
Abstract
Abstract
Background:
Laparoscopic pancreatic surgery has gradually expanded to include pancreatoduodenectomy (PD). This study presents data regarding the efficacy of laparoscopic PD in a single center.
Methods:
This was a single-cohort, prospective observational study. From March 2012 to September 2015, 50 consecutive patients underwent laparoscopic PD using a five-trocar technique. Reconstruction of the digestive tract was performed with double jejunal loop technique whenever feasible. Patients with radiological signs of portal vein invasion were operated by open approach.
Results:
Twenty-seven women and 23 men with a median age of 63 years (range 23–76) underwent laparoscopic PD. Five patients underwent total pancreatectomy. All, but 1 patient (previous bariatric operation), underwent pylorus-preserving resection. Reconstruction was performed with double jejunal loop in all cases except in 5 cases of total pancreatectomy. Conversion was required in 3 patients (6%) as a result of difficult dissection (two cases) and unsuspected portal vein invasion (1 patient). Median operative time was 420 minutes (range 360–660), and the 90-day mortality was nil. Pancreatic fistula occurred in 13 patients (26%). There was one grade C (reoperated), one grade B (percutaneous drainage), and all remaining were grade A (conservative treatment). Other complications included port site bleeding (n = 1), biliary fistula (n = 2), and delayed gastric emptying (n = 2). Mean hospital stay was 8.4 days (range 5–31).
Conclusions:
Laparoscopic PD is feasible and safe, but is technically demanding and may be reserved to highly skilled laparoscopic surgeons with proper training in high-volume centers. Isolated pancreatic anastomosis may be useful to decrease the severity of postoperative pancreatic fistulas. Therefore, it could be a good option in patients with a high risk for developing postoperative pancreatic, as well as by less-experienced surgeons.
Introduction
P
The first laparoscopic PD was performed by Gagner and Pomp in 1992. 5 Since then, the difficulty of the procedure has resulted in relatively few laparoscopic PD cases. However there is a recent interest in this type of surgery and the number of procedures is rapidly increasing.4,6 This aim of this article is to report our experience with laparoscopic PD.
Materials and Methods
This was a single-cohort, prospective observational study. From March 2012 to September 2015, 50 consecutive patients underwent laparoscopic PD using a five-trocar technique in a single center. Reconstruction of the digestive tract was performed with the double jejunal loop technique 7 except in cases when total pancreatectomy was required. Patients with suspicion of portal vein invasion by preoperative imaging were treated with an open approach. Patients with borderline resectable disease, patients operated on after neoadjuvant treatment, and those refusing laparoscopy were treated with the open approach. Over this period, 47 patients underwent open PD. The patients were informed about the advantages and risks of the technique, and they gave informed consent.
Surgical technique
The patient is placed in a supine position with the surgeon standing between the patient's legs. Five trocars are used (Fig. 1). Using an open technique, a 10-mm trocar is placed above the umbilicus and a 10-mm 30-degree angled laparoscope is introduced through this port. Pneumoperitoneum is established at a pressure of 12 mmHg. Once examination of the abdominal cavity confirms the absence of peritoneal metastases, four additional trocars are inserted. One 12-mm trocar is placed on the left midclavicular line about 5-cm above the umbilicus for the surgeon's right-hand. A 5-mm port is placed in a subxiphoid position and it is used for retraction. A 5-mm port is placed on right midclavicular line about 5-cm above the umbilicus for the surgeon's left hand. Finally a 5-mm port is placed on right axillar line for retraction.
