
Abstract
Abstract
Objective:
To evaluate the feasibility of Hem-o-lok clips tied with threads to improve surgical view in retroperitoneal laparoscopic surgery for renal cell carcinoma.
Materials and Methods:
Laparoscopic radical and partial nephrectomies performed by a single surgeon from May 2013 to April 2015 were reviewed. If Hem-o-lok clips tied with threads were applied to improve surgical view, the patient was recruited to the Hem-o-lok group. The other patients were recruited to the control group. Patient information, time of exposure procedure, number of clips used, number of trocars, exposure satisfaction, operation time, estimated blood loss, and perioperative complications were recorded.
Results:
Sixty-eight laparoscopic radical/partial nephrectomies were performed by a single surgeon. For 31 cases, Hem-o-lok clips were tied with threads to improve surgical view. For the other 37 cases, no Hem-o-lok clips were used. All cases were successfully performed. It took 30 to 178 seconds to finish the exposure procedure. In the Hem-o-lok group, less trocar usage, shorter operation time, and better exposure satisfaction were observed than control group (P < .05).
Conclusions:
This new technique is feasible and easy to improve surgical view in retroperitoneal laparoscopic surgery for renal cell carcinoma. This technique may be helpful to shorten operation time and avoid the use of the fourth trocar in certain cases. Large scale randomized controlled studies are needed to further prove its efficiency.
Introduction
R
Materials and Methods
Laparoscopic radical and partial nephrectomies performed by a single surgeon from May 2013 to April 2015 were reviewed. From May 2014 to April 2015, Hem-o-lok clips tied with threads were applied to improve surgical view. These patients were recruited to the Hem-o-lok group. Previous cases in which no such technique was applied were recruited to the control group.
General procedure
After general anesthesia was administered, a patient was placed on full flank position. The body was then flexed to expand the distance between iliac crest and the tip of the 12th rib, and appropriate padding was applied. A skin incision was made 2–3 cm above the iliac crest in the midaxillary line. The retroperitoneal space was bluntly created with a self-made balloon. A 12-mm trocar was used to tunnel through the subcutaneous adipose tissue, muscles, and lumbodorsal fascia to the retroperitoneal space. Under 14 mmHg of carbon dioxide and direction vision, the other two trocars were placed in the anterior and posterior axillary line below the costal arch, respectively. A fourth trocar was placed in the anterior axillary line below the upper trocar when additional assistance was needed. Retroperitoneal fat was first removed. Gerota's fascia was then opened from the upper pole to lower pole of the kidney. Renal hilum was posteriorly approached between psoas muscle and pararenal fat. For radical nephrectomy, renal artery was mobilized and ligated. The kidney was fully mobilized and the renal vein was ligated. For partial nephrectomy, renal artery was mobilized. The kidney was mobilized and the mass was exposed. Renal artery was clipped with a bulldog clip. The mass was removed, the kidney was reconstructed, and the bulldog clip was removed. The Hem-o-lok clips on Gerota's fascia were removed and taken out.
Key technique details
For the Hem-o-lok group, Hem-o-lok clips were tied with No. 7 silk threads before surgery. After mobilizing renal artery, Hem-o-lok clips tied with silk threads were clipped on Gerota's fascia. One or more clips were clipped onto Gerota's fascia where maximum exposure may be provided. A crochet needle was inserted through the Trocar to grab the tail of the thread. The crochet needle was retreated to take out the thread. The thread was fixed with a vessel clamp. The thread tail could also be taken out through the port with dissecting forceps (Fig. 1). For control group, no Hem-o-lok clips were used to improve surgical view.

The thread tail was taken out through the port and fixed with a vessel clamp.
Outcome measures
Patient information, time of exposure procedure, number of clips used, number of trocars, operation time, estimated blood loss, and perioperative complications were recorded. Exposure satisfaction was evaluated by the surgeon on the ascending scale from 1 to 10.
Statistical analysis
All data were analyzed using SPSS version 16.0 for Windows (SPSS, Inc., Chicago, IL). Data were expressed as mean ± standard deviation. Independent student t test was applied for comparison between the two groups. Chi-square test was used for nonparametric analysis. P < .05 was considered statistically significant.
Results
From May 2013 to April 2015, 68 laparoscopic radical/partial nephrectomies were performed by a single surgeon. For 31 cases, Hem-o-lok clips were tied with threads to improve surgical view (Hem-o-lok group). For the other 37 cases, no Hem-o-lok clips were used (control group). All cases were successfully performed. Patient information is shown in Table 1. The patients are comparable in age, sex, tumor size, ASA score, and so on. In the Hem-o-lok group, only one clip was used in 28 cases. In three cases, two clips were used. The mean time of the exposure procedure was 72 seconds (range 30–178). Operative pictures before and after the exposure are shown in Figure 2. In the Hem-o-lok group, few trocars were used and shorter operation time was observed. In addition, the surgeon experienced better surgical field and exposure (P < .05). Perioperative information is shown in Table 2.
