
Abstract
Abstract
Background:
Investigations indicate that natural orifice translumenal endoscopic surgery (NOTES) procedures induce a less pronounced postoperative inflammatory response than open or laparoscopic surgery, inflicting less trauma. In NOTES procedures, no skin incision is performed. We compare the inflammatory response added by the type of incision by measuring C-reactive protein (CRP) and tumors necrosis factor-alfa (TNF-α).
Methods:
Twenty-seven pigs were randomized to open surgical, laparoscopic, or transgastric NOTES abdominal access. After completion of the accesses, no surgery was performed. All accesses were left open for 40 minutes followed by closure, animals were survived for 7 days. Blood samples were drawn at the start of the accesses, at 20 and 40 minutes during the procedure, and at postoperative day (POD) 1, 3, and 7. Analyses of CRP and TNF-α were performed.
Results:
CRP increased in all animals until POD1. This increase was greater in the open group (P = .006). No significant differences in CRP-levels were found at POD 1, 3, or 7. TNF-α showed a peak during the procedure, at 20 and 40 minutes, with normalization at POD1 for 1/3 of the open and laparoscopic animals, but not for the NOTES animals. Due to variations within the groups, no statistical difference was shown between them. At postmortem, 1/3 of the pigs in the laparoscopic and open groups had wound infections, while no NOTES animals showed infections.
Conclusions:
This study provides no statistically significant differences in inflammatory response after the different abdominal accesses. However, the lack of a TNF-α-peak in the NOTES group might indicate a less pronounced response, supporting the initial theories.
Introduction
N
The total surgical trauma of an operation can be defined as the sum of the trauma of the abdominal access, the procedural trauma, and the trauma added by the duration of the procedure, the operation time. A previously published porcine study, in which transgastric NOTES uterine horn resection was compared with laparoscopic and open surgery, indicated that NOTES was less traumatic despite a three to four times longer operating time. 3 As NOTES procedures are performed without skin incision, this might be one of the reasons for inducing a less pronounced surgical trauma than both open and laparoscopic surgery. The aim of this study was to investigate if the access route into the abdominal cavity influences the postoperative inflammatory response comparing open surgical, laparoscopic, and transgastric NOTES abdominal accesses. In this survival porcine model, we chose to compare accesses mimicking cholecystectomy.
Materials and Methods
All procedures described were carried out in accordance with the requirements of the Directive 2010/63/EU and were evaluated and approved by the Animal Experimentation Ethics Committee of the Vall d'Hebron Research Institute (VHIR).
Design
Twenty-eight female Spanish hybrid landrace and large white pigs were randomized into three study groups to undergo access to the abdominal cavity as follows: open, laparoscopic, and transgastric NOTES. When the abdominal access was completed, the surgical retractors, ports, or the gastroscope for the NOTES group were left in place for 40 minutes. No surgical procedure was carried out. After the 40-minute period, closure of the skin wounds and the gastric wall was performed. All animals were survived and monitored for 7 days. They underwent a daily clinical evaluation during the study period. Blood samples were taken before and during the experiment and during the postoperative period for studies of inflammatory markers.
Endpoints
The main endpoint was to evaluate the systemic inflammatory response peri- and postoperatively, measuring CRP, WBC, and TNF-α, comparing the three groups.
Secondary endpoints were to evaluate postoperative weight gain during the survival period and to evaluate gross findings of infections, adhesions, or complications at postmortem.
Preparation
All animals were kept on liquid diet for 2 days before the study followed by free access to water 12 hours before the procedure. A single dose of intravenous antibiotic, ceftriaxone, was given at induction of anesthesia/analgesia and a bladder catheter was placed. All the procedures were performed under standard general anesthesia and under sterile conditions. Intraoperative monitoring consisted of electrocardiography, pulse oximetry, invasive blood pressure, and capnography.
Procedures
Operation time and incision length were recorded. Open and laparoscopic procedures were performed by four operators, all trained minimal invasive surgeons. The NOTES procedures were performed by two trained endoscopic surgeons and three gastroenterologists, well experienced in endoscopy and NOTES technique.
Open surgery (laparotomy)
A 12 cm right subcostal incision was made to access the abdominal cavity. Surgical retractors were left in place to expose the surgical wound for 40 minutes. The abdominal wall was carefully closed with a 0-0 running suture using resorbable monofilament in the fascia in two layers. The skin was finally closed with intracutaneous technique using a 2-0 resorbable monofilament suture.
Laparoscopy
Access to the abdominal cavity was obtained in the midline using standard open technique for the placement of the first 10 mm port. Pneumoperitoneum was established with CO2 at 12 mmHg. Under visual control, a 10 mm port was inserted in the subxiphoid area and two additional 5 mm ports were added in the right subcostal region. The four ports were left in place and the pneumoperitoneum was maintained at 12 mmHg for 40 minutes. After exsufflation, closure was performed using a 0-0 running resorbable suture in the fascia for the 10 mm ports. The skin was closed in all incisions with intracutaneous technique using a 2-0 resorbable monofilament suture. The total wound length was measured.
