
Abstract
Abstract
Background:
Laparoscopic right hepatectomy (LRH) is increasingly performed for the treatment of many liver diseases. However, it remains a challenging procedure and is limited to highly specialized centers. Increasing the safety and efficacy of LRH is crucial. This study evaluated the safety and feasibility of the novel caudal approach (CDA) in LRH and in comparison with the conventional approach (CA).
Methods:
Of a total of 40 patients who underwent LRH between June 2007 and July 2015 at our center, 10 cases underwent the CDA, while 30 underwent the CA. Operative and postoperative outcomes were analyzed.
Results:
Clinical data and patient characteristics were comparable between the two groups. Only 1 patient required a laparoscopic-assisted procedure in the CDA group, while 14 patients were converted to laparotomy (n = 10) or laparoscopic-assisted procedures (n = 4) in the CA group, although the difference did not reach statistical significance (P = .060). However, the difference in conversion to laparotomy between the two groups was significant (P = .043). In addition, when considering 23 patients with malignancies, the median surgical margin was significantly greater in the CDA group (n = 6) (20 mm versus 10 mm; P = .023) than in the CA group (n = 17). Other operative and postoperative outcomes were similar between the two groups.
Conclusions:
The CDA achieves safety and feasibility similar to that of the CA in LRH and requires relatively less conversion to laparotomy. In selected patients, the CDA offers an alternative option to the CA for LRH in experienced hands. Further studies with larger samples are warranted to evaluate the CDA.
Introduction
L
In open right hepatectomy, the anterior approach is frequently used, which contributes to reducing blood loss and holds oncologic benefits for tumor patients by avoiding previous mobilization of the right liver before liver parenchymal transection.23–26 Recently, a similar technique in laparoscopic liver resection, known as the caudal approach (CDA), has been seriously proposed by Soubrane et al. 27 and has gained expert consensus. 28 The CDA is based on the anterior approach described by Liu et al. 24 in open liver resections and also emphasizes that liver parenchymal transection should be performed before liver mobilization. Soubrane's report 27 indicates that the CDA confers low blood loss and morbidity in LRH. Therefore, the CDA is a potential alternative to the anterior approach in open right hepatectomy. 28
Our previously extensive experience in laparoscopic liver resections2,29,30 and encouraging literature results of the anterior approach in open right hepatectomy23–26 have led us to focus on the CDA in LRH. To our knowledge, few studies27,31–34 have mentioned the anterior approach or the novel CDA in LRH or other major laparoscopic liver resections. In this series, we report our preliminary operative and postoperative findings on the safety and feasibility of the CDA compared with the conventional approach (CA) in LRH.
Methods
Patients and data collection
From June 2007 to July 2015, 40 patients who underwent LRH at our center (Department of General Surgery, Institute of Minimally Invasive Surgery, Sir Run Run Shaw Hospital, College of Medicine, Zhejiang University, Hangzhou, China) were enrolled in this study. Right hepatectomy was defined as the resection of four Couinaud segments, including segments V–VIII. All patients with benign or malignant liver diseases were evaluated by preoperative laboratory tests and computed tomography scan (Fig. 1A). Eighteen patients had hepatocellular carcinoma (HCC) (45%), 12 intrahepatic lithiasis, 5 hemangioma, 3 colorectal liver metastases, and 2 intrahepatic cholangiocarcinoma. Three major surgeons participated in this study. Whether using the CDA or CA in LRH depended on the surgical extent, tumor size and location, and organ involvement, as well as the surgeon's preference. Operative data and postoperative outcomes were recorded and studied. This study was approved by the Institutional Review Board of the Sir Run Run Shaw Hospital.
