
Abstract
Abstract
Aim:
The role of intracorporeal anastomosis (IA) in right colectomy is still controversial. Primary endpoint of the present study is to evaluate the impact of IA versus extracorporeal anastomosis (EA) on recovery of bowel function and length of stay in right colon cancer patients.
Materials and Methods:
Adult patients with histologically proven cancer of the right colon were randomized to laparoscopic right colectomy with IA or EA anastomosis. Admitting a two-sided type I error level of 0.01 and an estimated power of 80%, 79 patients for each group were needed to test the primary endpoint.
Results:
At the time of this interim analysis, 60 patients were randomized; 30 were assigned to the IA group and 30 to the EA group. The two groups were homogeneous with respect to demographics, American Surgical Association score, and tumor stage. In the IA group, a longer operating time (P = .04), an earlier recovery of bowel function (P = .048), and a lower incidence of postoperative ileus (P = .05) were observed. No differences were observed between the two groups with respect to length of stay (P = .70) and complication rate (P = .89). Anastomotic leak rate occurred in two patients in the IA group, while no leak occurred in EA.
Conclusions:
Intracorporeal anastomosis could be considered a valuable option in the hands of expert surgeons, with favorable effect on recovery of bowel function and postoperative ileus. Definitive answers on its safety and efficacy will be given once the present randomized controlled trial (RCT) will be complete.
Introduction
L
Materials and Methods
Adult patients of both sexes with a histologically proven diagnosis of tumor of the right colon were assessed for study eligibility. Tumor classification was by the seventh edition of TNM. Exclusion criteria were emergency surgery, presence of a fixed palpable mass, cancer infiltrating an adjacent organ (assessed by computed tomography or magnetic resonance imaging), severe cardiovascular disease (New York Heart Association class higher than 3), respiratory dysfunction (arterial PO2 < 79 mmHg), hepatic dysfunction (Child-Pugh class C), American Surgical Association (ASA) class higher than 3, presence of ongoing infection or infective chronic diseases, presence of collagen diseases, or current corticosteroid therapy or a history of corticosteroid therapy within 6 months before surgery. The protocol was approved by the Ethics Committee of the IRCCS San Raffaele (Milan, Italy) and registered on ClinicalTrials.Gov (Clinical trials Gov; NCT01453556). The enrollment to the study started in October 2012. The protocol was fully explained to all participants, who signed a written informed consent document before randomization.
Patients were randomly assigned to EA or intracorporeal anastomosis (IA) by a computer-generated, blocked randomization list. A block size of four was used to balance both the treatments and the surgical procedures. The investigator who generated the randomization sequence was independent from the research staff. Assignment was double-blinded with respect to treatment. Sealed sequenced envelopes that were opened 120 minutes before surgery were used for assignment. On hospital admission, the following variables were considered: age, gender, site of tumor, ASA score, and body mass index. No patient received bowel preparation before surgery. All patients received a single dose of cefotetan (2 g IV) during anesthesia induction for antibiotic prophylaxis. A second dose of the same antibiotic was administered if surgery lasted more than 4 hours. All patients also were given low-molecular-weight heparin (enoxaparin 4000 IU/day) as prophylaxis against deep vein thrombosis. Three surgeons with extensive experience in laparoscopic and open colorectal surgery (A.V., C.S., S.D.P.) performed all operations. All patients were given the same postoperative analgesic. All patients received a thoracic epidural catheter at T-9 to T-10. A thoracic epidural block was then induced with 6–10 mL of 0.75% ropivacaine and maintained by injecting 50% of the induction bolus every 90–120 minutes (0.5 mg/kg/hour). Postoperative analgesia consisted of a continuous epidural infusion with 0.2% ropivacaine (infusion rate, 4–6 mL/hour) and 100 mg of ketorolac IV every 8 hours for the first 3 days. To maintain normotermia, active intraoperative warming (forced-air warming at 38°C on the thorax and upper limbs plus on-line heating) was instituted. All patients were treated according to the same postoperative care protocol, which included epidural analgesia maintenance for 3 days, removal of the nasogastric tube at the end of surgery, and removal of the bladder catheter on postoperative day (POD) 1. Postoperative infusion of fluids and electrolytes was given according to clinical requirement. A clear liquid diet was started on POD 1 as tolerated by the patient. Oral solid food was given after the first flatus occurred. The following details of the surgical procedure were recorded for all patients: duration of operation, operative blood loss, time to fashion the anastomosis, difficulty to close the mesenteric defect, and homologous blood transfusion rate. The number of lymph nodes intraoperatively retrieved was also recorded in all patients. Occurrence of the first flatus and recovery of bowel function were recorded in all patients. Postoperative ileus was defined as the absence of any bowel function after POD 3 without evidence of any precipitating complications according to a clinical consensus statement. 12 All infectious complications were confirmed by microbiologic analysis and culture. Complications were registered by members of the staff not directly involved in the study. Patients were discharged after occurrence of a bowel movement and full recovery of both ambulation and oral feeding. Complications and unexpected readmissions were recorded for the first 30 days after surgery.