NOTES transgastric
A 2T-gastroscope was used for the procedure (2T GIF Q160; Olympus). It was disinfected with 70% alcohol before use. No gastric lavage was performed. Transgastric abdominal access was achieved on the anterior wall of the antrum using a standardized needle knife-guidewire-balloon-dilatation technique. 4 The access gastrotomy was dilated to 20 mm, and the gastroscope was brought out into the abdominal cavity. The accessory channel of the gastroscope was then connected to a standard laparoscopic insufflator to maintain a stable pneumoperitoneum using CO2 at 12 mmHg. The gastroscope was left in the abdominal cavity for 40 minutes, and the pneumoperitoneum was maintained at 12 mmHg. After withdrawal of the endoscope into the stomach, the gastrotomy was closed using two pairs of T-tags, Brace-Bars from Olympus, Japan (Fig. 1).
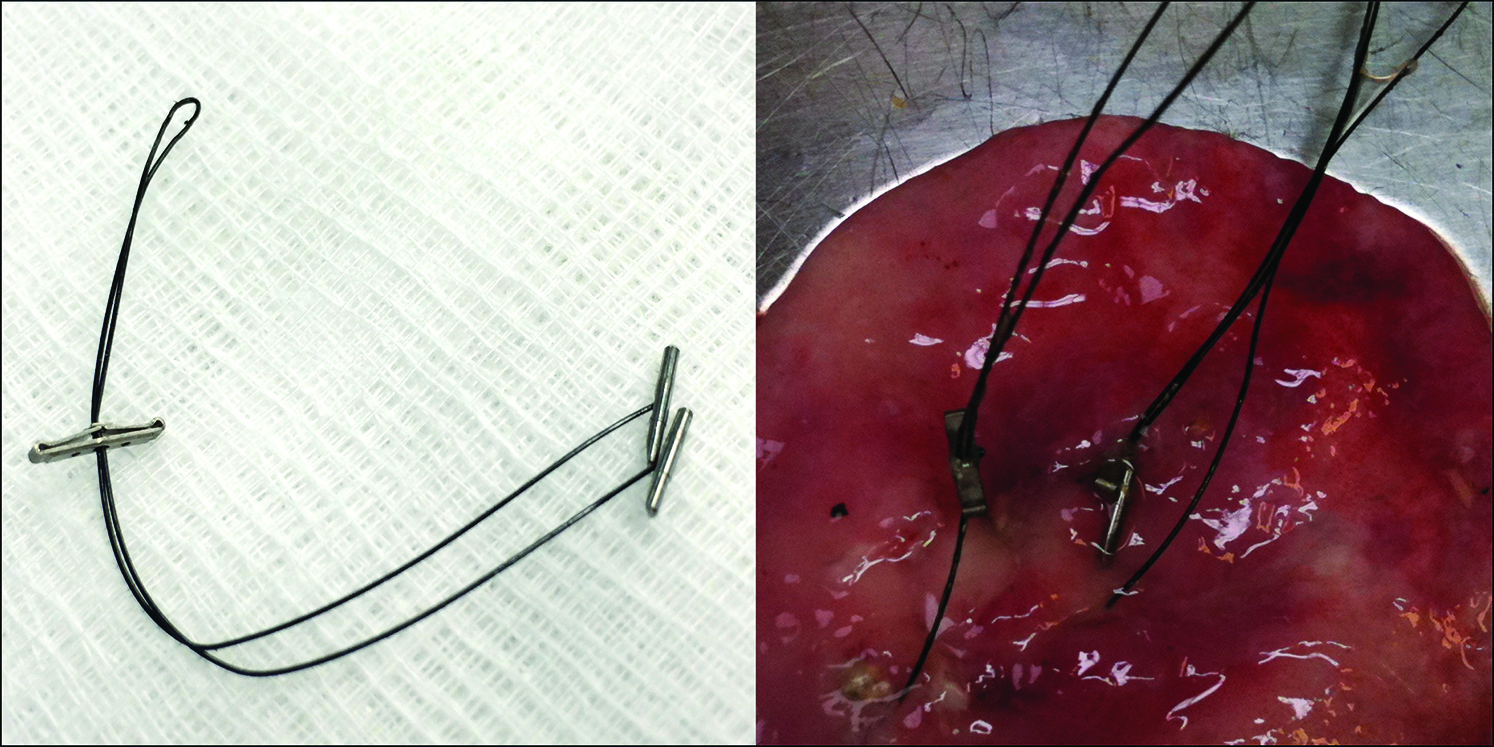
Brace-bars from Olympus, to the left before use and to the right at postmortem.
