
Abstract
Abstract
Objective:
The objective of our study is to evaluate the long-term results of laparoscopic bean vaginoplasty (LBV), which we previously described.
Materials and Methods:
From April 2002 to September 2013, 62 patients, who were diagnosed with Mayer–Rokitansky–Kuster–Hauser Syndrome and underwent LBV in Cukurova University School of Medicine Department of Obstetrics and Gynecology were included in the study. Operative data, complication rates, vaginal length, and sexuality of patients during the follow-up period were evaluated. Sexuality of the patients were evaluated using the Female Sexual Function Index (FSFI) questionnaire. The FSFI scores were compared with age-matched 65 healthy control subjects.
Results:
Mean age of patients in case and control groups were 23.9 ± 5.1 (18–32) and 25.1 ± 4.2 (18–31), respectively (P = .69). Median length of follow-up after surgery was 48 months (24–144 months). No complications occurred during the operations. No vaginal adhesions occurred during the follow-up periods. Median vaginal length during the last follow-up was 7 cm (6–9 cm). FSFI scores were similar with the control group.
Conclusion:
LBV is a successful modification of Vecchietti procedure, without any reported complication. However, the procedure should still be compared with the other methods in randomized trials.
Introduction
M
Primary amenorrhea and inability to have sexual intercourse are the main complaints of these patients. Currently, regular menses and pregnancy cannot be achieved for these patients because of the absence of the uterus. However, various methods are available for vaginal reconstruction. There are both nonsurgical and surgical reconstructive methods. Nonsurgical methods (most widely used is Frank's method) can be performed to cases with >1.5–2 cm distal vagina. This consists of gradual and long-term self-dilatation. 2 If dilatation is unsuccessful or patients are unwilling to use this method, surgery is indicated. Also, for cases without distal vagina (complete vaginal agenesis), surgical methods seem more appropriate.
Various surgical methods for vaginal reconstruction have been reported until now. McIndoe procedure is the most popular vaginoplasty method. It consists of creating a neovaginal space, which is subsequently covered by skin graft. Major concern for this surgery is the complexity of the technique and the remnant scar tissue on the site of the graft taken. 3 Different methods have been used for the lining of the canal. These include the use of peritoneum, bowel, amnion, adhesion barrier (Interceed®), allogenic epidermal sheets, autologous buccal mucosa, and autologous in vitro-cultured vaginal tissue.4–14
Today, the most popular surgical techniques for vaginoplasty are laparoscopic (L/S) peritoneal vaginoplasty (the Davydov technique), sigmoid Vaginoplasty, and modified Vecchietti techniques. L/S bean vaginoplasty (LBV) is a modified Vecchietti technique, which we previously described. 15 None of these techniques are regarded as superior to each other; all have distinctive advantages and disadvantages. In this article, we report our long-term results with the LBV.
Materials and Methods
From April 2002 to September 2013, 62 patients, who were diagnosed with MRKHS and underwent LBV in Cukurova University School of Medicine Obstetrics and Gynecology Department were included in the study. Patients who were operated later were not included in the study to evaluate long-term outcomes (at least 2 years). All patients gave informed consent for the procedure after careful explanation of all the available methods. Control group consisted of 65 healthy women aged between 18 and 31, who were admitted to our outpatient gynecology clinic for well-women visit and accepted to enroll in the study. The study was approved by the institutional local ethics board.
Patients were diagnosed as MRKHS after perineal inspection, transabominal and transrectal ultrasound, and hormonal profile, and karyotype testing confirmed the diagnosis. All cases had complete vaginal agenesis (without distal vagina). Possible coexisting urinary anomalies of all patients were evaluated with urinary system ultrasound and intravenous pyelogram (IVP). LBV was not performed on patients with pelvic kidney, to prevent inadvertent renal injury during the surgery.
Surgical procedure
As described previously by the authors, 15 the surgical procedure is shown in Figure 1.