Surgical technique
In both groups, four trocars were placed. After diagnostic laparoscopy, the ileocolic vessels were identified and divided at their origin after applying hemostatic clips or mechanical staplers. The colon was then mobilized; the right ureter and the duodenum were routinely identified. In case of EA, the division of the mesentery and colon was carried out extracorporeally as the mechanical anastomosis. The ileum was divided intracorporeally in both groups.
Intracorporeal anastomosis was fashioned by firing one 60-mm linear stapler load in an isoperistaltic side-to-side manner. A careful inspection of the anastomosis was done to exclude bleeding. The enterotomies were closed with two layers of running Vicryl sutures. EA was fashioned in the same manner. The defect between the mesentery and the mesocolon after an ileocolic anastomosis was closed using a 3-0 running Vicryl suture in both groups. A periumbilical midline incision was used for specimen retrieval in both groups. Drains were not routinely placed in both groups.
Conversion to open surgery was defined as the need to perform an abdominal incision longer than 7 cm or an incision different from that planned at the beginning of the case.
Postoperative pain
Thoracic epidural analgesia (TEA) catheter was checked every day by the anesthetic pain service and removed on day 3. Postoperative pain was evaluated by the same team at rest at 12-hour intervals from the day of the surgery until the patient was discharged home using a visual analog scale (VAS) ranging from 0 to 10 (0 = no pain, 10 = maximal pain).
Statistical analyses
The sample size was calculated to detect a difference in the standard deviation (SD) between the two groups of 50% or more in recovery of bowel function and length of stay. Admitting a two-sided type I error level of 0.01 and an estimated power of 80%, 79 patients were needed for each group in the study. A statistician blinded to randomization and allocation performed all statistical analyses, which were done in accordance with a pre-established analysis plan. Descriptive data are reported as mean (SD) and range or number of observations. Comparisons between groups were made using Student's t-test for continuous normally distributed variables, and the Mann–Whitney U test was used for non-normally distributed variables. Comparisons between groups for discrete variables were made using the chi-square test or Fisher's exact test as appropriate.
Results
At the time of this interim analysis, a total of 60 patients have been enrolled in this ongoing study. Figure 1 shows the diagram of the trial, which was designed according to the recommendations of the Consolidated Standards of Reporting Trials (CONSORT) statement. Of the 60 patients randomized, 30 were assigned to the IA group and 30 to the EA group. No patient was converted to EA or open colectomy.
