
Abstract
Abstract
Objectives:
To compare the safety and efficacy of thulium laser resection of prostate (ThuRP) and plasmakinetic resection of prostate (PKRP) for benign prostate hyperplasia (BPH), we made this meta-analysis in regard of the two techniques.
Methods:
A systematic search of PubMed, Web of Science, and China National Knowledge Infrastructure was performed up to October 1, 2015. Outcomes of interest assessing the two techniques included demographic and clinical characteristics, perioperative variables, follow-up data, and complications.
Results:
Nine eligible trials evaluating ThuRP versus PKRP for BPH were identified, including six randomized controlled trials (RCTs) and three retrospective trials. ThuRP was associated with longer operation time (P < .001), shorter hospital stay (P < .001), irrigation (P = .02), and catheterization (P < .001) duration. Estimated blood loss (P = .005) and drop in hemoglobin level (P = .02) were significantly more in PKRP. Except quality of life score (P = .04), which was better in ThuRP, the postoperative data, including international prostate symptom score (P = .44), Qmax (P = .33), postvoid residual urine volume (P = .55), and the complications such as severe bleeding (P = .52), temporary urinary retention (P = .20), temporary urinary incontinence (P = .64), urinary tract infection (P = .83), and urethral stricture (P = .22), did not differ significantly.
Conclusion:
Our analysis showed that there was no significant difference in terms of efficacy between ThuRP and PKRP. Although ThuRP was associated with longer operation time, it possessed more safe capacity with less blood loss, shorter hospital stay, irrigation, and catheterization duration. More worldwide RCTs with long-term follow-up are still needed to support our conclusion.
Introduction
F
In recent years, a number of new techniques, including laser and bipolar plasmakinetic energy, have been developed as references for the treatment of BPH and showed many advantages over conventional TURP. 5 Plasmakinetic resection of prostate (PKRP), as a modification of monopolar TURP, which is performed in normal saline, has similar efficacy with TURP, but is preferable due to a more favorable safety profile with fewer adverse events.2,6 Laser technique has advanced dramatically during the last decade. The efficacy and safety of holmium laser enucleation of prostate (HoLEP) and potassium-titanyl-phosphate/GreenLight laser vaporization of prostate (PVP) have been supported by current evidences 7 and both are recommended by the current guidelines. 3
Since thulium laser resection of prostate (ThuRP) was first described by Fried in 2005, 8 it has been preferred by urologists owing to its excellent characteristics in terms of safety and efficacy.9–11 However, as a newly introduced technique, the limited number of single trials does not permit final conclusions regarding the efficacy of thulium laser treatment for BPH.3,12 There is already a meta-analysis revealing several advantages in ThuRP over conventional TURP. 13 However, the comparison of ThuRP with PKRP, the modification of TURP, has not been demonstrated. So we made this meta-analysis comparing safety and efficacy between ThuRP and PKRP to assess the capacity of thulium laser for the surgical treatment of BPH.
Materials and Methods
Study selection
A systematic search of PubMed, Web of Science, and China National Knowledge Infrastructure was performed to recognize all published trials up to October 1, 2015 comparing ThuRP and PKRP with following MESH search headings: “comparative studies,” “thulium laser resection of prostate,” “plasmakinetic resection of prostate,” and “benign prostate hyperplasia.” The “related articles” function was used to broaden the search, and all abstracts, studies, and citations were reviewed.
Inclusion criteria and exclusion criteria
Trials were included if they met the following criteria: (1) randomized controlled trials (RCTs) or non-RCTs, (2) the comparison of ThuRP with PKRP, (3) patients with BPH who suffered from LUST, and (4) reports on at least one outcome of interest mentioned below, and the relative data were reported or could be calculated.
Trials were excluded if: (1) patients had other disease such as prostate cancer or neurogenic bladder, and (2) no outcomes of interest (specified later) were reported or impossible to calculate or extrapolate the necessary data for either ThuRP or PKRP from the published results.