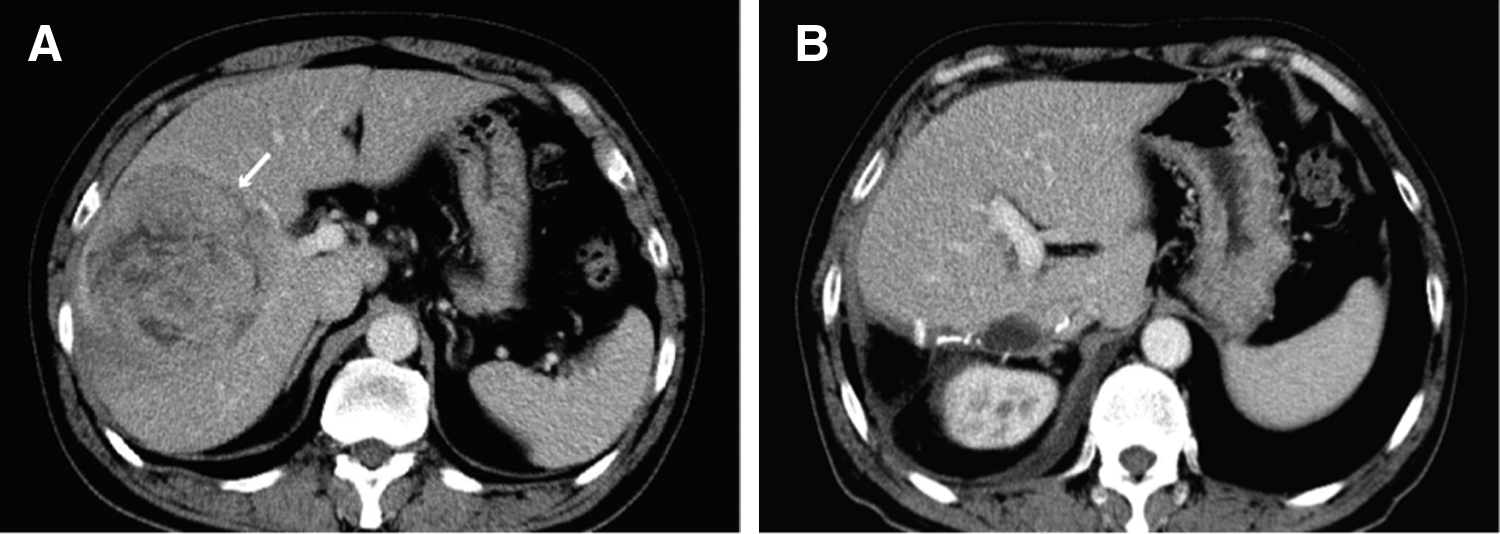
Preoperative and postoperative computed tomography (CT) scan performance of a 58-year-old male with a large hepatocellular carcinoma lesion.
Operative techniques
All patients were placed in the supine position. Basic laparoscopic equipment included trocars, a 30° laparoscope, the laparoscopic multifuctional operative dissector (LPMOD),29,35 the Goldfinger dissector (Blunt Dissectors, Obtech Medical, Johnson & Johnson, Le Locle, Switzerland), and other requisite instruments. Five to six trocars were generally used. A pneumoperitoneum was established in all procedures. After surgical exploration, both groups first underwent cholecystectomy but with the gallbladder remaining in situ.
For patients who underwent the CA, the right liver was mobilized completely from the retroperitoneum and rotated anteriorly to expose the retrohepatic inferior vena cava (IVC). The short venous branches were individually ligated, and then, the right hepatic vein (RHV) was divided and ligated extrahepatically. Liver hilar dissection was undertaken to acquire control of the right hepatic artery and portal vein. We then applied the LPMOD along with the technique of curettage and aspiration29,35 to transect the liver parenchyma along the demarcation line (Fig. 2B). However, if the RHV could not be previously dissected, an intrahepatic approach would substitute for the RHV ligation at the end of the liver transection using an Endo-GIA stapler. Generally, the right hepatic duct was not divided and ligated by clips or silk suture until the early phase of liver transection, when Glisson's capsule was detached in case of injury to the hepatic portal bile duct.