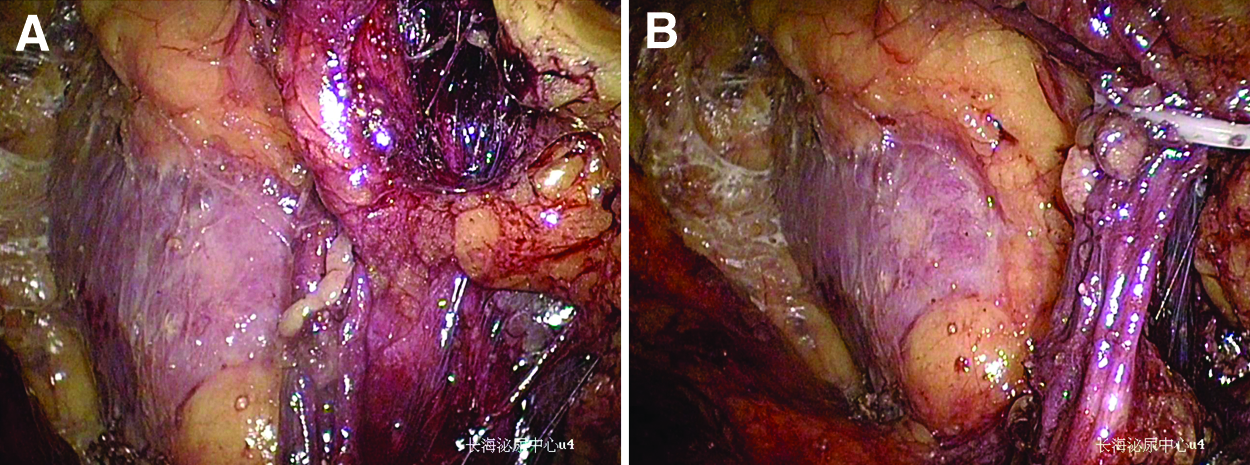
Effect of Hem-o-lok exposure.
Operation time was from skin to skin.
Discussion
In 1991, Clayman et al. performed the first laparoscopic nephrectomy. 5 Since then, this technique has been increasingly used and has become a common procedure to treat localized renal cell carcinoma. Laparoscopic radical/partial nephrectomies are mainly performed through transperitoneal or retroperitoneal approaches, and each approach has its advantages. In the transperitoneal approach, the anatomy is easy to comprehend, the surgical space is sufficient, and the requirement for traction of the left hand is relatively low. These features make the surgery especially suitable for beginners. However, in contrast, it also leads to longer operating time and longer hospital stay because of the involvement of ascending/descending colon during surgery.6,7 The advantages of the retroperitoneal approach are obvious. Comparing with the transperitoneal approach, it is relatively easy and takes less time to mobilize and control renal artery. For big tumors, the earlier the renal artery is controlled, the easier and safer the surgery will get. It may also be related with shorter overall operating time and hospital stay. Besides, it does not disturb abdominal organs, resulting in a lower complication rate and faster postoperative recovery. 8 This approach is widely accepted by surgeons despite the fact that intraoperative exposure is often inadequate. Retroperitoneal space is an artificial space created by surgeons. It is small, which makes the surgery more difficult. Where to incise Gerota's fascia is important. Too close to ventral side may cause injury of the peritoneum. Therefore, many surgeons prefer to open it posteriorly.9,10 However, because of the impact of Gerota's fascia, excellent intraoperative exposure is not easily achieved. When mobilizing ventral side of the kidney, the kidney is usually covered by Gerota's fascia. In this circumstance, the surgeon may either proceed with discomfort or add an additional trocar to help with the retraction.
In our series, we used Hem-o-lok clips to improve the surgical field when exposure is insufficient, especially when performing partial nephrectomy to treat ventral side masses. During these cases, the surgeon must mobilize the kidney on the ventral side to the best of his ability. A fourth trocar is of great help during mobilization as well as cut and reconstruction of the kidney. However, in our study, it normally took 1 minute or so (range 30–178 seconds) to finish the exposure procedure with Hem-o-lok clips. The whole procedure was fast and easy. In the Hem-o-lok group, only three trocars were used in 90.3% (28/31) of the cases, leading to less help from the assistant, less medical expenses, and better cosmetic results (P = .038). Also, shorter operation time was observed in the Hem-o-lok group (P = .047), which may be related to better surgical exposure (P < .001).
There are some tips that we should pay attention to while doing this procedure. (1) Hem-o-lok clips should be clipped to the fascia where exposure is needed most. (2) The crochet needle should be inserted under direct vision to prevent unnecessary injury to the peritoneum. When the path of the crochet needle could not be judged precisely, it may be helpful to use the needle of a 5 mL syringe to puncture the abdominal wall first. (3) We should grab the tail of the thread and take it out. Otherwise the thread may not be long enough for the crochet needle to get out.
In conclusion, it is feasible and easy to use Hem-o-lok clips tied with threads to improve surgical view in retroperitoneal laparoscopic surgery for renal cell carcinoma. This technique may be helpful to shorten operation time and avoid the use of the fourth trocar in certain cases. Large scale randomized controlled studies are needed to further prove its efficiency.
Footnotes
Disclosure Statement
No competing financial interests exist.