
Abstract
Abstract
Background:
Different techniques for ileal pouch-anal anastomosis (IPAA) following total proctocolectomy (TPC) have been described in patients with ulcerative colitis (UC), including rectal eversion (RE). RE allows for precise identification of the dentate line, but concerns have been raised regarding continence rates. No studies have specifically evaluated RE in the pediatric population. The purpose of this study was to evaluate the outcomes and continence rates for pediatric patients undergoing minimally invasive surgery (MIS) TPC and IPAA with RE for UC.
Materials and Methods:
All patients who underwent TPC and IPAA were reviewed at our institution. Data collected included demographics, proctocolectomy technique (open without RE versus MIS with RE), operative time, postoperative data, and continence outcomes following ileostomy closure.
Results:
Thirty-three patients were identified who underwent TPC and IPAA between July 2006 and October 2014. Thirty of these patients underwent ileostomy takedown and were evaluated for continence. Of these, 17 (56.7%) patients had a laparoscopic procedure, 5 (16.7%) had a robotic-assisted procedure, and 8 (26.7%) had an open procedure. There were no statistically significant differences in regard to demographics, operative time, or length of stay when comparing the two groups. There were no differences in the two groups as measured at 1, 6, and 12 months in terms of number of daily stools (P = .93, .09, and .87, respectively), nighttime stooling (P = .29, .10, and .25, respectively), soiling (P = .43, .36, and .52, respectively), or stool-altering medication usage (P = .26, 1.00, and .37, respectively).
Conclusions:
The RE technique can be used safely and effectively during MIS TPC and IPAA in children without altering continence rates.
Introduction
T
Most typically a three-stage approach with total abdominal colectomy, then completion proctectomy and IPAA with diverting ileostomy, and then ileostomy takedown is the preferred approach. 1 Minimally invasive surgery (MIS) techniques have gained popularity among adult and pediatric surgeons who care for patients with inflammatory bowel disease (IBD).1,13,14 However, difficulty completing the low resection and anastomosis necessary for TPC and IPAA has led to adoption of a technique involving rectal eversion (RE). 15 RE allows for precise identification of the dentate line and thus more complete proctectomy. Concerns have been expressed, however, that this technique may lead to increased traction injuries and decreased continence. 15 Additionally, this technique has not been specifically evaluated for safety and efficacy in the pediatric group.
The purpose of this work is to evaluate the outcomes of children with UC undergoing TPC and IPAA at a large freestanding pediatric institution specifically focusing on continence.
Materials and Methods
Patients
This retrospective cohort study included a review of all patients undergoing TPC and IPAA between 2006 and 2014 at a large, single-center pediatric institution. In 2009, the primary IBD surgeon at our institution began performing minimally invasive TPC and IPAA using the RE technique. Patient data are maintained in a prospectively collected database approved by our Institutional Review Board (approval number 12-00845). Data evaluated included demographic data (age, race, gender, body mass index), preoperative characteristics, intraoperative data (technique and length of operation), postoperative complications (length of stay, re-admissions, bowel obstructions), and continence data at 1, 6, and 12 months post–ileostomy takedown.
TPC and IPAA
Prior to 2009, the method of TPC and IPAA at our institution was open without RE. Beginning in 2009, all patients undergoing TPC and IPAA were treated by minimally invasive techniques using RE. Patients undergoing open techniques had previously undergone total colectomy with end ileostomy. The standard technique for the open group was ileostomy takedown, completion stapled proctectomy without RE, and IPAA creation with diverting ileostomy. Similarly, the MIS group had previously undergone total colectomy with end ileostomy. The MIS group had ileostomy takedown, followed by creation of the pouch extracorporeally through the ileostomy site, laparoscopic completion proctectomy, RE and stapling 2 cm above the dentate line, end-to-end stapled anastomosis, and diverting loop ileostomy.
Outcome measures
The primary outcome measure was continence as measured at 1, 6, and 12 months following diverting ileostomy takedown following TPC with IPAA. Secondary outcomes included length of surgery, postoperative length of stay, length of time from IPAA to ileostomy closure, re-admission rates, and postoperative complications.
Results
In total, 47 patients underwent TPC from 2006 to 2014. Thirty-three of those patients underwent IPAA, most commonly as a second-stage procedure. These patients were divided into two groups: MIS approach with RE (includes both standard laparoscopic procedures and robotic-assisted procedures) and open approach with intraabdominal anastomosis (without RE). Thirty-three of these patients had IPAA creation, and 30 of these had ileostomy takedown and were the focus of our study. Twenty-two of these (73.3%) had MIS techniques with RE, and 8 of these (26.7%) had an open technique without RE. Eighteen of the 22 (81.8%) MIS patients had UC, and 8 of 8 (100%) in the open group had UC. Of the MIS procedures, 17 (77.3%) were laparoscopic, and 5 (22.7%) were robotic-assisted. One patient (12.5%) in the open group ultimately required diverting ileostomy for medically refractory perianal disease. Figure 1 shows the breakdown of patients meeting inclusion criteria from the total patients evaluated.