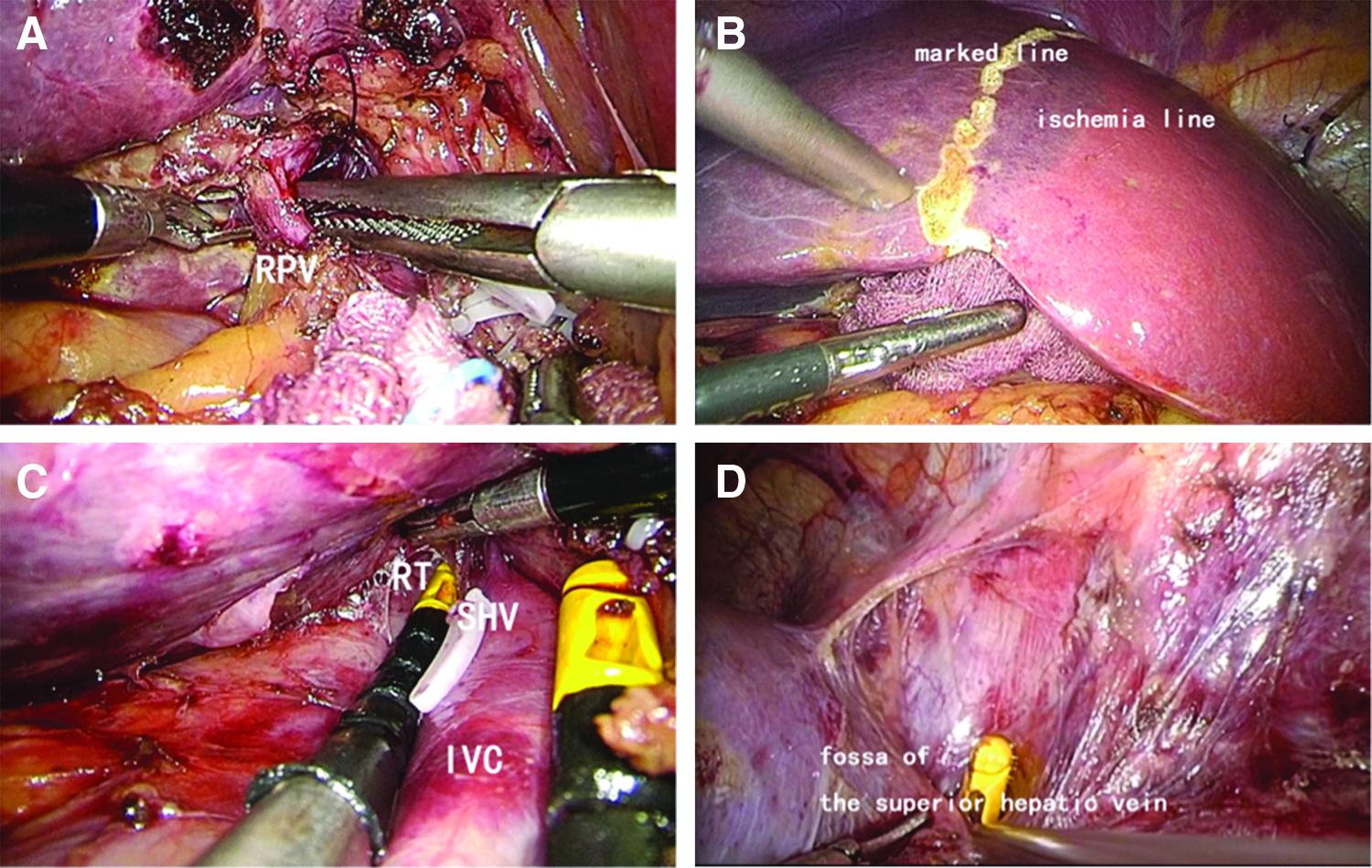
Liver hilar dissection and establishment of the retrohepatic tunnel.
For patients who underwent the CDA, dissection of the right portal pedicle was first carried out (Fig. 2A). In fact, the CDA we used here was similar to the original four-step strategy in Soubrane's study, 27 and we extended this approach by establishing a retrohepatic tunnel between step 1 (liver hilar dissection intrafascially) and step 2 (liver parenchymal transection). Next, the retrohepatic space anterior to the IVC was meticulously dissected using the Goldfinger dissector (Fig. 2C, D). The caudal half of the retrohepatic tunnel was gradually established by dissection from the caudate lobe in a caudal to cranial direction along the avascular space anterior to the IVC. The cranial half of the retrohepatic tunnel was achieved by dissection from the fossa of the superior hepatic vein, locating between the RHV and the middle hepatic vein, in a cranial to caudal direction along the avascular space anterior to the IVC. The retrohepatic tunnel was then completely (when the two halves were connected) or partially established depending on the surgeon's proficiency and the technical difficulty in each case. Specifically, in our last five cases, a complete retrohepatic tunnel was established and the liver-hanging maneuver 36 was used to elevate the liver. The transection was then performed by LPMOD in a caudal to cranial direction (Fig. 3A) until the IVC was clearly exposed. The right hepatic duct was divided and ligated during this transection phase when it was clearly identified. Each branch of short hepatic veins was ligated individually, and the RHV was dissected free and ligated by silk suture or an Endo-GIA stapler (Fig. 3B). The right liver was soon mobilized out of the retroperitoneum (Fig. 3C) after the right triangular ligament was divided, after which the specimen was placed in a plastic bag and removed through a remote suprapubic incision. Finally, a careful examination was made for hemostasis and bile leaks (Fig. 3D).