Blood samples
Venous blood samples were taken at the start of each procedure, after 20 and 40 minutes, and postoperatively at day 1 (at 24 hours), day 3, and before euthanasia at day 7.
The animals were sedated using Zoletil 100 (Tiletamina, Zolazepam) IM 4 mg/kg and Xilacina IM 2 mg/kg for each sampling occasion.
Blood samples were centrifuged at 4000 rpm at 4°C for 10 minutes and the plasma was frozen and stored at −70°C for further analyses.
Protein analyses were performed in batches using commercially available pig-specific ELISA Kits. For CRP (Immunology Consultants Laboratory, Inc.), lower detection limit was determined, using three standard deviations from the standard zero, to be less than 1.4 ng/mL. Intra- and interassay variations were less than 9%, respectively. For TNF-α (R&D Systems), lower detection limit was determined, using three standard deviations from the standard zero, to be less than 20 pg/mL. Intra- and interassay variations were less than 7% and 14%, respectively.
Follow-up
The animals were allowed free access to water and food as soon as they recovered from anesthesia. Body temperature and weight were recorded before the experiment and at postoperative day (POD) 1, 3, and 7.
Postmortem examination
The animals were euthanized at POD7. At necropsy, the abdominal cavity was opened with a long midline incision for complete exposure of the inside of the abdominal wall and cavity. The abdominal cavity and the access sites were carefully examined and documented for peritonitis, abscesses, abdominal adhesions, and other complications.
Statistics
Values are given as median with range for operating times and mean with ±SD for animal weight and plasma protein levels. Comparisons between groups were performed using nonparametric tests, the Kruskal–Wallis test for multiple nonrelated data, and the Wilcoxon sign-rank test for pairwise comparisons of related data. All statistics were processed using the SPSS 19 software. Differences were considered statistically significant at P < .05.
Results
Animals and procedures
Twenty-eight animals were included in the study. The initial mean weight for all animals was 32 kg (±3.4 kg [SD]) with no differences between the groups. All animals survived the procedure and the follow-up time of 1 week and gained weight according to expectations with no differences between the groups. The time for accessing the abdominal cavity was in median 10 minutes (6–16) in the laparoscopic group, 8 minutes (4–21) for the NOTES group, and 8 minutes (4–10) in the open surgery group. All exposures lasted for 40 minutes. The closure time was in median 19 minutes (5–21) in the laparoscopic group, 7 minutes (3–19) in the NOTES group, and 24 minutes (17–27) for the open surgical group. Closure took significantly shorter time after the NOTES access than after the open surgical access (P < .0001) and almost significantly shorter time than after the laparoscopic access (P = .051) (Fig. 2).