Data extraction and outcomes of interest
Two reviewers independently extracted the following data, including: first author, year of publication, country, study interval, study design, number of patients who underwent ThuRP or PKRP, follow-up time, and outcomes of interest. The extracted outcomes included patients' baseline characteristics, including: age, prostate volume, prostate-specific antigen (PSA) level, international prostate symptom score (IPSS), quality of life (QoL) score, maximum urinary flow rate (Qmax), and postvoid residual urine volume (PVR); perioperative and postoperative variables, including: operating time, estimated blood loss, length of hospital stay, irrigation duration, drop in hemoglobin level, catheterization time, postoperative IPSS, QoL score, Qmax, and PVR; and complications including: severe bleeding, temporary urinary retention, temporary urinary incontinence, urinary tract infection, and urethral stricture. All disagreements about eligibility were resolved by discussion between all authors until a consensus was reached.
Study quality and level of evidence
The level of evidence of included studies was rated according to criteria by the Centre for Evidence-Based Medicine in Oxford, United Kingdom. 14 Two reviewers independently assessed the quality of the studies and disagreement was resolved by consensus.
Statistical analyses
We performed this meta-analysis according to the recommendations of the Cochrane Collaboration and the Quality of Reporting of Meta-analyses guidelines. 15 All the statistical analyses were performed using RevMan 5.3 (Cochrane Library Software, Oxford, United Kingdom). For continuous variables, weighted mean difference (WMD) was used and for dichotomous parameters, odds ratio (OR) was used, respectively, both with 95% confidence interval (CI). All the pooled effects were determined by the z test, and P < .05 was considered statistically significant. The quantity of heterogeneity among included studies was assessed by chi-square-based Q test and I2 test, when I2 < 50%, P > .05; when the evidences showed no heterogeneity, we used fixed-effects model, otherwise we used random-effects model. Sensitivity analysis was carried out in RCTs. Variables were pooled only if outcomes were reported by three or more studies in the overall meta-analysis. Publish bias was assessed by funnel plots.
Results
Characteristics of selected studies
After screening, nine trials16–24 with totally 463 cases of ThuRP and 527 cases of PKRP were selected for this meta-analysis, including six RCTs18–20,22–24 and three retrospective ones16,17,21 (Fig. 1). The characteristics of these studies are shown in Table 1.
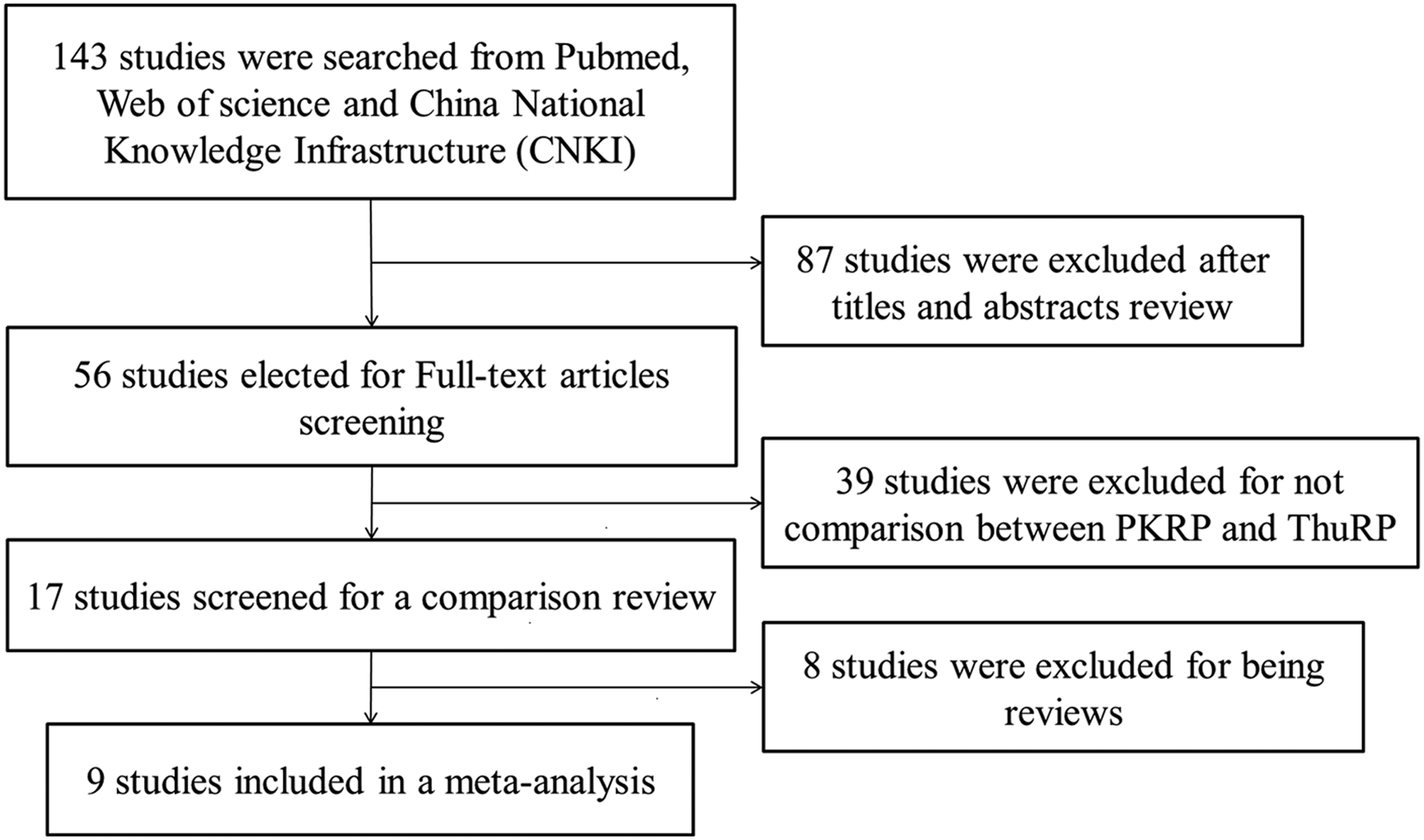
Flowchart showing the selection of studies for meta-analysis.
Based on US preventive services task force grading system.
Matching/comparable variables: 1 = age, 2 = prostate volume, 3 = PSA (prostate-specific antigen) level, 4 = IPSS (international prostate symptom score), 5 = QoL (quality of life) score, 6 = Qmax (maximum urinary flow rate), and 7 = PVR (postvoid residual urine volume).
ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate; LOE, level of evidence; RCT, randomized control trial; NA, data not available.