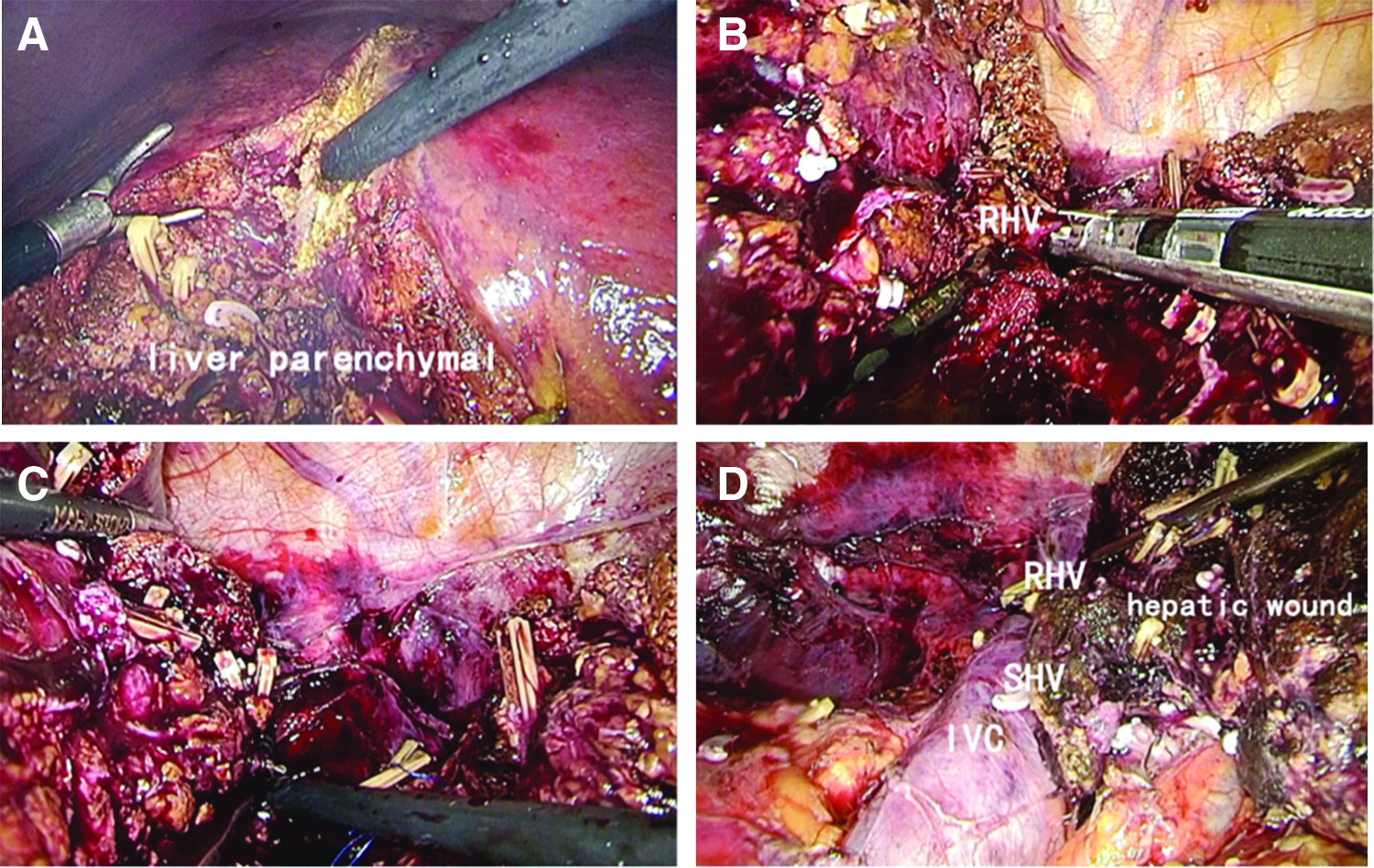
Parenchymal transection by the caudal approach and mobilization of the right liver.
