ascending testis after laparoscopic pediatric inguinal herniorrhaphy.19–21 Cho et al. 20 reported that 2.4% of patients younger than 1 year of age showed ascending testis after laparoscopic herniorrhaphy. Turial et al. 21 also found that 4.1% of infants who weighed less than 5 kg showed high testes that required orchiopexy after laparoscopic herniorrhaphy, although they could not determine whether the high testes were present but not detected at the time of surgery. They calculated a 65.5% increase in the risk of iatrogenic cryptorchidism for each 1 kg of body weight below 5 kg at the time of laparoscopic herniorrhaphy.
It has been suggested that iatrogenic cryptorchidism is caused by the severe adhesion of the spermatic cord in the inguinal canal due to the wide dissection during open herniorrhaphy procedures. 22 However, the cause of ascending testes after surgery is not well understood. The spermatic cord structures are not usually touched during laparoscopic hernia repair, 23 and Shalaby et al. 24 suggested that iatrogenic cryptorchidism is rarely seen in association with laparoscopic repair. This is reported to be due to the advantage of the magnified field of view during laparoscopic surgery, especially in infant patients.17,20 Cho et al. 20 reported that iatrogenic cryptorchidism might be caused by the overzealous tightening of the purse-string of the internal inguinal ring. Turial et al. 21 suggested that the clear etiology of undescended testes after hernia repair remained unknown, and they speculated that undescended testes might occur after surgery due to prematurity or low body weight at the time of surgery.
In the present study, 6 of 273 boys (1.8%) showed postoperative testicular ascent on the side of the operation: 4 (4.1%) of these were Group A patients, and 2 (0.9%) were Group B patients. In each of these 6 cases, testicular ascent was found at 7–21 months after the LPEC procedure. The 1 Group A patient with postoperative testicular ascent was an extremely low body weight infant (his birth weights was 478 g).
Cases of ascending or acquired undescended testes have been reported, in which the testes descend into the scrotum in early infanthood and later reascend out of the scrotum. 25 An abnormal fibrous remnant of the processus vaginalis or the persistence of processus vaginalis is presumed to cause ascending testes.26,27 The incidence of ascending testes has been reported to be 1%–2% in normal males. 25 In our study, the incidence of ascending testes was 1.8% of the male patients who underwent LPEC. We performed single scrotal incision orchidopexy, which was proposed by Bianchi and Squire 28 because it is known to be an effective procedure, with low rates of complications, for treating palpable testes.29,30 Regarding the long-term outcome of testicular function, testicular development remains satisfactory without a recurrence of ascending testis at 2–7 years after orchidopexy. Thus, the rate of incidence of ascending testes was similar to that of the normal male population. However, physicians should carefully examine postoperative patients, especially extremely low birth weight infants, for postoperative ascending testes because the remaining processus vaginalis may adhere to the spermatic cord. 11
The LPEC procedure was first reported by Takehara in 1995, as noted by Takehara et al., 4 and has been widely performed in Japan for the repair of pediatric inguinal hernias.5–11 In this procedure, a specific needle (the Lapaherclosure) is used to dissect the retroperitoneum under a magnified field of view. The internal inguinal ring is closed by extraperitoneal circuit suturing in the LPEC procedure, and there have been no reports of serious intraoperative or postoperative complications in relation to LPEC procedures (including from our own study).5–11 The present study suggests that LPEC is a safe technique regardless of the patient's age, body size, or the size of the abdominal cavity.
In conclusion, LPEC is a safe and effective procedure for neonates and infants younger than 1 year of age. The safety and efficacy are comparable to those achieved by laparoscopic herniorrhaphy in patients older than 1 year of age. Our results indicated that the postoperative outcomes in the patients who were younger than 1 year of age were not inferior to the outcomes of patients who were older than 1 year of age.
Footnotes
Acknowledgment
The authors thank Brian Quinn for his assistance with reading and editing the manuscript.
Disclosure Statement
No competing financial interests exist.