
Abstract
Abstract
Introduction and Objective:
Appendectomy is one of the most common operations carried out by general surgeons. The recent introduction of the alternative energy-based devices in surgery and their use in the laparoscopic appendectomy shortened the duration of operations, but these devices are used generally for meso dissection. These devices did not receive wide acceptance among surgeons as there is not enough evidence confirming their use in appendicular lumen operations. Our objective in this study was to test the safety of three types of appendectomy.
Materials and Methods:
Twenty-four cases with right hemicolectomy or subtotal colectomy were enrolled into this study. The patients were distributed in three groups. After the colectomy specimen was removed, in Group 1 conventional appendectomy (it was dissected with mesoappendiceal fixation and with electro cauterization) was performed in the operating room, the appendicular stump was ligated with a silk suture; in Group 2 appendectomy was performed with LigaSure™ and the stump was closed also with LigaSure; in Group 3 appendectomy was performed with Harmonic Scalpel™ and the stump was closed also with Harmonic Scalpel. Stump opening pressures were measured in all patients in the groups.
Results:
Three groups were compared in terms of age, gender, concomitant diseases, clinical diagnosis, previous operations, pathological findings, and applied maximum pressure levels. No statistical difference was detected among the groups.
Conclusion:
Appendectomies carried out with LigaSure and Harmonic Scalpel are as safe as appendectomies carried out with the conventional methods.
Introduction
A
Materials and Methods
In our study, we enrolled 24 patients, who had right hemicolectomy and subtotal colectomy in the general surgery clinic of Keçiören Training and Research Hospital between July 2010 and January 2013. Connective tissue disorders, colon ischemia, cecum tumor, lesion in the appendicular stump more than 10 cm in size, disseminated infection in the abdomen, and appendectomy were regarded as exclusion criteria. Patients were distributed in three groups using the sealed envelope method. After colectomy specimen was resected, in Group 1 conventional appendectomy (it was dissected with mesoappendiceal fixation and electro cauterization) was performed in the operating room, appendicular stump was ligated with a silk suture; in Group 2 appendectomy was performed with LigaSure™ and stump was closed also with LigaSure (Fig. 1); in Group 3 appendectomy was performed with Harmonic Scalpel™ and stump was closed also with Harmonic Scalpel. After operation, the material in the specimen was discharged, proximal part was examined with palpation, and after being certain that there was no mass, ileum and distal area distant about 10 cm from appendix were closed with clamp. The colon was opened 1 cm next to distal side of the clamp and a 16F Foley catheter was inserted and was fixated with a purse suture (Fig. 2). Afterward, the Foley catheter was connected to a Rister® manual pneumatic komprimeter with a 0–700 mmHg gauge. The pump mechanism of the komprimeter enabled us to inflate the colon manually and its gauge made possible simultaneous monitorization of the intraluminal pressure. A certain pressure level achieved by the inflation process caused ruptures in the haustra and as a consequence sudden and significant drop of pressure was observed. This pressure, if it opened up the stump, was recorded as the “stump opening pressure” and if not opened, the achieved pressure was recorded as the “maximum pressure” (Fig. 3).

Appendectomy by means of LigaSure™.
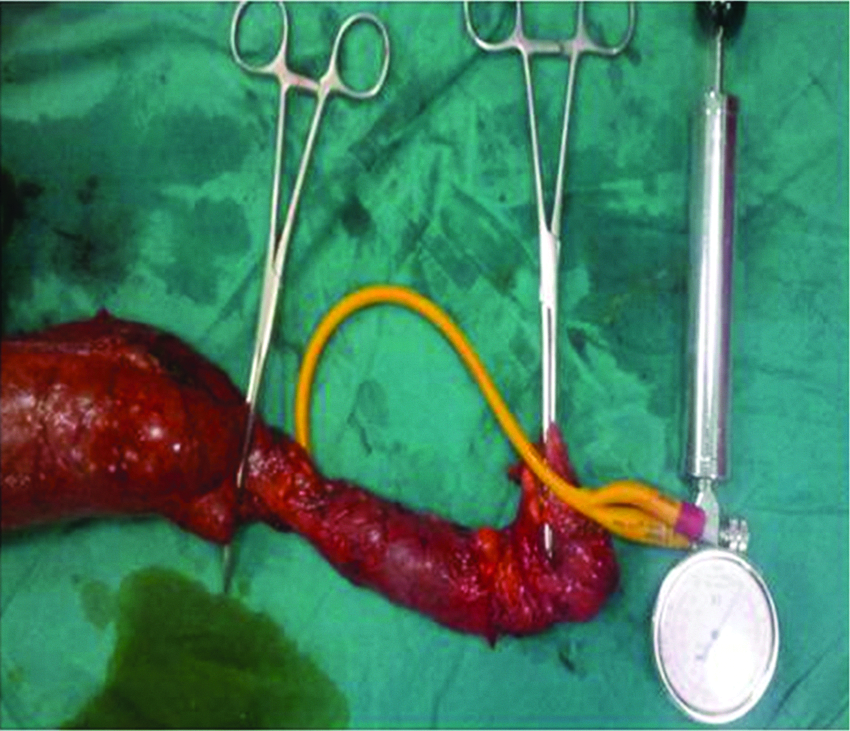
Preparation of colon pressure measurement mechanism.

Inflating colon and following appendix stump.