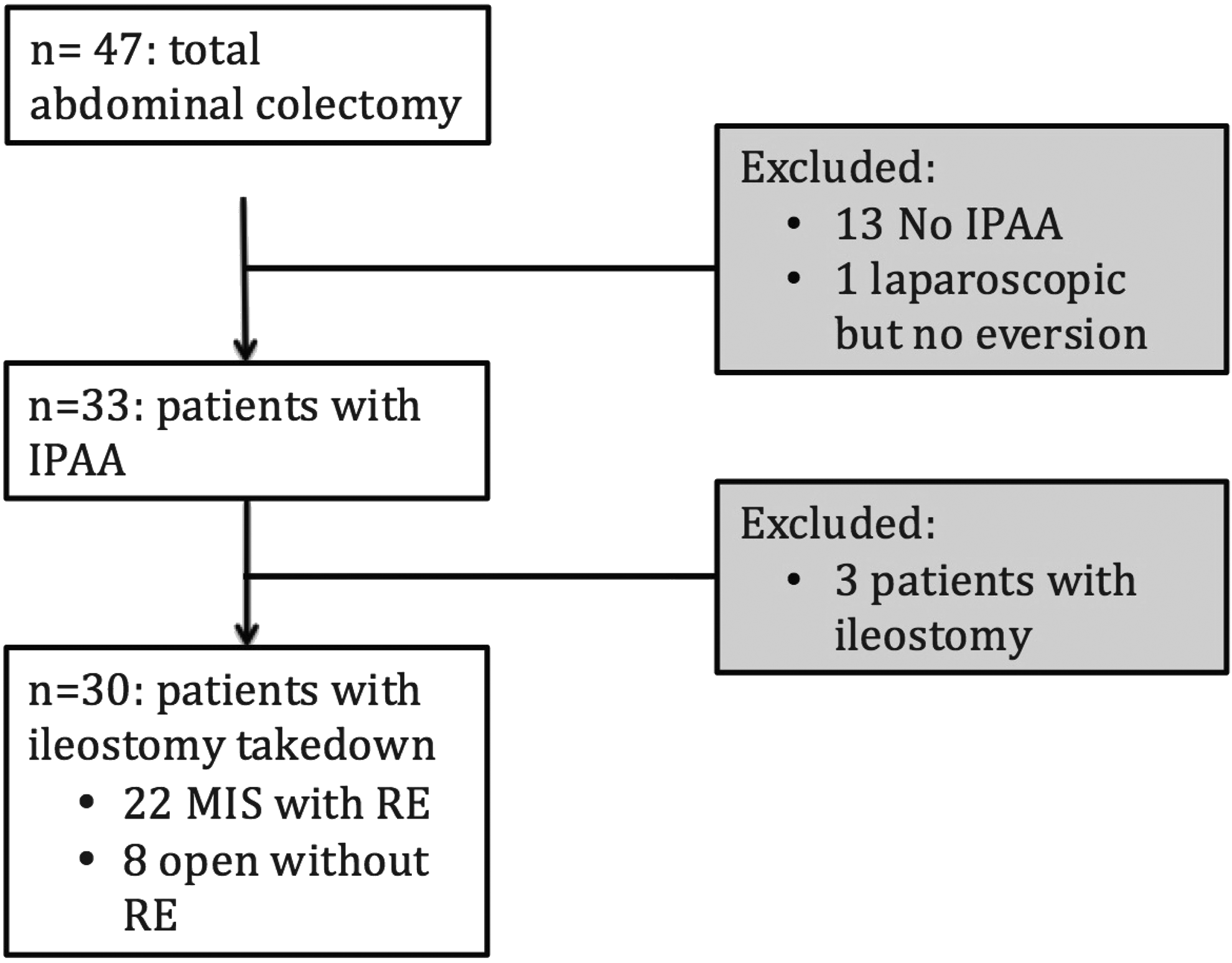
A breakdown of the patients meeting inclusion criteria for the study. Thirty patients underwent total proctocolectomy and ileostomy takedown and were evaluated for continence data. IPAA, ileal pouch-anal anastomosis; MIS, minimally invasive surgery; RE, rectal eversion.
Demographic data for the two groups were similar. There were no statistical differences in terms of age, body mass index, gender, and race (Table 1).
There are no statistically significant differences.
BMI, body mass index; MIS, minimally invasive surgery; RE, rectal eversion.
Operative data showed that the median length of surgery was 259 (± 67) minutes for the MIS group compared with 296 (± 14) minutes for the open group (P = .6). Median postoperative length of stay was 10.7 (± 10.1) days for the MIS group compared with 8.9 (± 1.9) days for the open group (P = .6). The time from IPAA to ileostomy takedown was 9.9 (± 8.4) weeks for the MIS group compared with 19 (± 16.4) weeks for the open group (P = .04).