Outcomes of demographic and clinical characteristics
Patients in ThuRP group were associated with older age. There were no significant differences with respect to prostate volume, PSA level, IPSS, QoL score, Qmax, and PVR between ThuRP and PKRP (Fig. 2). The results are shown in Table 2.
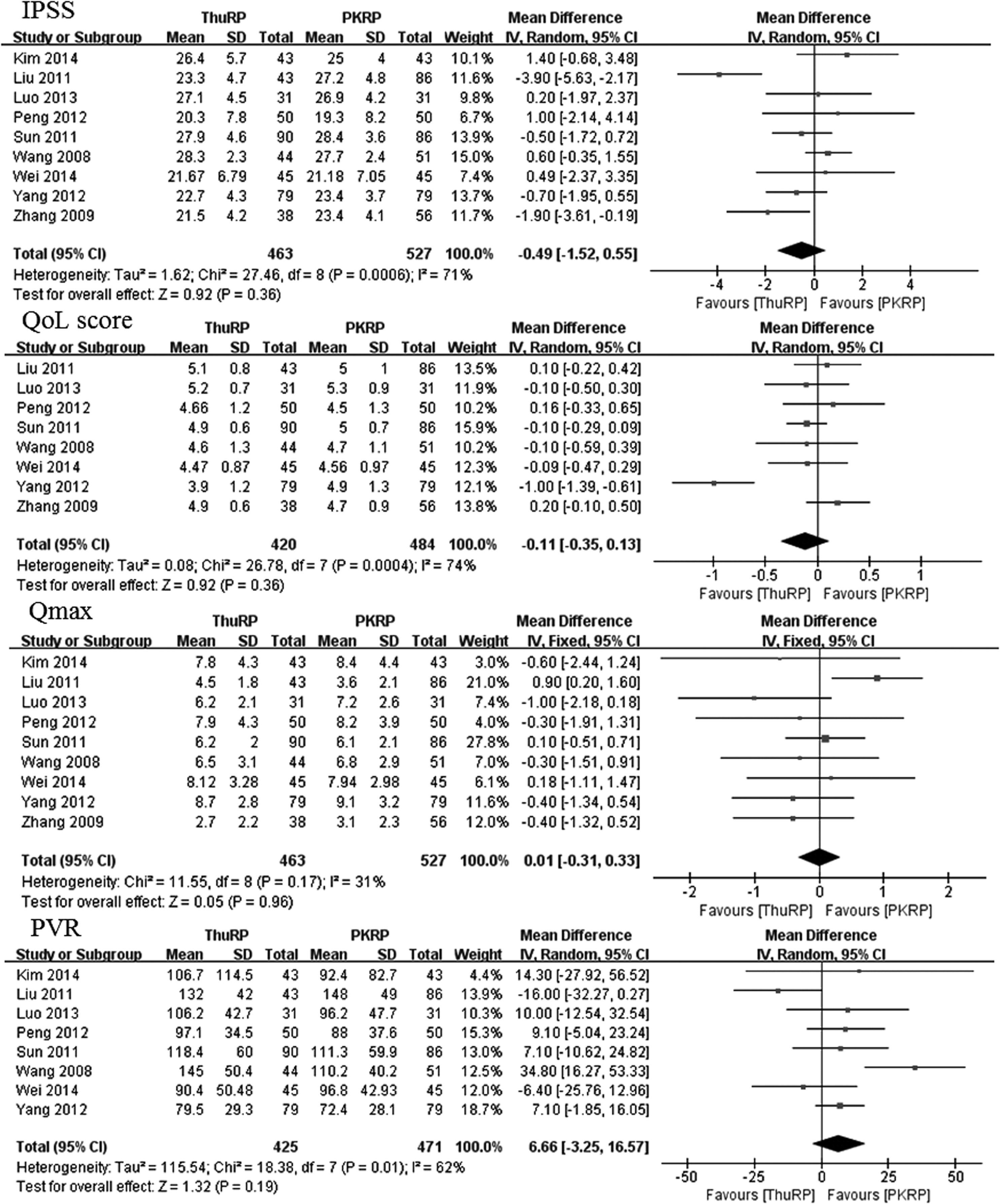
Forest plot and meta-analysis of preoperative IPSS, QoL score, Qmax (mL/s), and PVR (mL). IPSS, international prostate symptom score; QoL, quality of life; Qmax, maximum urinary flow rate; PVR, postvoid residual urine volume; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Statistically significant results are shown in bold.
CI, confidence interval; WMD, weighted mean difference; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate; PSA, prostate-specific antigen; IPSS, international prostate symptom score; QoL, quality of life; Qmax, maximum urinary flow rate; PVR, postvoid residual urine volume.
Outcomes of perioperative variables
The operation time (WMD: 15.82; 95% CI: 9.61–22.03; P < .001) was longer in ThuRP, but the hospital stay (WMD: −1.78; 95% CI: −2.35 to −1.22; P < .001), irrigation time (WMD: −22.59; 95% CI: −41.13 to −3.88; P = .02), and catheterization time (WMD: −1.74; 95% CI: −2.62 to −0.86; P < .001) were clinically relevant and shorter compared with PKRP. There was less estimated blood loss (WMD: −34.92; 95% CI: −59.18 to −10.67; P = .005) and less drop in hemoglobin level (WMD: −0.56; 95% CI: −1.06 to −0.08; P = .02) in the ThuRP group. The results are shown in Table 3 (Fig. 3).