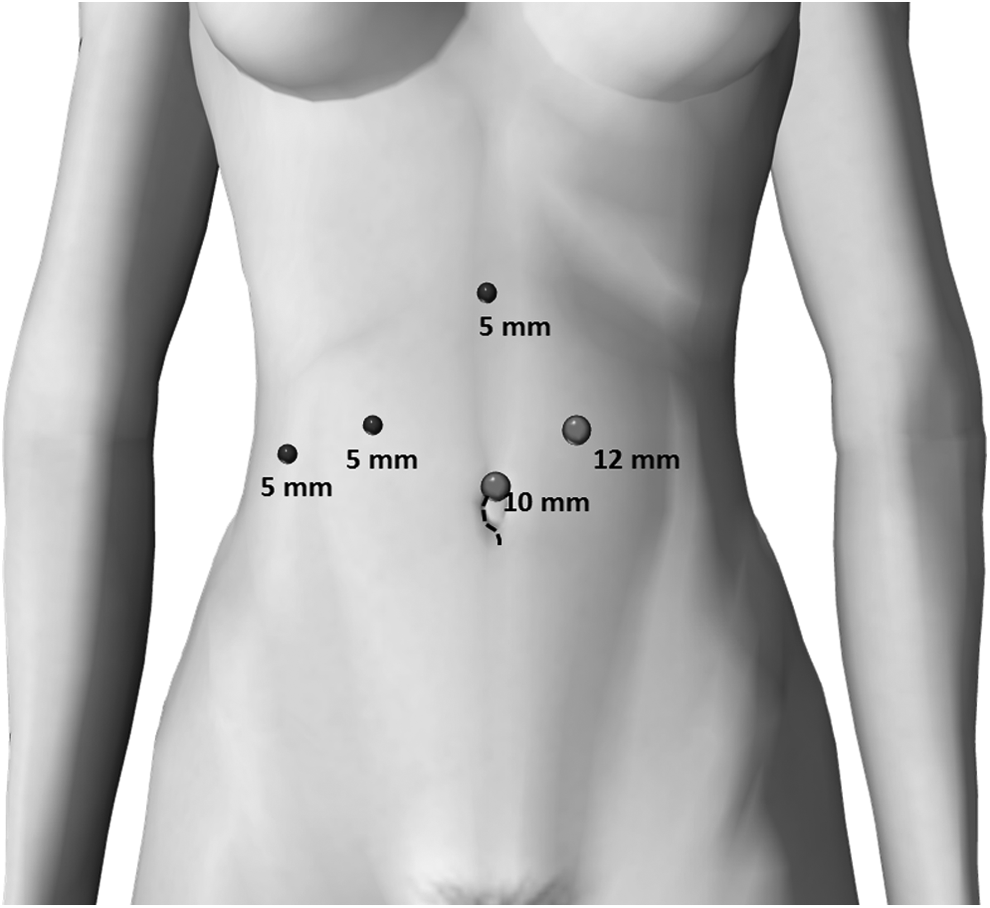
Trocar placement. Five trocars are used as displayed, including three 5-mm trocars, one 10-mm, and one 12-mm trocar. The surgical specimen is retrieved through the umbilical incision and in some cases with larger tumors, an enlargement of this incision is necessary (interrupted dots).
Pylorus-preserving PD
The Kocher maneuver is performed with upper traction of the duodenum. After division of the gastroepiploic vessels, the duodenum is transected 2–4 cm below the pylorus using an endoscopic linear stapler. The stomach is then moved to the left upper quadrant followed by hepatic hilum dissection. Cholecystectomy is performed, and the common bile duct is dissected and divided. The proximal bile duct is maintained closed with a detachable vascular clamp, and the hepatoduodenal ligament is then skeletonized. The gastroduodenal artery is safely divided, and the portal vein is exposed. A tunnel is carefully created behind the neck of the pancreas at the level of superior mesenteric and portal vein using a right angle instrument and blunt dissection. The pancreas is then divided with a harmonic scalpel.
Reconstruction of the alimentary tract with double jejunal loop
Reconstruction of the alimentary tract was performed using a double jejunal loop technique. 7 First, double-layered end-to-side pancreaticojejunostomy with duct-to-mucosa anastomosis was performed followed by a second layer between the jejunal seromuscular and pancreatic tissue to reinforce the anastomosis. Second, the jejunal loop is divided with stapler and side-to-side jejunojejunostomy is performed with stapler leaving a 40-cm jejunal loop for hepaticojejunostomy. Next, a detachable vascular clamp is removed and an end-to-side hepaticojejunostomy is performed with running absorbable suture. Finally, end-to-side duodenojejunal anastomosis is performed using the standard double-layer technique in an antecolic manner (Fig. 2). Two drains—one for pancreaticojejunostomy and the other for hepaticojejunostomy—are left in place and exteriorized on the left and right flank, respectively.