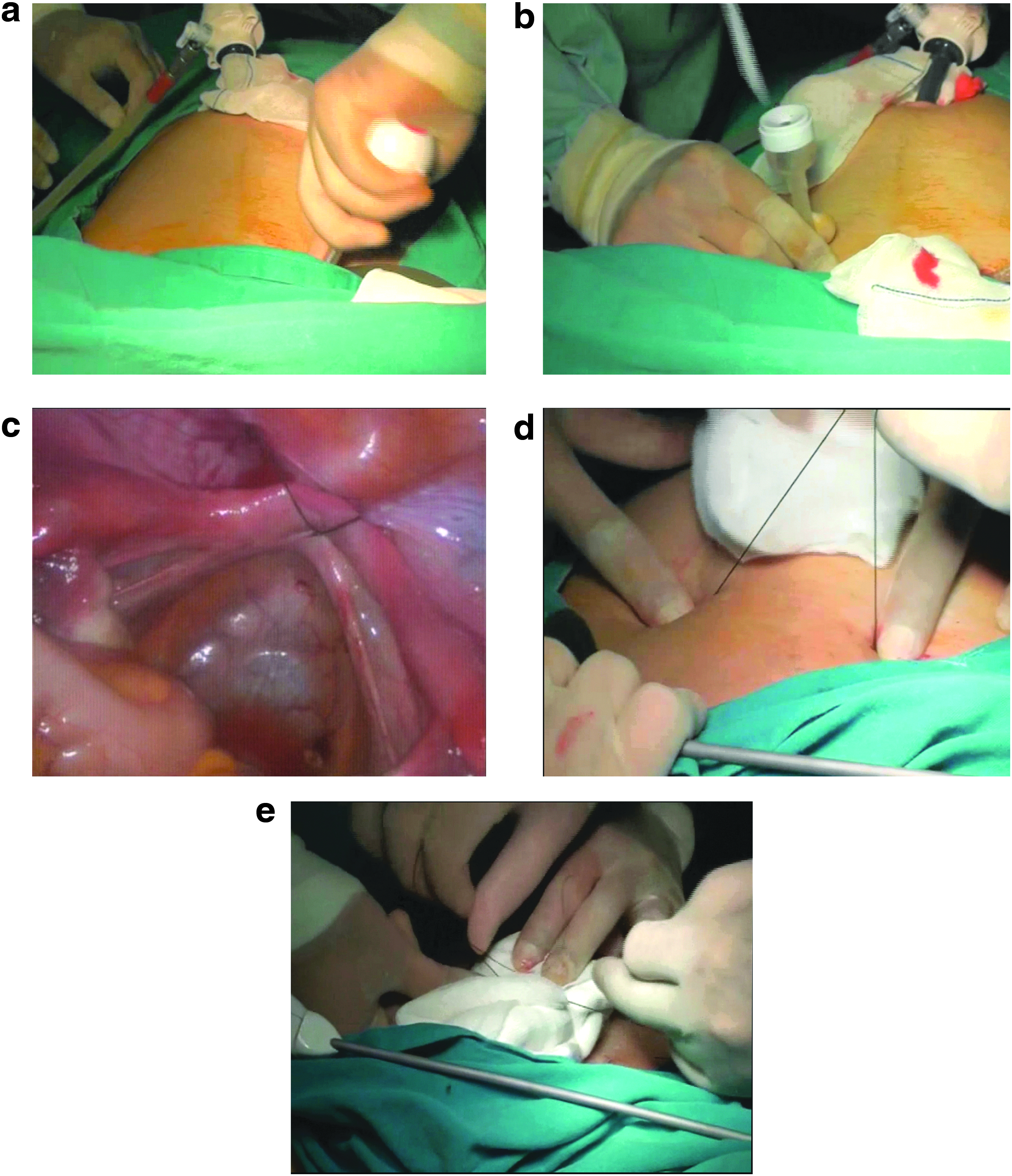
The operation.
