
Abstract
Abstract
Introduction:
Achalasia is an uncommon disorder in children. Currently, there is no consensus regarding the optimal treatment for achalasia. We investigate the effectiveness of symptom relief in patients who underwent endoscopic treatments versus Heller myotomy (HM).
Methods:
We conducted a retrospective review of all children (age 0–18 years) treated for achalasia at two pediatric hospitals from 2004 to 2014. Demographics, presenting symptoms, outcomes, and complications were analyzed.
Results:
Twenty-three patients (61% male) were identified with a mean age at diagnosis of 11.6 ± 5.0 years. About 47.8% of the cohort had no comorbidities. Common presenting symptoms included weight loss/failure to thrive (87.0%), emesis (69.6%), and dysphagia (69.6%). Mean time from symptom onset to diagnosis was 18 ± 18.9 months. Nine patients underwent laparoscopic HM as their primary treatment, whereas 14 received esophageal dilatation (ED) as their first-line therapy. Patients who underwent ED as their initial treatment were younger (9.92 versus 15.6 years, P = .047). Patients who underwent HM were more likely to attain symptom resolution compared to those managed with ED alone (P = .004). Of the 14 patients who underwent ED initially, 10 subsequently required HM due to persistent symptoms. None of the 4 patients who underwent ED alone achieved long-term symptom relief and, on the average, required an increased number of procedures compared to their HM counterparts (5.25 versus 2.47, P = .010). There was a trend toward increased intraoperative mucosal perforation in patients who underwent preoperative ED and botulinum injections.
Conclusion:
Our data suggest that HM is superior to balloon dilatation or botulinum injection in children with achalasia. We conclude that HM should be recommended for newly diagnosed children with achalasia as a first-line therapy.
Introduction
A
The presentation of achalasia in children can vary by age. Young children may present with reflux, nocturnal cough, hoarseness, apnea, pneumonia, feeding intolerance, and failure to thrive. Older children may exhibit symptoms similar to adults, which include progressive dysphagia, regurgitation of undigested food, vomiting, weight loss, and retrosternal chest pain. 7 This presentation can easily be confused with gastroesophageal reflux disease, feeding aversion, and failure to thrive and often leads to a delay in diagnosis. 8
The diagnosis of achalasia is established with a barium swallow, endoscopic evaluation, and esophageal manometry. The classic “bird's beak” appearance of a dilated proximal esophagus with gradual tapering toward the LES can be seen on barium esophagram. Endoscopy is helpful to rule out other esophageal pathology. Esophageal manometry is performed to confirm the diagnosis by demonstrating a lack of peristalsis, an elevated resting LES pressure, and a failure of the LES to relax with swallowing.6,7,9
The exact etiology of achalasia is unknown; furthermore, there is no known cure for the myenteric neurodegeneration. Treatment is directed at relief of the obstructive symptoms, which include medical management with calcium channel blocker (CCB), botulinum injection, esophageal dilatation (ED), and surgical intervention with Heller myotomy (HM). The results of botulinum toxin injection, ED, or HM as treatment for achalasia in children have been variable.2,7,8,10–14 Large studies aimed at evaluating treatment modalities for this disorder are difficult due to the rarity of the disease in children.
Although there is no consensus regarding the optimal treatment of children with achalasia, recent literature has touted the safety and efficacy of surgical intervention.7,8,15,16 We investigated symptom relief in patients undergoing HM compared to endoscopic modalities at two high-volume, stand-alone pediatric hospitals. We hypothesized that HM leads to improved symptom amelioration compared to endoscopic procedures.
Materials and Methods
Institutional Review Board approval was obtained for a retrospective review of patients with a confirmed diagnosis (esophagram, esophagogastroduodenoscopy, manometry) of achalasia (ICD-9 code 530.0) from September 1, 2004 to August 31, 2014 at two free-standing children's hospital in a major metropolitan area with a wide referral base. Patients were excluded if they were older than 18 years at the time of diagnosis, or if medical records were not available.
Patient demographics, presenting symptoms, duration of symptoms, endoscopic procedures, operative procedures, and outcomes were extracted from procedural, operative, inpatient and outpatient records. Patients were considered to have symptom alleviation if they no longer reported the preoperative symptoms at their most recent follow-up visit.