Statistical analysis
Operative and postoperative parameters included operating time, intraoperative blood loss, red blood cell transfusion rate, conversion rate, malignancy characteristics, overall complication rate, postoperative alanine aminotransferase (ALT) peak level, total bilirubin peak level, international normalized ratio (INR) peak level, recovery time, postoperative death, readmission rate, and length of postoperative hospital stay. Continuous data were expressed as medians (with ranges). The Mann–Whitney U test was used to compare differences of the continuous data between two groups. Fisher's exact test was used for proportions. All clinical data were entered and analyzed using SPSS version 19.0 (SPSS, Inc., Chicago, IL), and a P < .05 was considered statistically significant.
Results
Clinical data and patient characteristics
The clinical data and patient characteristics between the two groups showed no significant difference in demographics (age and sex), indications for surgery, Eastern Cooperative Oncology Group performance status, body mass index, American Society of Anesthesiologists status, presence of hepatitis B surface antigen or cirrhosis, history of upper abdominal surgery, presence of hypertension or diabetes mellitus, and laboratory tests (Table 1).
By Mann–Whitney U test.
By Fisher's exact test.
LRH CDA, laparoscopic right hepatectomy by the caudal approach; LRH CA, laparoscopic right hepatectomy by the conventional approach; HCC, hepatocellular carcinoma; CLM, colorectal liver metastases; ECOG, Eastern Cooperative Oncology Group; BMI, body mass index; ASA, American Society of Anesthesiologists; HBsAg, hepatitis B surface antigen; ALT, alanine aminotransferase; AST, aspartate aminotransferase; PT, prothrombin time; INR, international normalized ratio.
Operative data
The median operating time, intraoperative blood loss, and red blood cell transfusion rates were comparable between groups (P = .790, P = .605, and P = 1, respectively). In our last five cases, a complete retrohepatic tunnel was established and the hanging maneuver was adopted totally laparoscopically. Although the total conversion rates (including laparotomy and laparoscopic-assisted procedures) were comparable between the two groups (10% versus 46.7%, P = .060), none of these patients in the CDA group required conversion to laparotomy, compared with 10 (33.3%) in the CA group (P = .043). Reasons for conversions among all patients included tight adhesions, uncontrollable intraoperative bleeding, and poor exposure under laparoscopy. Among 23 patients with malignant tumors in the two groups, there was no significant difference in the maximum diameter or the number of lesions. All of them received R0 resection; the median surgical margin was significantly greater in the CDA group (n = 6) (20 [10–40] mm) than in the CA group (n = 17) (10 [10–25] mm; P = .023) (Table 2).
By Mann–Whitney U test.
By Fisher's exact test.
P < .05 indicates significant difference.
This comparison was drawn based on 23 patients with malignant tumors, including hepatocellular carcinoma (n = 18), colorectal liver metastases (n = 3), and intrahepatic cholangiocarcinoma (n = 2) between the CDA group (n = 6) and the CA group (n = 17).
LRH CDA, laparoscopic right hepatectomy by the caudal approach; LRH CA, laparoscopic right hepatectomy by the conventional approach; RBC, red blood cell.
Postoperative outcomes
The overall complication rates were comparable between the two groups (P = .700). According to the Clavien–Dindo classification, 37 most complications were not severe (≤Grade IIIa). In the CDA group, there was one severe complication when a male patient developed postoperative renal dysfunction (Grade IVa), but he received dialysis and support therapy immediately and recovered within 2 weeks postoperatively. In the CDA and CA groups, respectively, the median postoperative ALT peak level was 400 IU/L and 351.5 IU/L (P = .950); median postoperative total bilirubin peak level, 45.1 μmol/L and 42.4 μmol/L (P = .747); and median postoperative INR peak level, 1.525 and 1.395 (P = .272). No significant difference was observed in recovery time between the two groups. The median length of postoperative hospital stay was comparable between the two groups, at 14.5 (range, 9–25) days in the CDA group and 13.0 (range, 7–33) days in the CA group (P = .814). Readmission rates were also comparable (20% versus 16.6%; P = 1). No deaths had occurred in either group at 90 days postoperatively (Table 3).
Complications are graded according to Clavien–Dindo classification; ALT, alanine aminotransferase; INR, international normalized ratio.