For the LBV technique, a bean-shaped acrylic device was used, which is thought to be more suitable to the anatomy of the vaginal vault, because of its shape (Fig. 2). Under general anesthesia, the bladder was emptied by metal catheterization and adequate pneumoperitoneum was obtained. Then, the laparoscope was introduced through the 10-mm umbilical trocar. Two lateral 5-mm trocars were later introduced into the suprapubic region to allow an accurate exploration of the abdominal and pelvic organs. Traction sutures connected to the acrylic bean were inserted into the suture carrier needle (Fig. 3). The needle was then pushed forward through the space between the bladder and rectum into the abdominal cavity until it reached the level of the fibrous tissue (uterine rudiment), replacing the uterus.

The Bean is made of acrylic material.

Thirty-five centimeters of metallic needle used for insertion of the threads of the Bean.
At this point, cystoscopy was performed to confirm that the bladder was not perforated during the needle insertion. Atraumatic grasping forceps was then introduced under the parietal peritoneum from the 5-mm trocars toward the fibrous tissue, where they perforated the peritoneum with the help of scissors. The threads at the end of the needle were pulled below the parietal peritoneum at the sacrouterine level to above the suprapubic region with the grasping forceps on each side. After gentle traction, the two sutures were tied over sponges at the midline on the suprapubic region as much as tissues permitted, but care was taken for the tissue tension, as excessive traction can cause necrosis of the foveal epithelium. A traction device was not used.
Unless any bladder injury occurs, Foley catheter is kept for 2 days postoperatively. Patients were given prophylactic antibiotics (900 mg clindamycin phosphate every 8 hours and 1.5 mg/kg gentamicin daily) for 5 days. Routine analgesic treatment was given for 1 day, but was prolonged if patients needed. The suture was lifted by adding sponges, ∼1 cm every day to increase the traction, until a 7–8 cm long neovagina was achieved. (It takes 7–8 days on average) After the removal of the bean, mold was inserted using lidocaine gel, nitrofurazone cream, and estriol cream for 7 days. A supporting underwear was worn to prevent dislocation of the mold. All patients were then discharged with a 10-cm long and 2.5-cm wide dilatator (mold), which they used for 8 hours every day for 1 month.
After patients got used to the mold, patients were told to continue using the mold without lidocaine gel for 1 month. Two months after the surgery, patients' neovaginal epithelization was assessed using office vaginoscopy. In cases with adequate epithelization, sexual intercourse was initiated. Of those who did not have regular intercourse were suggested to continue using the dilatator for 6 months. Patients were also told to make Kegel exercises to strengthen the levator muscles. Follow-up visits were 1, 2, 6, and 12 months after the operation and every 6 months thereafter.
Both control group and case group patients who had begun sexual activity after the surgery, completed the Female Sexual Function Index (FSFI) questionnaire. FSFI questionnaire was given to patients at least 12 months after the surgery. Vaginal length of patients were also measured using a metal hysterometry device on each visit. As for the case group, the vaginal length and FSFI scores on the last visit were used. The FSFI results were compared with those of age-matched controls.
Statistics
For normally distributed data, parametric test (Student's t-test) was used, whereas for not normally distributed data, nonparametric test (the Mann–Whitney U-test) was used to compare results. The P-value of <.05 was considered as statistically significant. Statistical analysis was performed with Statistical Package for the Social Sciences (SPSS) version 15 software (SPSS, Inc., Chicago, IL).
Results
Mean age of patients in case and control groups were 23.9 ± 5.1 (18–32) and 25.1 ± 4.2 (18–31), respectively (P = .69). Fifty-five patients in the case group were married, whereas 63 patients in the control group. Seven patients stated that they do not have regular intercourse, whereas all women in the control group had regular sexual intercourse.
Seven patients with MRKHS had concomitant urinary anomaly (unilateral renal agenesis, urinary duplication, etc.) diagnosed with IVP and ultrasound. They were consulted with the urology department. Also, one patient did not have the fifth finger on her left hand.