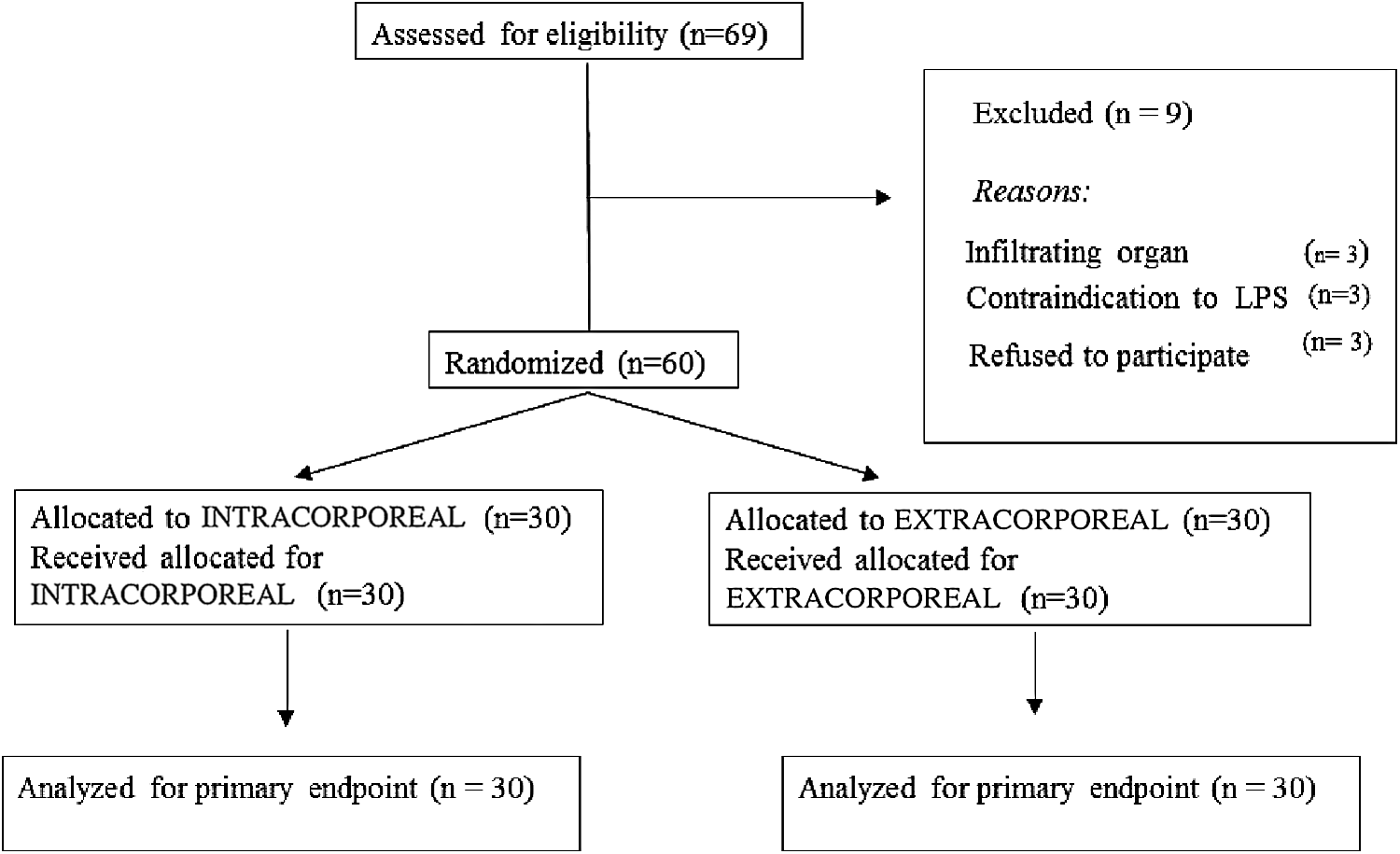
Diagram of the trial, according to the recommendations of the CONSORT statement. CONSORT, Consolidated Standards of Reporting Trials.
The two groups were well balanced for demographics, preoperative clinical characteristics, age, body mass index, ASA score, tumor site, and stage (Table 1). With respect to operative variables, patients in the IA group experienced a higher operative time, a longer time necessary to construct the anastomosis, and a shorter incision length (P = .04, P = .01, P = .01; respectively). Moreover, in the IA group, no operative difficulty to close the mesenteric defect was encountered, while it occurred in 10% of the patients in the EA group (Table 2).
Only abdominal surgeries were included.
Values are reported as mean (SD) or percentages (%).
ASA, American Surgical Association.