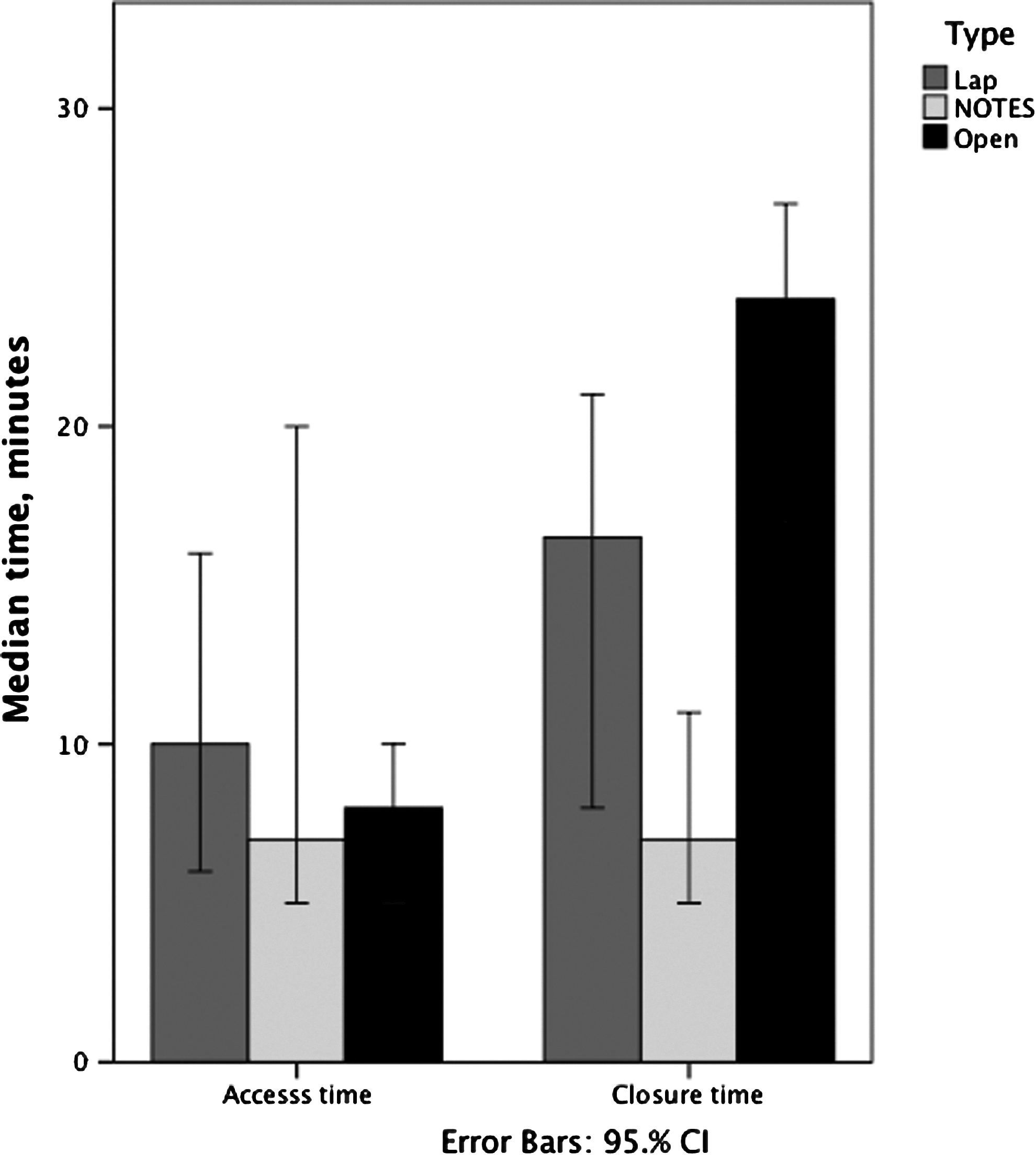
Recorded times for access of the abdominal cavity and for closure of the accesses using the three different techniques.
All animals survived the procedure and the follow-up time of 1 week.
C-reactive protein
Mean CRP at start of the procedure was 515 ng/mg protein (±277) with no significant differences between the groups. During the procedure (at 20 and 40 minutes), no changes were measured in CRP-levels. At POD1, CRP had increased significantly in all groups. The increase was significantly greater in the open access group (P = .006) compared with the other two techniques (Fig. 3).
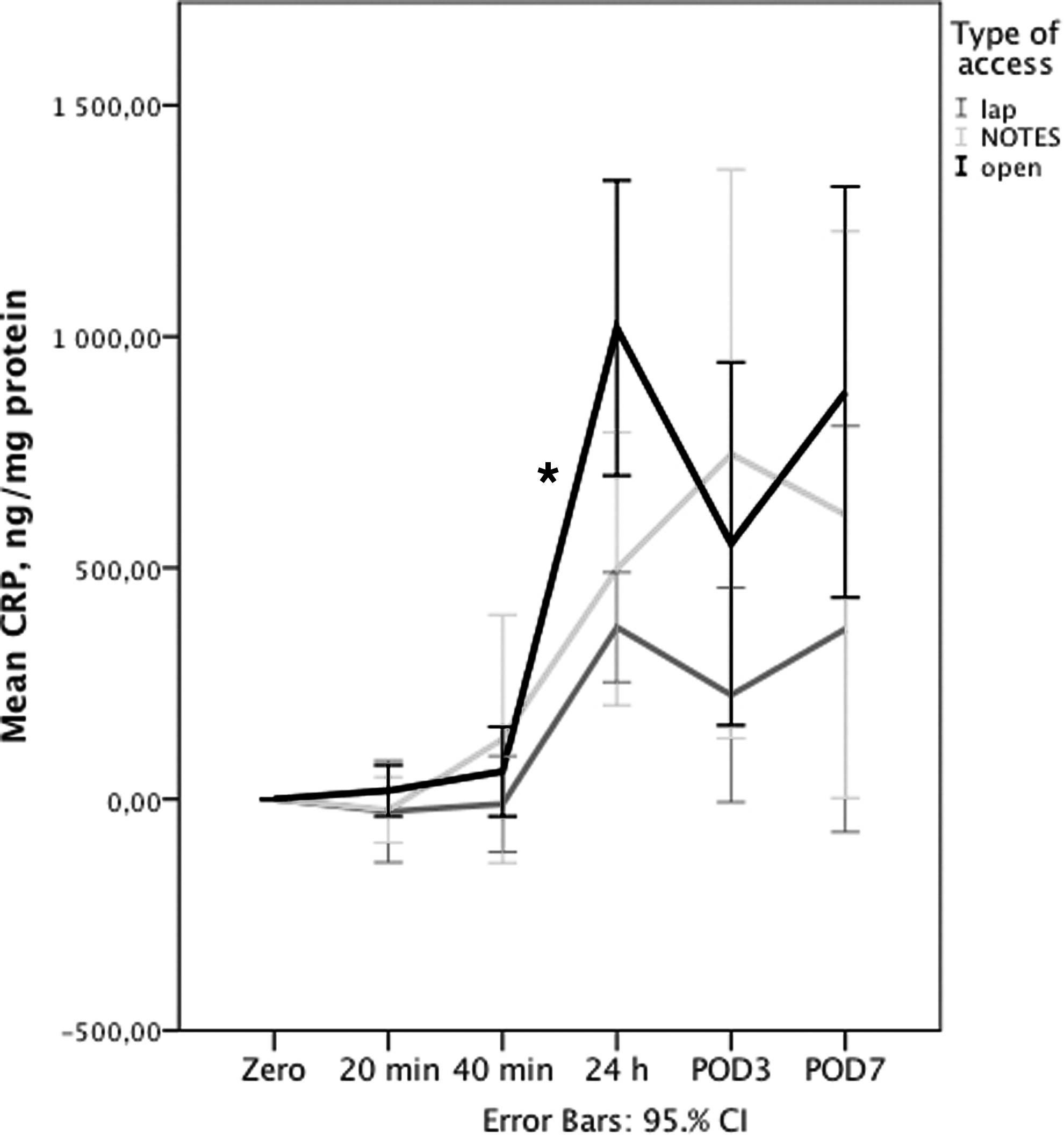
Mean levels of CRP at different time points. Note that the X-axis is nonlinear. The * indicates a significantly greater increase in CRP-level during the first 24 hours in the open group. CRP, C-reactive protein.
WBC
Mean WBC did not differ between the groups at any time point. All animals showed peroperative decrease (P = .0001) in WBC followed by a significant postoperative increase until POD1 (P = .0001). This increased WBC level persisted until POD7 for all groups (Fig. 4).
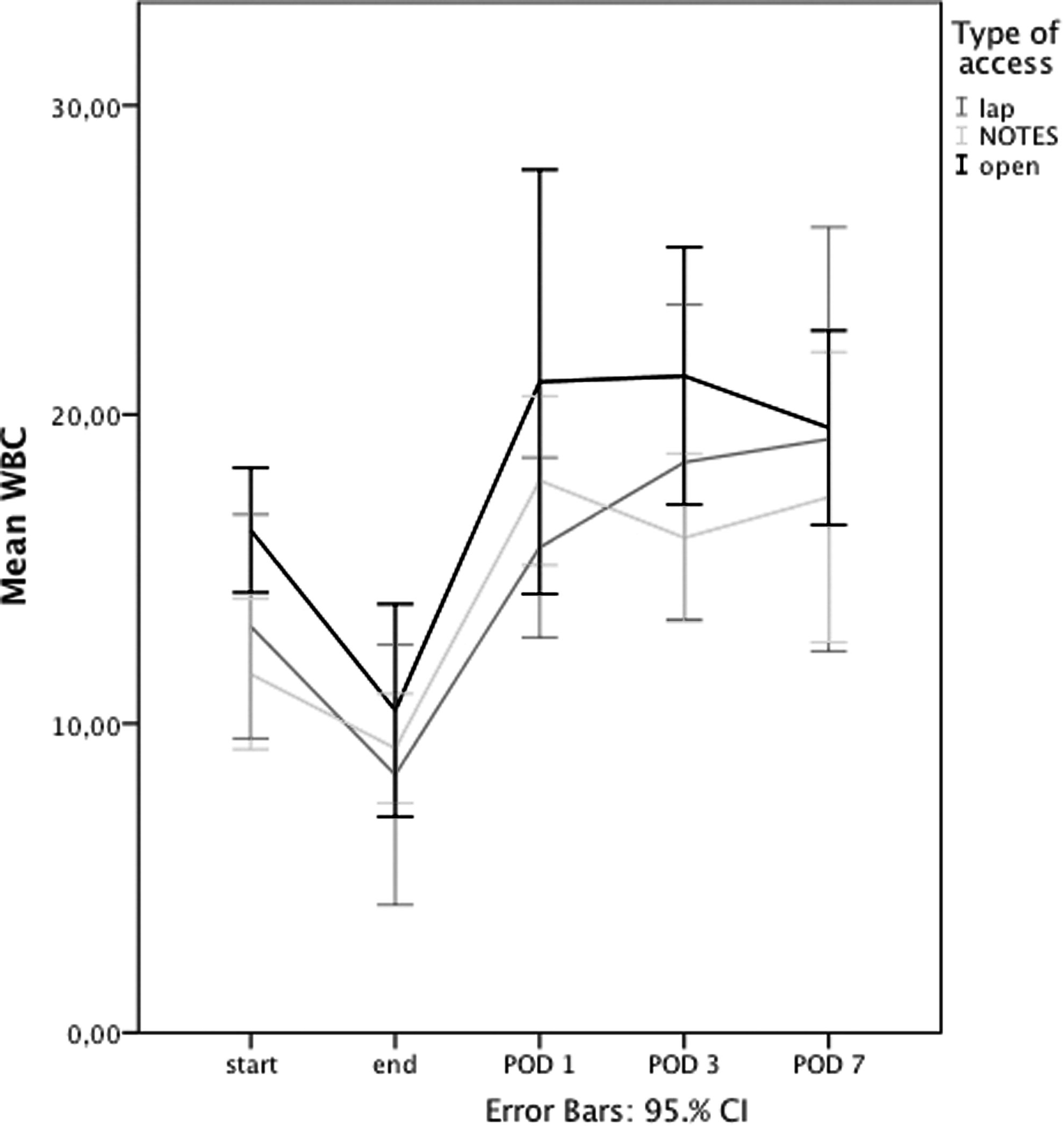
Mean WBC at different time points. Note that the X-axis is nonlinear.