Median length of follow-up after surgery was 48 months (24–144 months). All patients with MRKHS had primary amenorrhea and complete uterovaginal agenesis, but had normal secondary sexual characteristics, normal ovarian function, and a normal female karyotype (46, XX).
Operative data are shown in Table 1. No complications occurred during operations. Also, no vaginal adhesions occurred during the follow-up periods. FSFI scores of groups are compared in Table 2. Median vaginal length during the last follow-up was 7 cm (6–9 cm).
Student's t-test was used to compare groups.
FSFI, Female Sexual Function Index.
Discussion
Although regular menses cannot be achieved for patients with MRKHS, vaginal reconstruction is possible for these patients. Unable to have sexual intercourse is a significant burden for these patients. Today, various nonsurgical and surgical methods are used for reconstruction.
Frank's method, one of the initial methods, was first reported in 1938. It is the most commonly used nonsurgical method, which uses dilatators and patients need to use these for certain amount of time during the day. Despite high success rates, due to the discomfort by intermittent pressure by dilatators, it is not preferred by some patients. 3 For these patients surgical procedures may be an alternative.
McIndoe vaginoplasty is the classic surgical method that needs graft to be taken from other body parts. On account of this, donor site is cicatrized. Also, hair growth can occur on the graft tissue if full-thickness skin graft is taken. 15
L/S methods have also been reported: L/S peritoneal vaginoplasty (the Davydov technique) and L/S sigmoid vaginoplasty are the most popular L/S procedures. Also, several modifications of Vecchietti procedure have been described, each trying to improve the success rate. In Vecchietti procedure, an olive-shaped device is used for traction of the vaginal vault. In LBV, a bean-shaped device distributes the traction force bilaterally to left and right sides of the vaginal vault by the help of two threads. In our opinion, this creates a more physiologic vaginal shape, which in turn causes the long-term success with no adhesions.
In L/S peritoneal vaginoplasty (the Davydov technique), peritoneum is used to cover the vagina and a urinary catheter is kept for 5 days after the surgery. 16 Daily vaginal douching is performed and vaginal mold is used until she starts regular intercourse. Special surgical equipments are needed for peritoneal pushing and when compared with LBV, longer operation time and longer hospital stay have been reported in the comparison made by Liu et al. 16 Urinary complications (bladder and ureter injury, vesicovaginal fistula) both during and after the operation have been reported with this technique. 17
L/S sigmoid vaginoplasty uses patients' own intestines for reconstruction and therefore is a major operation and carries significant risks. 18 Reported complications include intestinal fistula, intestinal obstruction, peritonitis at the intestinal anastomotic stoma, incision infection, and neovaginal stenosis. 16 Also, vaginal discharge with foul smell is another important and undesired side effect of this surgery. 16
FSFI is an index used for sexual functions. FSFI scores of all these L/S surgeries are found to be similar. 16 LBV also showed similar FSFI scores both with the control group and with the previous studies. 16 Main goal for the treatment of MRKHS is creating a vagina with an appropriate length for sexual intercourse. All these methods therefore are effective for MRKHS patients. The selection among these methods should depend on the physician's experience in the procedure, complication rates of techniques, complexity of surgeries (operation time, etc.), and long-term effectiveness.
LBV is another modification of Vecchietti procedure. Main advantages of LBV, when compared with published results of other methods, are short operation time, less blood loss, less hospital stay, no reported complication, no scarring on body parts, no need for an abdominal device, no requirement for long durations of urinary catheterization, and similar FSFI scores with the control group.16,17,19–25
The main limitation of our study is that it lacks the comparison of LBV with other methods by randomizing some patients to other methods.
In conclusion, patients with MRKHS can have a neovagina. There are various methods for reconstruction. Classical operation methods can be modified to improve success rates and decrease complication rates. LBV is an effective modification of Vecchietti procedure. This is emphasized especially by our long-term successful results. However, it still needs to be compared with other methods, probably with large and randomized trials.
Footnotes
Disclosure Statement
No competing financial interests exist.