A similar length of postoperative stay was observed in the two groups. Patients in the IA group experienced a trend toward an earlier recovery of bowel function (P = .06). In the same group, an earlier stool canalization occurred when compared with the EA group (P = .048) (Table 3).
Overall, VAS pain scores were not statistically different between the two groups in the first three days following surgery. After TEA removal (on day 3), a similar trend was maintained (Table 4).
POD, postoperative day.
All postoperative complications are summarized in Table 5. The overall 30-day morbidity rate was 30% in the EA group and 26.6% in the IA group, with no statistical differences between the two treatment groups. No significant difference was observed between the two groups with respect to infectious and noninfectious complications, as well as for technical complications.
In the EA group, paralytic ileus occurred in 23, 3% (n = 7 patients) of cases, while it occurred in 3.3% (n = 1) of the cases in the IA (P = .05). Intestinal obstruction occurred in 6.6% (n = 2) of patients in the EA group and in 3.3% (n = 1) of patients in the IA group (P = .89).
Anastomotic leak occurred in two patients (6.6%) in the IA group, while no leak occurred in the EA group. Both patients with anastomotic leak were managed surgically. One patient in the IA group died in the postoperative period due to the sequelae of an anastomotic leak. Among the two patients in the EA group who developed postoperative bowel obstruction, a reoperation was necessary due to an abdominal abscess, which was not amenable to percutaneous drainage (n = 1), and an internal hernia due to a failure in the mesentery closure at the anastomotic site, which occurred once the patients were discharged at home on POD 9 (n = 1). This latter one was the only 30-day hospital readmission we experienced (3.3%). The patient with bowel obstruction in the IA group was successfully treated with conservative management.
A similar oncologic radicality in terms of number of lymph nodes intraoperatively harvested was obtained in the two groups (21.5 ± 9.8 in the IA versus 22.4 ± 12, four in the EA group; P = .38). In all patients, negative margins were obtained.
Discussion
There is a relative paucity of data in the literature concerning the adoption of intracorporeal anastomosis following laparoscopic right colectomy. At the present time, the majority of surgeons prefer to fashion an EA, which has been reported to be less technically demanding, and do not require to perform intracorporeal hand-sewn sutures. However, a growing interest in intracorporeal anastomosis following laparoscopic right colectomy has recently emerged. Four meta-analyses, including mainly retrospective or case–control series, have been published in the last 2 years, reporting benefits for intracorporeal anastomoses in terms of early postoperative outcomes with no adverse effect in terms of anastomotic leak and overall postoperative complications.13–16 Definitive conclusions, however, are difficult to draw due to the nature of the studies included and the high heterogeneity of surgical techniques used in fashioning the EA, including both manual, totally stapled, and stapled–manual. The same heterogeneity was also observed for mesentery closure and type of incision used for specimen removal.11,13–16 To the best of our knowledge, this is the first RCT study analyzing the role of intracorporeal stapled versus extracorporeal stapled anastomosis following laparoscopic right colectomy using a standardized approach.
In the present interim analysis, a significant lower incidence of paralytic ileus and a trend toward an earlier recovery of bowel function have been reported in the intracorporeal group when compared with the EA group, while no difference was observed with respect to the length of stay, which, with the two aforementioned variables, constitutes the primary endpoints of the present study. With respect to bowel movement, our findings confirm previous authors' experience, despite high heterogeneity being reported.6–10,17–19 Milone et al. in the largest multicenter study comparing IA and EA, including 512 right-sided colorectal cancer, reported a significantly lower time to first flatus in the IA group, while no difference was observed with respect to stool canalization. 4 On the other hand, an earlier recovery of stool canalization in the IA group has been reported by Anania et al. 20 and Chaves et al. 21 in two case–control studies comparing IA and EA.