Tumors necrosis factor-alfa
TNF-α levels seemed to follow two patterns. The majority of the animals showed little response during the procedures. However, 1/3 of the animals in both the laparoscopic and the open access groups responded to the trauma with a significant increase in TNF-α-levels during the exposure period (at 20 and 40 minutes). None of the NOTES animals showed this response. However, there were no statistically significant differences in the measured protein levels due to several “zero-responses.” All animals were normalized to the very low initial levels after 24 hours at POD1 (Fig. 5).
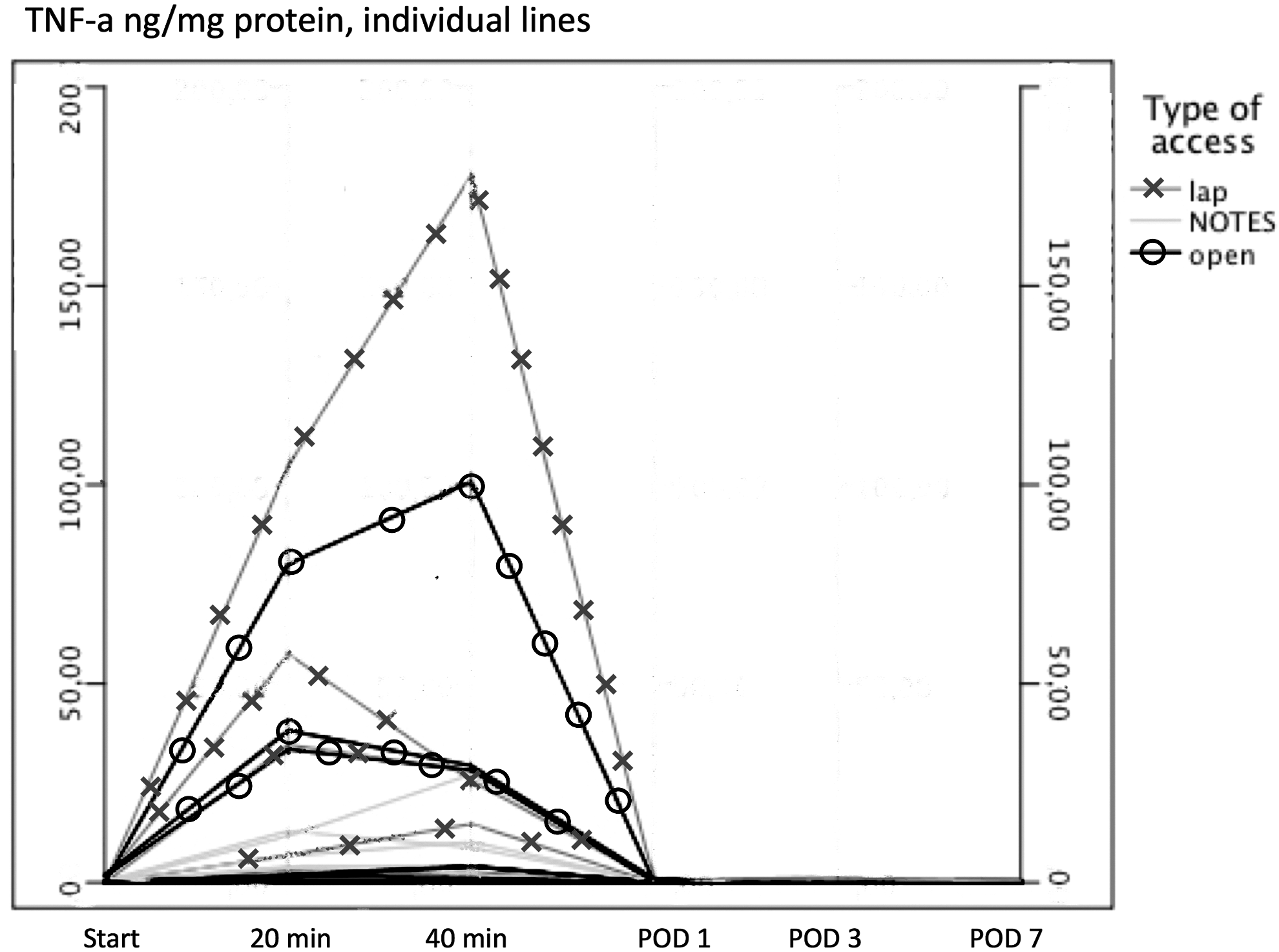
Levels of TNF-α, individual lines over time. Each line represents 1 animal. The 3 responding animals in the open and the laparoscopic groups are marked with O or X, but the nonresponding animals are not marked. TNF-α, tumors necrosis factor-alfa.