Statistical analyses were conducted using SAS v 9.2 (SAS Institute, Cary, NC). Descriptive statistics, chi-square test, Fisher's exact test, and unpaired t-test with Welch's correction were used for analyses wherever appropriate. Statistical significance was defined as P < .05.
Results
Demographics
We identified 26 patients with a confirmed diagnosis of achalasia by esophagram, upper endoscopy, and esophageal manometry. Three patients were excluded from the study (2 patients had their initial surgery performed at another institution and 1 was managed with CCB). The remaining 23 patients were included in the analysis. The mean age at diagnosis was 11.6 ± 5.0 years, 60.9% of the patients were male, and 47.8% of the children were without comorbidities. The most common associated anomalies included Trisomy 21 (3), mental retardation/developmental delay (3), Allgrove syndrome (1), scleroderma (1), and sarcoidosis (1) (Table 1).
MRCP, mental retardation/cerebral palsy.
The most common presenting symptom was weight loss/failure to thrive (80.7%), followed by emesis (69.6%), and dysphagia (69.6%). The mean time from the onset of symptoms to diagnosis was 18.0 ± 18.9 months (median 12 months; range 1–89 months). The average length of follow-up was 30.2 ± 30.7 months (median 24 months; range 1–124 months). There were no deaths related to achalasia in our cohort, and there were no esophageal perforations during endoscopic procedures.
Patients who underwent ED as initial treatment tended to be younger than HM patients (9.92 versus 15.5 years, P = .047). However, there were no statistically significant differences between the two groups with regard to comorbidities (P = .40) or duration of symptoms at presentation (HM 13.0 months versus ED 21.2 months, P = .26).
Initial treatment with ED
Fourteen patients underwent ED as their initial treatment (Fig. 1). None of these patients had symptom alleviation at their subsequent follow-up visits. Three patients were subsequently treated with endoscopic botulinum injection without ED; none had lasting symptomatic improvement. Ten of the 14 who were initially managed with ED ultimately underwent HM, whereas the remaining 4 continued with endoscopic treatment. None of the 4 patients treated solely by ED achieved long-term symptom relief.
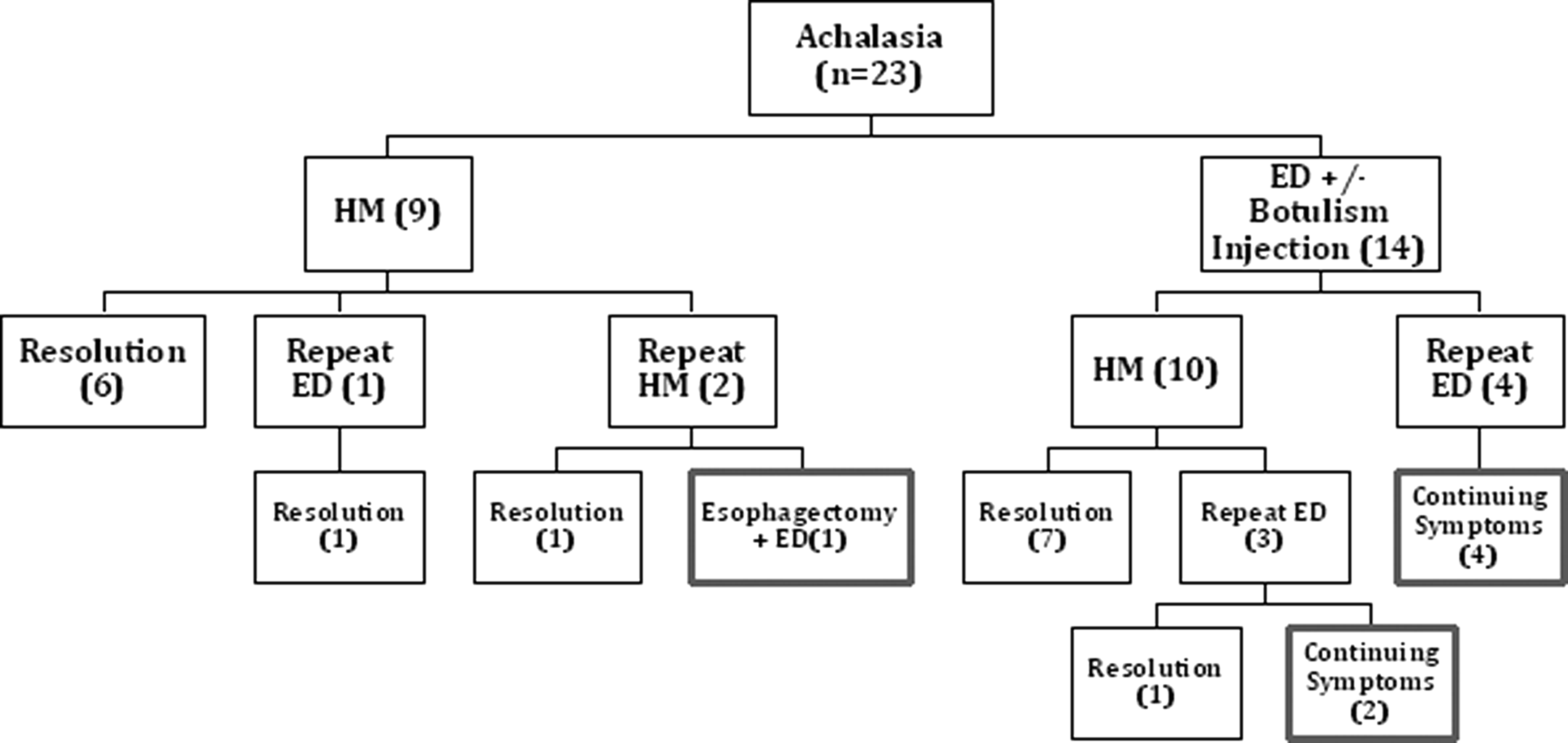
Outcomes after treatment modalities.
Initial treatment with HM
Nine patients underwent HM as initial management, performed by 8 surgeons. All HM were performed laparoscopically with a partial fundoplication per surgeon preference (5 Dor, 3 Toupet, 2 Thal). Of the 9 HM, 6 (66.7%) achieved symptom relief. Only 1 patient had a complication (mucosal perforation), which was identified and repaired intraoperatively. Routine postoperative care included advancement from clear liquid diet to full liquid diet after HM; in patients who required mucosal perforation repair, patients were kept nil per os (nothing per mouth) for 24 hours, followed by an esophagram to evaluate for extravasation before starting a clear liquid diet. Average length of stay was 6.5 (range 1–40) days.