By Fisher's exact test.
By Mann–Whitney U test.
LRH CDA, laparoscopic right hepatectomy by the caudal approach; LRH CA, laparoscopic right hepatectomy by the conventional approach.
Discussion
Laparoscopic liver resection has prevailed among surgeons, with satisfactory outcomes widely reported.3–5 LRH has also been established in treating liver diseases and has gained popularity in recent years.3,14–20 However, according to the Morioka statement, 28 LRH, together with other major laparoscopic liver resections, remains an innovative procedure in the exploration phase. Moreover, LRH is regarded as very challenging, owing to its apparent technical difficulty in resecting the largest and deepest part of the liver and its potentially hazardous complications, including massive bleeding. Increasing the safety and efficacy of LRH to induce more benefits for patients therefore appears crucial. For patients with huge tumors who undergo right hepatectomy, inappropriate mobilization of the liver may result in massive intraoperative bleeding caused by the rupture of tumors. Moreover, dissemination of tumor cells into the systemic circulation is a concern. While the anterior approach in open right hepatectomy has been widely used and has proved advantageous in ruling out such concerns for patients with huge tumors,23–26 laparoscopic procedures are associated with some inevitable defects, including loss of tactile feedback.
The major advantage of the CDA over other techniques in LRH is the possibility of preventing injuries to the major vascular structures and obtaining oncologic benefits for tumor patients. The CDA is based on oncologic principles, including abandonment of previous mobilization of the liver. Reports on the CDA in LRH are ongoing in the current literature. The initial study by Soubrane et al. 27 reported 30 cases of LRH by the CDA and showed that it was safe and feasible, conferring low blood loss and morbidity. Another report on the CDA in LRH focused on the technical details and demonstrated that this technique could facilitate the safe and efficient execution of the procedure. 34 In our study, we compared 10 patients who underwent LRH by the CDA with 30 patients under the CA. Our results suggest that the CDA for LRH is technically safe and feasible, with operative and postoperative outcomes comparable to those of the CA. To the best of our knowledge, this is the first report comparing the CDA with the CA in LRH.
Our study demonstrated a trend toward a lower total conversion rate in the CDA group than in the CA group, although the difference did not reach statistical significance (P = .060). However, conversions to laparotomy were more in demand in the CA group (P = .043). The only conversion in the CDA group (a laparoscopic-assisted procedure in a patient with intrahepatic lithiasis) occurred at the end of the procedure just before the final right liver mobilization, caused by the existence of tight adhesions owing to previous chronic cholangitis. In this case, a 7-cm small subcostal incision was made to accomplish the right liver mobilization and concomitant removal of the specimen. In addition, the CDA seemed to allow more right hepatectomies to be performed totally laparoscopically. Moreover, bleeding was considered among the most common reasons for conversion.38,39 Dagher et al. 15 reported 20 cases of LRH, 2 (10%) of which required conversion to laparotomy, including one case of continuous diffuse bleeding during parenchymal transection. Lainas et al. 20 performed LRH to treat colorectal liver metastases and reported that 5 (11.1%) out of 45 patients required conversion to open surgery owing to intraoperative bleeding (>900 mL), also during parenchymal transection.
As a consequence, the CDA presents several advantages to help avoid bleeding and improve operative tolerance during parenchymal transection. First, the CDA creates a caudal to cranial operative field, 32 which contributes to better visualization of the dorsal side of the liver and the IVC and RHV, thus avoiding unnecessary injuries to these major vascular structures and reducing the possibility of unnecessary bleeding and conversions. Ogiso et al. 34 described this direction of parenchymal division as “opening a door,” compared with “opening a book” in open liver resections. Ikeda et al. 40 even suggested that a semiprone position could allow better transection for liver parenchyma through the caudal to cranial direction facilitated by the weight of the right liver. Second, the CDA has a distinct advantage in that it requires an upward direction in parenchymal transection, 27 which allows surgeons to be more adaptable when they are habitually looking upward intraoperatively. Furthermore, the CDA is also regarded as a “no-touch” technique with primary vascular control and without tumor manipulation. 27
In addition, the fully established retrohepatic tunnel and liver-hanging maneuver used in five cases in our study can facilitate the CDA and parenchymal transection. When using the liver-hanging maneuver, the hanging tape that passes through the retrohepatic tunnel not only guides the transection plane but also elevates the liver, thus preventing the IVC or its short venous branches from being torn incautiously. In fact, the liver-hanging maneuver, first described by Belghiti et al., 36 was commonly thought to facilitate the anterior approach to acquire better vascular control and improve operative outcomes of liver resections.25,41,42 In cases with the retrohepatic tunnel only partially established (5 patients in our study), the Goldfinger dissector can be inserted through the avascular area anterior to the IVC when the partial liver parenchyma is transected to provide elevating and protective effects, consistent with the previous report by Troisi and Montalti. 43 Moreover, the Goldfinger dissector contributes to the safe establishment of the retrohepatic tunnel and is widely used in LRH 43 because it is atraumatic with an angled shape and has strong consistency to support the liver.