Schematic drawing of double jejunal loop technique for reconstruction of the alimentary tract after laparoscopic pylorus-preserving pancreatoduodenectomy.
Variables
The primary endpoint was safety of the procedures. Safety was assessed as the occurrence of complications during hospitalization such as pancreatic fistulas, delayed gastric emptying, and postpancreatectomy hemorrhage. Ninety-day mortality was additionally assessed. To further account for the severity of complications, the Clavien–Dindo classification was used. 8 Secondary outcomes were surgical efficacy endpoints such as conversion rate, operative time, blood loss, need for transfusions, and length of hospitalization.
Pancreatic fistula was diagnosed (measurable drain output on or after postoperative day 3 with an amylase content thrice the upper limit of the normal serum value) and classified according to International Study Group on Pancreatic Fistula Definition. 9 Delayed gastric emptying was defined as the inability to return to a standard diet by the end of the first postoperative week (includes prolonged nasogastric intubation) and classified according to the International Study Group of Pancreatic Surgery (ISGPS). 10 Postpancreatectomy hemorrhage was graded according to the ISGPS consensus definition. 11
Statistical analysis
Values are expressed as means and ranges or percentages when appropriate. The chi-square test was used to compare categorical variables. The independent t-test and the Mann–Whitney test were used to compare continuous variables. Values of P < .05 were considered significant. All statistical studies were performed using SPSS version 19.0 (SPSS, Inc.).
Results
We have performed this procedure on 50 consecutive cases. Twenty-seven women and 23 men with median age of 63 years (range: 23–76) underwent laparoscopic PD (Table 1). Twenty-two patients were treated for ductal adenocarcinoma, 11 for neuroendocrine tumor, 8 for intraductal papillary mucinous neoplasm (IPMN), 3 for periampullary adenocarcinoma, and 6 for other causes (Table 2).
IPMN, intraductal papillary mucinous neoplasms.
Five patients underwent total pancreatectomy. Three patients had type 1 diffuse IPMN, 1 patient with multiple neuroendocrine tumors (NEM 1), and 1 patient with multiple pancreatic metastasis from kidney tumor.
All, but 1 patient (previous bariatric operation), underwent pylorus-preserving resection. Reconstruction was performed with a double jejunal loop in all cases except in 5 cases of total pancreatectomy. Hand assistance was used in 2 cases in the beginning of our experience. 7 Operative variables are depicted in Table 3. Conversion was required in 3 patients (6%) as a result of difficult dissection (two cases) or unsuspected portal vein invasion (1 patient). Median operative time was 420 minutes (range 360–660); the 90-day mortality was nil. Pancreatic fistula (excluding 5 patients with total pancreatectomy) occurred in 13 patients (29%). One patient developed a grade C fistula and abdominal sepsis that required reoperation by an open approach after failed percutaneous drainage. This patient fully recovered. Another patient developed persistent abdominal collection and was successfully treated by percutaneous drainage (grade B). The remaining patients with pancreatic fistula presented grade A and recovered with conservative treatment, that is, late removal of the abdominal drain. Two patients developed delayed gastric emptying—both were grade B. One patient developed postpancreatic hemorrhage (grade B) with full recovery. Other complications included port site bleeding (n = 1) and biliary fistula (n = 2). Mean hospital stay was 8.4 days (range: 5–31). Late complications were umbilical hernia and biliary stenosis that required reoperation after failed percutaneous biliary manipulation. One patient required correction of umbilical hernia and another underwent successful laparoscopic de novo hepaticojejunostomy.
Comparison of two consecutive periods (learning curve)
The first 20 laparoscopic PD were compared to the last 30 cases. Table 4 shows a significant decrease in the operation time (465 versus 405 minutes, P < .001) and blood loss (295 versus 188 mL, P = .004). There was no difference in morbidity, including severe pancreatic fistula, reoperation, or bleeding between the two groups. Conversion to an open approach and other complications such as wound infection, delayed gastric emptying, and bile leaks were also similar between the two groups. Late complications such as umbilical hernia and biliary stenosis occurred in the first 20 cases, but were not statistically significant.