Secondary treatments
Of the 14 patients treated initially with ED, 10 were referred for HM. The average interval between ED to HM was 8 months (range 2 weeks–2 years). Eight of these 10 who underwent HM achieved symptom relief. All but 1 of these patients undergoing HM had a fundoplication. Of the 19 HM patients, 5 required a single postoperative ED due to persistent dysphagia (Table 2).
ED, esophageal dilatation; HM, Heller myotomy.
Symptomatic relief outcomes
Overall, 84.2% of the HM patients achieved symptom relief compared to 0% in the ED patients at their most recent follow-up visits (P = .004). Of the 5 patients who underwent HM but did not have improvement in symptoms, 2 required repeat HM. One of these patients had a nonfunctional esophagus that ultimately required a minimally invasive esophagectomy and gastric pull-up. Overall, patients who underwent HM had, on average, 2.47 (range 1–5) total procedures including HM, compared to 5.25 (range 3–10) in ED patients (P = .010).
Risk of intraoperative complication
We conducted a subset analysis of intraoperative complication rates, notably mucosal perforation, in patients who had a preoperative intervention with ED or botulinum injection. Of the 19 HM patients, 10 had pre-operative intervention, of which 5 (50%) experienced an intraoperative mucosal perforation including 1 who also received botulinum injection. Of the 9 patients who underwent HM as their initial treatment, only 1 experienced an intraoperative perforation (RR = 1.4, CI 0.7449 to 2.631). All perforations were identified and repaired at the time of HM. Two patients required conversion to an open procedure after the perforation was identified. No long-term complications or prolonged hospitalization were attributed to the mucosal injury.
Discussion
The etiology of achalasia is largely unknown. As such there is no cure for the condition, and treatment is centered on relieving the obstructive symptoms. Due to the rare nature of the disease in the pediatric population, there are currently no consensus treatment guidelines.
Pharmacologic therapy with CCB has been used for short-term relief of symptoms with limited efficacy. 8 The mechanism of CCB involves inhibition of transmembrane calcium influx in smooth muscle. 6 Although well studied in adults, the use of CCB in children is sparse. Small studies have reported symptom relief in children who are treated with nifedipine before meals, likely attributable to decreased LES pressure. 17 To be effective, the medication must be taken before every meal; therefore, compliance is a concern.