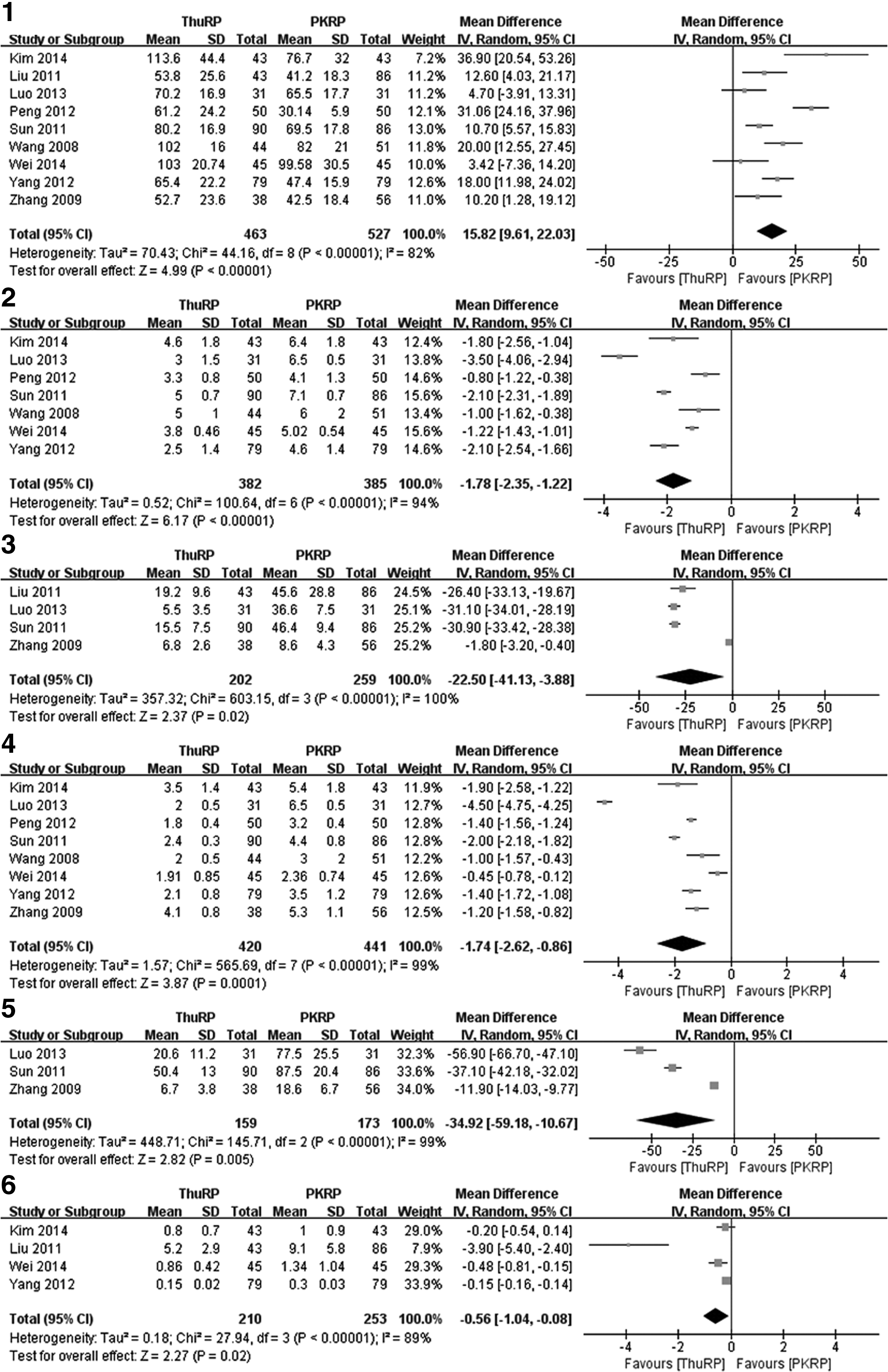
Forest plot and meta-analysis of perioperative variables.
Statistically significant results are shown in bold.
CI, confidence interval; WMD, weighted mean difference; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Outcomes of postoperative clinical characteristics
Postoperative clinical characteristics such as IPSS (WMD: 0.09; 95% CI: −0.14 to 0.31; P = .44), Qmax (WMD: 0.41; 95% CI: −0.41 to 1.23; P = .33), and PVR (WMD: 0.29; 95% CI: −0.65 to 1.24; P = .55) had no significant difference between ThuRP and PKRP. Postoperative QoL score (WMD: −0.20; 95% CI: −0.39 to 0.01; P = .04) was even better in the ThuRP group. The results are shown in Table 4 (Fig. 4).