The population of interest in this study was the 30 patients who went on to have ileostomy takedown and were evaluated for continence at 1, 6, and 12 months post–ileostomy takedown. Specifically the mean number of stools per day, percentage of patients stooling at night, percentage of patients with soiling, and percentage of patients requiring stool-altering medications were evaluated. Evaluating the MIS group versus the open group at 1,6, and 12 months showed no statistical difference in any of the outcomes at any time point (Table 2).
MIS, minimally invasive surgery; RE, rectal eversion.
Pouchitis occurred in 44% of the MIS patients compared with 50% for the open group (P = .77). Surgical-site infections were found in 8% of the MIS patients compared with 12.5% for the open group (P = .71). Re-admissions within 30 days occurred in 16.7% of the MIS group, and there were no occurrences in the open group (P = .23). Bowel obstructions occurred in 8.3% of the MIS patients compared with 12.5% of the open patients (P = .74).
Discussion
This study examined our initial experience with RE as a technique to aid in TPC with IPAA for restorative continence in medically refractory UC in a pediatric population. We found that combination of MIS techniques with RE is an effective tool with similar operative times, length of stay, and complications compared with open techniques without RE with equivalent continence outcomes. Stool-altering medications are the norm in both groups and are not statistically different. Soiling is rare in both groups at 1 year removed from the ileostomy takedown, and nighttime stooling decreases with time.
IPAA is the gold standard operation for patients requiring TPC for continence restoration and has a low side effect profile with overall good long-term continence, and even re-operative IPAA surgery has acceptable results whether performed locally or via abdominal approaches.11,16–19 MIS approaches are increasingly becoming popular for IBD in children as they are in adults. 20 MIS approaches for colorectal surgery have been found to be safe and efficacious with shorter hospital stays, better cosmesis, and fewer complications.2,21–24 There are variations and preferences for MIS restorative proctocolectomy with or without protective ileostomy and differing techniques for pouch creation with significant debate as to the best approach in the literature.2,14,17,18,20,25–27 Our preference is to perform a three-stage approach with laparoscopic total colectomy, followed by laparoscopic completion proctectomy and IPAA using RE with protective diverting ileostomy, and finally ileostomy takedown.
An important concern regarding RE techniques is the possibility of sphincter injuries resulting in long-term continence issues. Our study did not show any statistical difference in continence data with the RE technique using MIS techniques. Additional work by other groups has similarly indicated preserved continence with RE. An adult study of 50 patients with end-to-end ileoanal anastomosis by the eversion technique showed that as measured by anal manometry resting anal pressure and median thresholds for sensation in the lower third of the anal canal 1 year postoperatively were decreased; however, all patients were continent, with only 2 patients having leakage of mucus requiring a pad. 28 In agreement with our results, this adult series showed gradual improvement in bowel function with time. 28 There does appear to be some increased incontinence at multiple years following IPAA found in the adult literature, but there appears to be good overall satisfaction among patients.11,29–31 An additional single-institution study of 75 adult patients undergoing laparoscopic IPAA with RE using the assistance of a rectal tube stapled at the level of the rectosigmoid junction to aid in eversion showed no postoperative incontinence, and 34 of 40 patients (85%) with follow-up experienced no soiling. 32
Beyond continence issues, RE techniques have a good side effect profile. A large adult study of 507 patients undergoing IPAA comparing intramesorectal proctectomy with RE versus standard total mesorectal excision in patients with UC showed that the intramesorectal proctectomy/RE group had fewer perioperative complications, anastomotic leaks, and infections with no other statistically significant different outcomes, but continence data were not evaluated. 15
This study is limited by its small sample size and follow-up after ileostomy takedown is 12 months. Additionally, a single surgeon performed all MIS with RE operations, with the change in technique occurring in 2009. Surgical expertise and technique are crucial to the outcomes of any surgery, and alterations of technique and tissue handling could significantly change outcomes. To date, there have been no other studies evaluating MIS with RE techniques for TPC with IPAA in pediatric patients. Long-term follow-up with multicenter validation and larger trials are of utmost importance to validate our findings of preserved continence using RE. MIS techniques do require a learning curve, and operative times should diminish with improved mastery of this advanced laparoscopic or robotic-assisted technique.
Conclusions
This represents the first work to evaluate MIS with RE for TPC with IPAA in the pediatric population. MIS techniques with RE are safe, effective strategies in children with IBD for TPC with IPAA and allow for preserved continence. MIS techniques have overall similar safety profile, operative times, length of stay, and complication rates when compared with open techniques. Additionally, cosmetic results are significantly better using MIS techniques. RE carried out carefully can lead to excellent long-term continence outcomes and is an important tool in the armament of techniques for a minimally invasive IBD surgeon. Evolution in laparoscopic techniques, modifications of current strategies, and surgeon experience will only make these operations better and enhance surgical outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.