Botulinum toxin can be injected into the LES to decrease acetylcholine release and decrease muscle tone. This therapy leads to transient benefit with a mean duration of symptom relief of 4 months.6,13 In adult studies, long-term relief has been reported in 10%–40%18–20 of patients, but such success has been limited in the pediatric population. Although botulinum toxin injection is a simple procedure to perform and does provide some symptom relief, it may lead to a more difficult dissection should the patient undergo a myotomy in the future. 16 Horgan et al. described the impact of botulinum toxin injection on esophagomyotomy, and noted that there was difficulty in dissecting the submucosal plane in 53.5% of patients who were treated with toxin injections before undergoing HM. They report a 13.3% intraoperative mucosal perforation rate in patients who were treated with toxin injection, versus 2.4% in those treated preoperatively with dilatation only. 21 Our data is too small to draw any conclusions regarding the risks of perforation. However, based on the operative description, it is probable that the patient who received botulinum toxin injection sustained a mucosal perforation due to difficulty of the dissection.
Endoscopic ED has gained considerable popularity as a primary treatment for achalasia. However, the results are highly variable. ED does provide symptom relief, but the benefit is often short-lived and patients invariably develop recurrence of symptoms, necessitating repeat interventions.2,10 ED may offer some advantages such as shorter length of stay, minimal recovery time, decreased cost per procedure, and may be used as a temporary treatment modality at some institutions; however, long-term results are poor.6,22,23 In our series, none of the 14 patients who underwent ED achieved symptom relief. Ten of these patients eventually underwent HM, with 80% attaining symptom resolution. The 4 patients who continue to receive nonoperative management remain symptomatic. Furthermore, it has been reported that dilatation may lead to increased mucosal perforation rates during subsequent myotomy.22,24,25 In our cohort, 50% who had ED before myotomy sustained mucosal injury, compared to 11.1% in patients who underwent a primary HM. Even though the results of our series are limited due to the small sample size and retrospective nature, the trend toward higher perforation rate is consistent with earlier reports.
A new modality known as peroral esophageal myotomy (POEM) is gaining popularity.26–35 This minimally invasive procedure combines the benefits of an endoscopic procedure with the outcomes of HM. 26 POEM has been reported to have shorter operative time, the ability to make a longer myotomy, and shorter length of stay. Pediatric POEM literature is limited, but outcomes appear similar to that of HM.26–29
Despite the increasing utilization of other modalities in the management of achalasia, we show that HM provides more reliable and lasting symptom relief. Nearly 85% of patients in our series achieved long-term symptom relief. Laparoscopic HM has been found to be safe and effective, and it is now being considered the surgical approach of choice in pediatric achalasia.2,6–8,10,11,14,15,36–38
In our series, HM was performed laparoscopically. All the patients had a partial wrap, either anterior or posterior depending on the surgeon's preference. Two of our patients required conversion to open due to mucosal perforations. The main reason for the conversions was due to the comfort level of the primary surgeon in managing the intraoperative complication laparoscopically. Overall, the mucosal injury rate was 31%. It is possible that the reason our series resulted in a higher rate of mucosal injuries is that a significant number of our patients received ED before HM. We feel that at large teaching institutions, inexperience may contribute, in part, to this finding.
Our study has a number of inherent limitations. It is a retrospective analysis of two institutions. Additionally, with multiple surgeons the practice guidelines are widely variable and lack standardization. The endoscopies and operations were performed by gastroenterologists and surgeons, respectively, including trainees. Therefore, there was a range of experience levels. Finally, even though our series is respectable compared to other published series about achalasia in children, the number is still small to draw a definitive conclusion.
Our data suggest that HM is superior to ED or botulinum injection in children with achalasia. We conclude that laparoscopic HM should be recommended for newly diagnosed children with achalasia as a first-line therapy. Further studies are needed to validate our findings.
Footnotes
Acknowledgments
We wish to thank the Department of Pediatric Surgery at Children's Hospital Los Angeles and the Department of Pediatric Surgery at Miller Children's Hospital, Long Beach Memorial Medical Center.
Disclosure Statement
No competing financial interests exist.