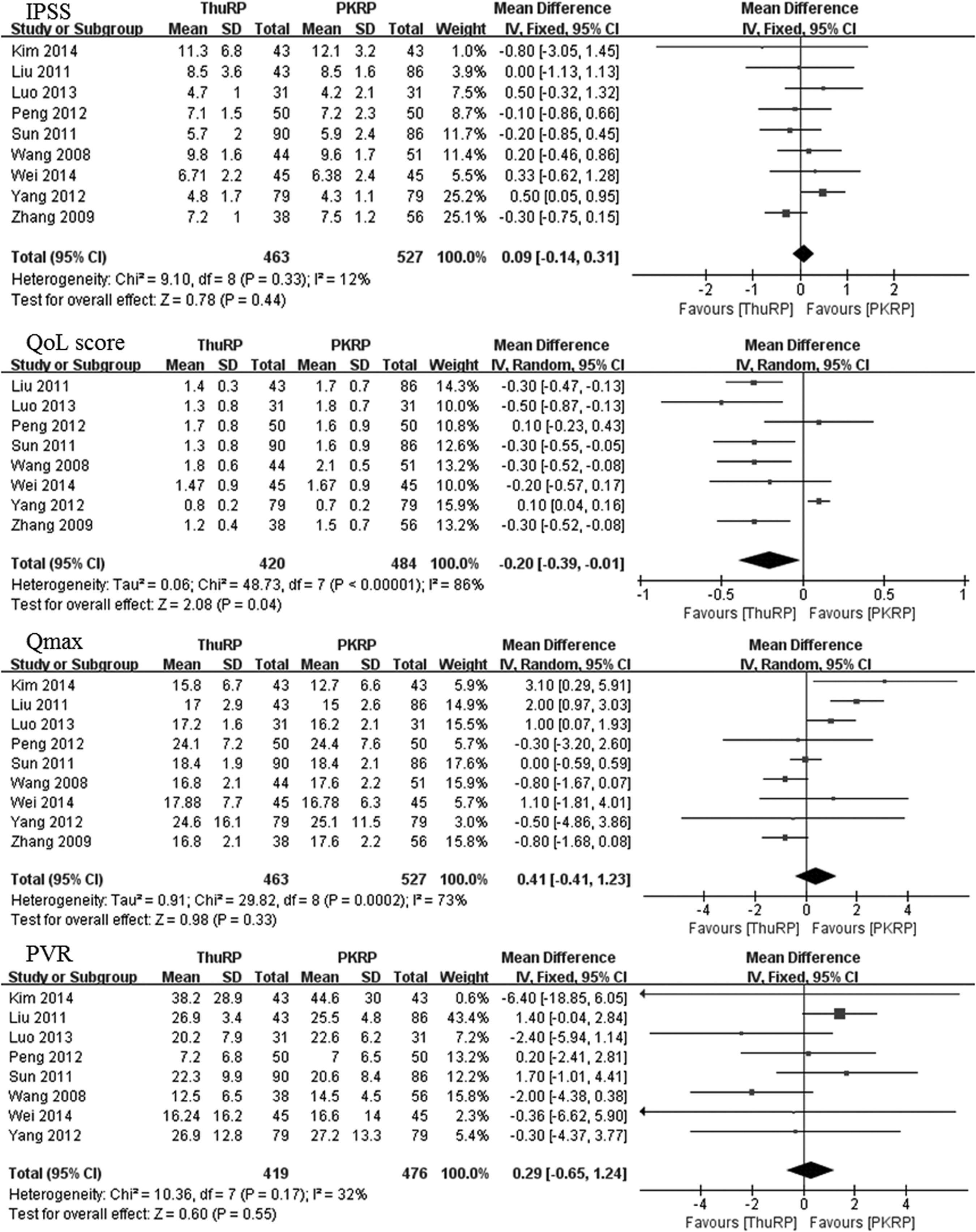
Forest plot and meta-analysis of postoperative IPSS, QoL score, Qmax (mL/s), and PVR (mL). IPSS, international prostate symptom score; QoL, quality of life; Qmax, maximum urinary flow rate; PVR, postvoid residual urine volume; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Statistically significant results are shown in bold.
CI, confidence interval; WMD, weighted mean difference; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Outcomes of complications
There were no differences in complications, including severe bleeding that need transfusion (OR: 0.74; 95% CI: 0.30 to 1.86; P = .52), temporary urinary retention (OR: 0.67; 95% CI: 0.36 to 1.23; P = .20), temporary urinary incontinence (OR: 1.22; 95% CI: 0.53 to 2.77; P = .64), urinary tract infection (OR: 0.91; 95% CI: 0.39 to 2.13; P = .83), and urethral stricture (OR: 0.54; 95% CI: 0.20 to 1.45; P = .22), between the two groups. These results are shown in Table 5 (Fig. 5).