Five total pancreatectomies were excluded, 4 in the first 20 cases and 1 in the latter period.
Patients with ductal adenocarcinoma.
When we analyzed patients undergoing laparoscopic PD due to ductal adenocarcinoma, there were no differences in the number of patients in both groups and no differences in R0 resection. However, the number of harvested lymph nodes was higher in the last period (P = .049) (Table 4).
Discussion
The data are from a high-volume institution with highly experienced pancreatic surgeons. The initial comparative data suggest that minimally invasive PD are feasible with outcomes that are comparable to an open approach for a select group of patients.5,12–14
Our experience with minimally invasive pancreatic resections began in 2001. 15 Our first pancreatic laparoscopic procedure was a distal pancreatectomy for a benign cystic tumor. Our expertise improved and we integrated new equipment and technology to facilitate more complex operations. Laparoscopic procedures such as resection of uncinate process, central pancreatectomy with Roux-en-Y pancreatojejunostomy, and major liver resections with hepaticojejunostomy were subsequently added to our surgical armamentarium.16–18 Therefore, most of the necessary skills to perform a laparoscopic PD were progressively acquired. This prompt us to start a protocol for gradual implementation of this procedure based on the initial favorable results from Palanivelu's group. 12 These benefits over the open approach were later confirmed by Asbun and Stauffer. 13
More recently, a larger comparative study from the Mayo Clinic showed not only shorter hospital stay and faster recovery but also a longer progression-free survival in patients undergoing laparoscopic PD than those undergoing open surgery. 14 This result boosted the number of minimally invasive PD performed in the United States. 4 A recent study analyzed the short-term outcomes from minimally invasive PD to operation for adenocarcinoma at a population level and showed an increased 30-day mortality. 4 Another important finding is that the majority of hospitals performing minimally invasive PD were low volume. It is common knowledge that both hospital volume and surgeon experience are significantly associated with reduced morbidity and mortality after PD. 19 Therefore, some sort of concentration of selected operations in high-volume hospitals are highly warranted. 20
Abdelgadir et al. 4 suggested that comprehensive protocols are necessary and rigid criteria should be met for implementation of minimally invasive PD to optimize patient safety. While there is a competitive desire among surgeons and institutions to implement new minimally invasive techniques and improve patient outcomes, premature introduction of new techniques could impair patient outcomes and ultimately the success of the procedure. 4 It is likely that such a phenomenon is happening in other countries as well. In our service, we only started a program of laparoscopic PD in 2012 after extensive experience in both open and laparoscopic pancreatic procedures with increasing complexity. 15 This is directly reflected in our results with the absence of postoperative 90-day mortality and acceptable rate of complications.
Pancreatic fistulas from pancreatic anastomosis are the most common factors responsible for the high morbidity and mortality after both open and laparoscopic PD.1,2,6 To reduce the incidence and complications of anastomosis, several techniques, including pancreaticogastrostomy, duct to mucosa anastomosis, binding pancreaticojejunostomy, or the use of octreotide, have been studied. However, none of these have shown a clear advantage.21–23
Most of the reports related to pancreatic fistula use a technique to decrease the incidence and not to the severity of this complication. Pancreatic juice is secreted in an inactivated state and is activated into the bowel lumen mainly by biliary secretion. In all of our patients except those undergoing total pancreatectomy, the double jejunal loop technique was used.7,24 Separation of the biliary and pancreatic conduits may decrease the incidence and the severity of pancreatic fistulas, therefore reducing the morbidity and mortality of PD.7,24,25 This may be of special interest when one expects a higher rate of pancreatic fistula such as in patients with periampullary tumors. 26
In conclusion, laparoscopic PD is feasible and safe, but is technically demanding and may be reserved for highly skilled laparoscopic surgeons with proper training in high-volume centers. Isolated pancreatic drainage may be useful in decreasing the severity of postoperative pancreatic fistulas. Therefore, it could be a good option in patients with high risk for developing a postoperative pancreatic fistula, as well as with less-experienced surgeons.
Footnotes
Disclosure Statement
No competing financial interests exist.