Postmortem
At postmortem, 3/9 animals in both the laparoscopic and the open surgical access groups had wound infections, but none of the NOTES animals had signs of peritonitis or local infections. All animals in the NOTES access group had an adhesive band between the omentum and the gastric access site, but no other intra-abdominal adhesions. In the open surgical access group, 6/9 animals showed intra-abdominal adhesions mainly to the liver and to the incision site. Only 1 animal in the laparoscopic group had adhesions, located at a port site (Fig. 6).
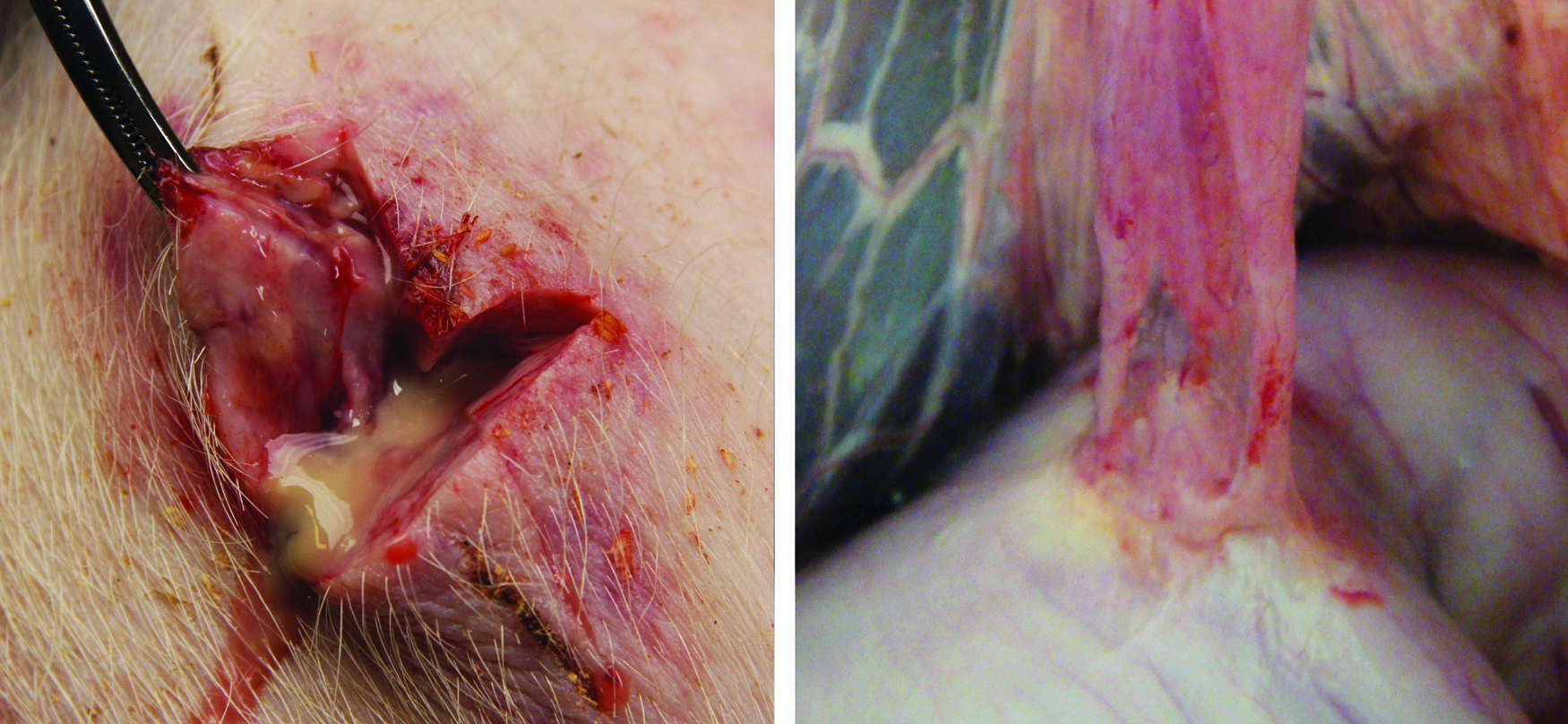
At postmortem: Infection in laparoscopic incision to the left and adhesion between the stomach and the abdominal wall after a NOTES access to the right. NOTES, natural orifice translumenal endoscopic surgery.