With respect to postoperative ileus, contrasting results have been published so far, favoring IA, EA, or reporting identical results in the two groups with figures ranging from 10.6% to 23%.8,10,17,19 However, in no case, the difference between the two groups reached statistical significance. A possible explanation in the wide variability of the reported results lies in the heterogeneity in the definition of postoperative ileus as stressed by Carnuccio et al. in a recently published meta-analysis, including 484 patients. 13 The significant favorable results reported in the present series in terms of paralytic ileus and earlier recovery of bowel function in the IA group could be ascribed to the reduced manipulation of the abdominal organs and to the related traction sometimes necessary to exteriorize a heavy and large specimen through a small laparotomic incision. This is particularly true in obese patients with thicker abdominal wall and short mesentery.13–15 Moreover, the smaller incision used for specimen extraction observed in the IA group could have also contributed to reduce postoperative ileus. 22 Differently from other authors, we experienced a similar postoperative pain in the groups in the study.8,21 A possible interpretation lies in the fact that we used the same incision to extract the specimen to avoid possible bias in the data analysis.
One controversial issue of intracorporeal anastomosis following laparoscopy (LPS) right colectomy is the longer operating time. In the present series, a longer operating time has been reported in the IA group. This finding is in line with the experience of the majority of authors as emerged in a recent meta-analysis by Feroci et al. 15 This probably reflects the difference in the experience or skill level of the operator or an incomplete learning curve for intracorporeal anastomosis. Before starting the present RCT trial, the surgical team who had extensive experience in laparoscopic colectomy performed 20 cases of IA and experienced no conversion to extracorporeal or open right colectomy (data not shown). This trend was also maintained in the trial, with no conversion occurring. However, the two anastomotic leaks experienced in the IA group suggest for a longer learning curve required for this technique, as stressed by Jamali et al. in a survey conducted among surgeons. According to this survey, laparoscopic right colectomy with intracorporeal anastomosis emerged as one of the most difficult laparoscopic surgical procedures. 11 Nevertheless, the dehiscence rate in our study is in line with the 5.2% leak rate recently reported in the largest monocenter study, including 173 ileocolic intracorporeal anastomoses. 23
In the present series, a similar length of stay was observed in the two groups, despite the lower incidence of postoperative ileus and the earlier recovery of bowel function observed in the IA group. This finding could probably be explained on the basis of the two cases of anastomotic leak that occurred in the IA group, which required reoperation in both cases. A definitive answer on this subject will probably be obtained once the study will be completed.
Although the present study was not designed with clinical outcome as primary endpoint, and definitive conclusion on morbidity could not be made because of the small number of patients included in this preliminary analysis, no difference in the overall and infectious complication rates was observed between the two groups. This is in line with the results reported by recent meta-analyses and retrospective and case-matched studies comparing the two surgical techniques.4,13,15,16,23
One claimed advantage of the intracorporeal technique is avoiding anastomotic twisting and ease of closing the mesenterial defect, despite controversial opinions that exist about the need of closing the mesentery.15,19 Recently, it has been shown that closure is associated with an increase in complications such as obstruction and anastomotic dehiscence. 24 We experienced one case of internal hernia that occurred in the EA group in an obese patient in whom a difficult close of mesentery has been intraoperatively recorded. Chang et al. reported one case of torsion of the anastomosis in the EA group. Similarly, Hellan et al. reported two cases of twisting of the mesentery and an anastomotic volvulus. In both these studies, however, the mesentery was left open.10,18 These findings are in favor of the application of intracorporeal anastomosis with systemic closure of the mesenteric defect, in particular in the obese patients.
With respect to short-term oncological variables, no difference was observed in the number of lymph nodes retrieved. This is an expected finding since the surgical technique applied was conceptually identical in the two groups with high ligation of the vessels at the base of the ileocolic mesentery.
In conclusion, our preliminary results suggest that intracorporeal anastomosis in laparoscopic right colectomy could be considered a valuable option in the hands of expert surgeons, with favorable effect on recovery of bowel function and reduced postoperative ileus. Definitive answers on safety and efficacy of IA will be given once the present RCT will be complete.
Footnotes
Acknowledgment
The authors thank Giovanni Radaelli, MB, PhD, from the Department of Biometry and Statistics, University of Milan, Italy, for his statistical assistance.
Disclosure Statement
No competing financial interests exist.