Continuous variables were recorded as mean ± standard deviation, dispersed variables were as median (minimum–maximum), and categorical variables were recorded as numeric values and percentage. One-way ANOVA and Mann–Whitney U tests were used for comparison of averages. Categorical variables were compared with Pearson's Chi-square test. The duplex statistical significance level was set to P < .5. Analyses were done with Windows SPSS v10.0.
Results
Twenty-four patients (M:F = 1:1) were enrolled into the study. Patients were distributed in three groups using the sealed envelope method. Their average age was 58.7 years (22–87 years). Operation was indicated according to the following diagnoses: colon cancer (10 patients), volvulus (5 patients), colonic intussusception (2 patients), and polyposis coli (6 patients). In patients with volvulus and polyposis coli, subtotal colectomy was performed; in patients with colon tumor and colonic intussusception, right hemicolectomy was performed. Only 2 patients had subtotal colectomy, because the colon structure was destroyed as a result of the extreme dilatation caused by the flexural and transverse colon tumors. Appendiceal stump did not open up in any group until the maximum pressure value. Averages of the maximum pressures were 510.0 ± 6.5 mmHg in Group 1, 495.8 ± 9.2 mmHg in Group 2, and 480.3 ± 8.6 mmHg in Group 3. There was not any statistically significant difference among the groups in terms of the average maximum pressure levels (P = .25). Also we did not found any statistically significant difference regarding gender (P = .8), comorbidity (P = .56), clinical diagnosis (P = .2), operation type (P = .39), and pathological diagnosis (P = .34) among Groups 1, 2, and 3.
Discussion
In our study, we demonstrated that after the appendectomy performed with three different methods, stump did not open under given pressures and these methods were equally safe. In operations, different energy-based devices were used generally for the ligation of the vessels. It was demonstrated that instruments can be safely used in both ligation and cystic duct closure in the cholecystectomy operations. Experimental studies showed that the duct closed with these devices could also resist high pressures such as 320 mmHg. Reports about the safe usage of these devices in cholecystectomy encouraged surgeons to use these devices also in the lumen closure operations. 7
The appendectomy operation technique without clip and nodule described by Khanna et al. is an important progress in the laparoscopic appendectomy technique. 4 However, there is no other study confirming the results of Khanna, who closed safely the appendicular lumen with bipolar electrocoagulation in 60 patients. Needless to say, for the demonstration of the safety of the closure of the appendicular lumen without clip and nodule only with energy sources, randomized and prospective clinical studies with big patient groups are necessary.
In this topic, as the clinical experience is not sufficient, experimental studies gain in importance. However, it is difficult to conduct studies on this topic, as studies on chimpanzees that have an appendicular structure most similar to humans, have practical hindrances and other animals have quite different appendicular structures. 8 In the study of Aslan et al., the cecum resection was done with silk suture ligation or bipolar electrocoagulation. Although the stump's opening pressure just after the cauterization was 11.2 ± 2.7 cmH2O, no opening in the resection line even under pressures up to 30 cmH2O was observed after 15 days in both suture and bipolar cauterization groups. 6
Burkit and Donovan, in their study, monitored the pressure inside the colon in patients with left colon resection. They observed that 98% of the pressures measured in the first 89 hours were around 50 mmHg and the maximum pressure was 90 mmHg. 9 Roeder et al., in their study, showed that grafts, obtained from mucosa of the small intestine, can resist high pressures up to 3500 mmHg. 10 Although, under the normal physiological conditions, intraluminal pressure may be up to 90 mmHg in humans, low pressures such as 30 cmH2O may be not considered as reliable by the surgeons. However, these findings are still important, as operations are influenced not only by mechanic impacts but also by physiological impacts.
However, during the application of high pressures (500 mmHg) on the colon segments, we did not observe any mucosal or submucosal injury in the related colon segments. As colon segments are destroyed as a result of ruptures in haustra caused by the applied pressure, a pressure of 500 mmHg was applied as the maximum pressure, so that it did not prevent the pathological examination. In our study, as we tested the lumen closures performed with different techniques, with high pressures such as 500 mmHg, regarding the early-phase safety of these techniques our findings might be useful for surgeons.
In our study, three techniques were used in the right colon tissue, which was removed because of different pathological diagnoses before the operation, and pressures that force the stump to open were evaluated. Although we have concerns about having performed these three methods on the normal appendicular vermiformis, we still believe that similar results would be obtained in patients with acute appendicitis and a normal stump.
Another weakness of our study is that we evaluated stump pressures immediately after surgery. These may not reflect the stump pressures of the inflamed appendix a few days later, if opening or leakage is likely to occur. However, our model is the most appropriate model to evaluate the appendix stump pressure up until today. It may be useful to design studies focusing on the early- and late-phase comparison of different closure techniques concerning acute appendicitis models in animals with a cecum and appendix structure similar to humans. The efficacy of the devices may be investigated with a stump opening pressure measured with the relaparatomy performed after a certain waiting period in edematous and inflamed stumps. Thus, instead of the mechanical factors, the physiological factors will be investigated.
In conclusion, appendectomies carried out with LigaSure and Harmonic Scalpel are as safe as appendectomies carried out with conventional methods.
Footnotes
Disclosure Statement
We hereby declare that all authors have made a substantial contribution to the information submitted for publication, all have read and approved the final article, and the study was not published or accepted by a journal or not under consideration for publication. We have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers' bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this article.