Discussion
Minimal access surgery is less traumatic than open surgery.1,5 NOTES procedures are believed to be even less traumatic, despite the often longer operating time. The total operating trauma of an abdominal procedure can be considered as the sum of the trauma of the access to the cavity, the trauma of the procedure itself, and the trauma added by the duration of the procedure. The original concept of NOTES involves an abdominal access without skin incisions. Previous publications analyze the postoperative inflammatory response after different surgical procedures.
In the current study, we aim at isolating the effects of the access route into the abdominal cavity using a model utilizing the accesses needed for a cholecystectomy. At 20 minutes after the access, a peroperative peak in TNF-α was shown in 1/3 of the open and laparoscopic access animals, but in none of the NOTES animals. The TNF-α responding animals did not have a more complicated access procedure or longer access time that might explain this reaction. We, therefore, regard it as a response to the access trauma through the skin.
The serum level of CRP is a well-accepted marker of postoperative stress response.1,2,6 Its increase is part of the postoperative cascade effect initiated by TNF-α. 7 The peak level of CRP is expected about 24 hours after surgery, which is reproduced in our study. All groups showed an increase in serum CRP between end of the procedure and POD1 (24 hours), but the increase was significantly greater in the open access group than in the other two groups. There was no statistical difference in CRP-levels comparing the groups at POD1, but there was a clear trend (Fig. 2). This finding differs slightly from our previous study where only the NOTES animals had a significantly lower CRP-level at POD1. 3
Recently, many investigators have published experimental studies comparing stress response after NOTES and laparoscopic surgery. Varying parameters have been investigated during different surgical procedures and time points, why comparisons are difficult. Some have found a lower inflammatory response after NOTES procedures 8 and others have found no differences.9–11 In some studies, invasive procedures like drain placement and placement of central vein catheters have been performed before the NOTES procedure, increasing the degree of trauma and making inference difficult. 9 Many studies compare laparoscopy using CO2 with NOTES using air insufflation, thus altering the peritoneal response to trauma. 12 In our recently published study comparing postoperative stress response after open, laparoscopic, and NOTES transgastric uterine horn resection in pigs, we found results indicating a lower stress response in the NOTES group. 3 In the most recent publication on this subject, Wang et al. compared the postoperative inflammatory response after standard laparoscopy and transgastric NOTES peritoneoscopy using two different sized endoscopes without finding any differences. 11 No study has specifically targeted the access trauma.
There are many similarities between laparoscopy and NOTES peritoneoscopy. The obvious difference is the access route, through the abdominal wall or through the viscera. In our animal model, CO2 was utilized for creating pneumoperitoneum in both groups making the comparison more fair. The transgastric NOTES group showed an inflammatory response close to the laparoscopic group. This response might be due to leakage of gastric contents into the abdominal cavity. The leakage does not seem to induce infections, as shown in this study and in previous studies, 13 but might influence the inflammatory response.
Wound incisions always carry a risk of wound infections, attenuated in animal models, as shown in the current study (6/18 animals). In humans, the rate of wound infections after laparoscopic procedures is low, often less than 1%, 14 why the clinical relevance of this parameter in a swine model can be questioned. Another drawback with animal models that include blood sampling is the need for sedation/anesthesia during the sampling. These sampling procedures increase the postoperative biologic trauma and might also influence the results, as well as the postoperative recovery.
The theoretical advantage with NOTES is difficult to prove experimentally in animal models. Our present study shows no obvious advantage with transgastric NOTES route compared to standard laparoscopy. The access route in itself does not seem to be the key to less traumatic surgery.
With current knowledge, it is difficult to justify pure NOTES procedures with longer operating time and expensive instrumentation. However, the NOTES evolution has brought new operating techniques, including hybrid procedures and the use of flexible endoscopy in surgical practice initiating new ideas thinking outside the box.
Footnotes
Acknowledgments
WIDER Institute and Vall d'Hebron Hospital, Barcelona. Stiftelsen Borås Forsknings- och utvecklingsfond mot cancer (928/19). Olympus, Sweden for supplying “Brace-Bar” T-tags.
Disclosure Statement
No competing financial interests exist.