Although recent studies have also showed that large malignant tumors (≥5 cm) can be treated safely by laparoscopic liver resection,44,45 few studies 46 have mentioned resection of even larger malignant tumors (≥10 cm) under total laparoscopy. Interestingly, large tumors previously considered unsuitable for laparoscopy 3 owing to the possibility of tumor break up during mobilization now seem to be quite suitable for the CDA, which avoids previous mobilization. As expected, total LRH by the CDA was performed successfully for two patients with large HCCs (tumor size 11 and 15 cm; data not shown). By contrast, in the CA group, all three patients with large HCCs required conversions (tumor size 10.5, 12, and 16 cm; data not shown). In fact, patients who have huge tumors located in the right lobe of liver, or tumors with infiltration to the diaphragm or the IVC, are more suitable for the CDA than the CA because in the CA, inappropriate mobilization can readily result in massive bleeding and tumor cell dissemination. 24 Tomishige et al. 32 performed laparoscopic posterior sectionectomy using the CDA successfully to resect a 1.5-cm metastatic lesion in segment 6 near the RHV. They concluded that the CDA is useful for patients who have tumors close to the RHV and that exposure of the RHV is necessary.
Our study has also shown that, among patients with malignancies, a greater median surgical margin was observed in the CDA group (P = .023). In fact, whether a wider surgical margin for malignancies is beneficial remains controversial. It was reported47,48 that a wider surgical margin was associated with an increased recurrence-free survival for patients with HCC. However, other studies showed that margin status might have no significant influence on survival among patients with HCC49,50 or colorectal liver metastases. 51 Interestingly, Sasaki et al. 52 found no correlation between margin size and recurrence-free survival among patients with tumors smaller than 30 mm, but a wider surgical margin significantly improved recurrence-free survival when tumors were larger than 30 mm. Moreover, a wider surgical margin may limit the local recurrence and tumor infiltration by a residual microsatellite lesion. However, a wider surgical margin is also associated with less liver remnant and reduced liver function. In our study, no difference in survival was noted among these malignant patients (data not shown). Nevertheless, taking all the aforementioned advantages of the CDA into account, we believe that the CDA is more capable of allowing malignant lesions to be removed completely in LRH. However, further studies with larger samples and longer follow-up time are warranted for fuller evaluation of its oncologic benefit.
Laparoscopic liver resection is a complicated technique informed by a learning curve.13,29 With advancements in laparoscopic equipment and better patient selection, laparoscopic liver surgery can be performed safely, with improved operative and postoperative outcomes. Our comparison analysis (data not shown) between the last 10 CA cases and the CDA cases demonstrated that the initial CDA cases were not inferior to the later CA cases in terms of operative and postoperative outcomes. Better operative and postoperative outcomes can be expected from later CDA cases.
In conclusion, our study demonstrates that the CDA has operative and postoperative outcomes comparable to those of the CA. The CDA also achieves safety and feasibility similar to that of the CA. Moreover, use of the CDA in LRH requires fewer conversions to laparotomy than the CA. In selected patients, the CDA can be considered an alternative option to the CA for LRH in experienced expert hands. Further studies with larger samples of patients are warranted to delineate the benefit of the CDA for LRH.
Footnotes
Acknowledgments
The authors thank Dr. Zhu QC for her excellent work in helping design an elegant presentation of figures and also thank Dr. Yu TN for his warm help and practical guide in study design. Supported by Grants from the General Research Project of Medicine and Science of Zhejiang Province, No. 2014KYB119 and No. 2015KYB221.
Disclosure Statement
No competing financial interests exist.