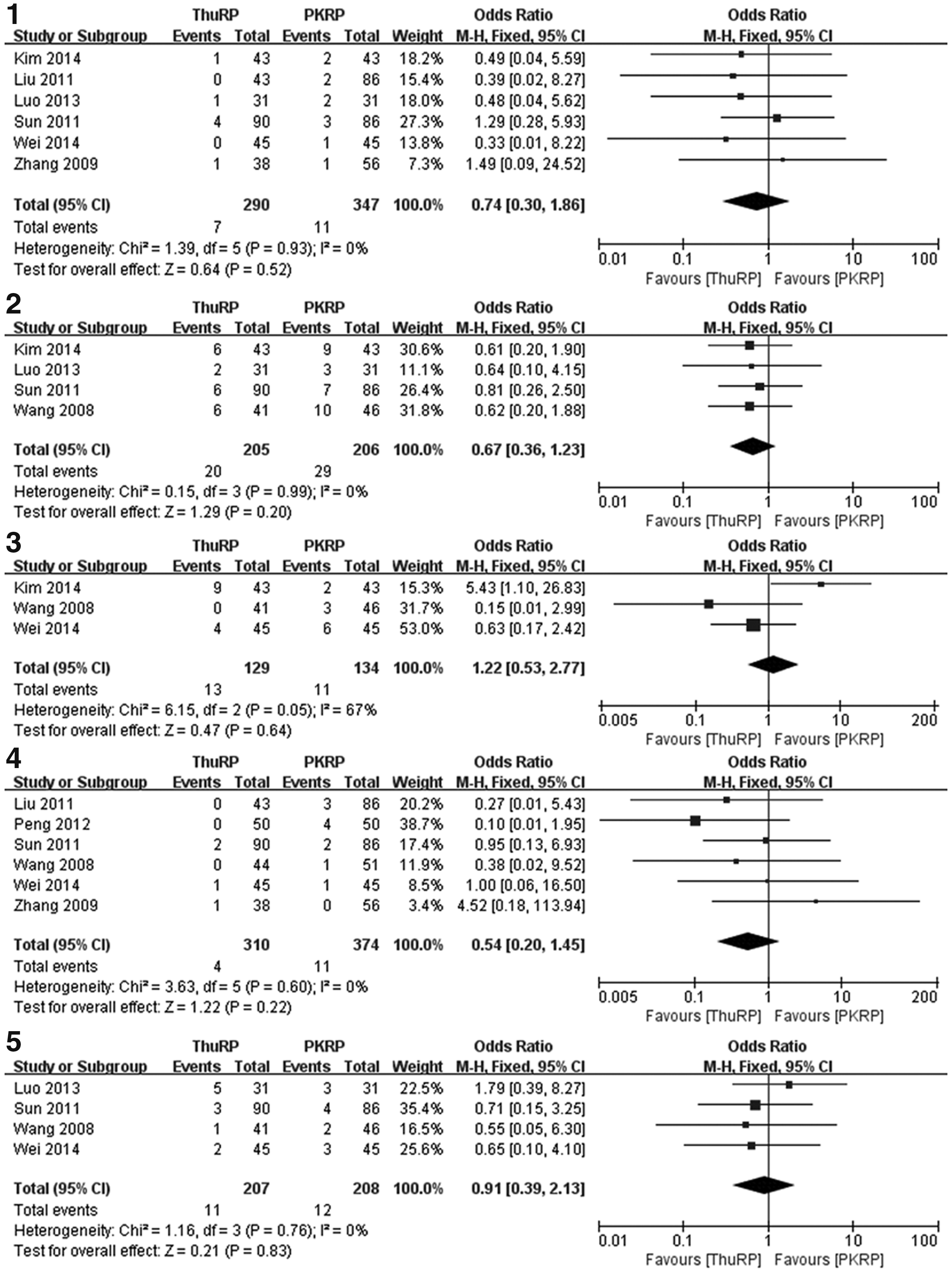
Forest plot and meta-analysis of overall complications.
CI, confidence interval; OR, odds ratio; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Sensitivity analysis and publication bias
Sensitivity analysis was carried out by subgroup of six RCTs; the results are shown in Table 6. Except that the irrigation time (P = .02 vs. P = .06) and postoperative QoL score (P = .04 vs. P = .15) were significantly different, there was no change in significance compared with the original analysis, indicating that the results of our meta-analysis were stable. Funnel plots were used to assess the publication bias of included studies. No significant publication bias was found in all the analysis. As an example, we present the funnel plot of operation time showing no obvious asymmetry (Fig. 6).
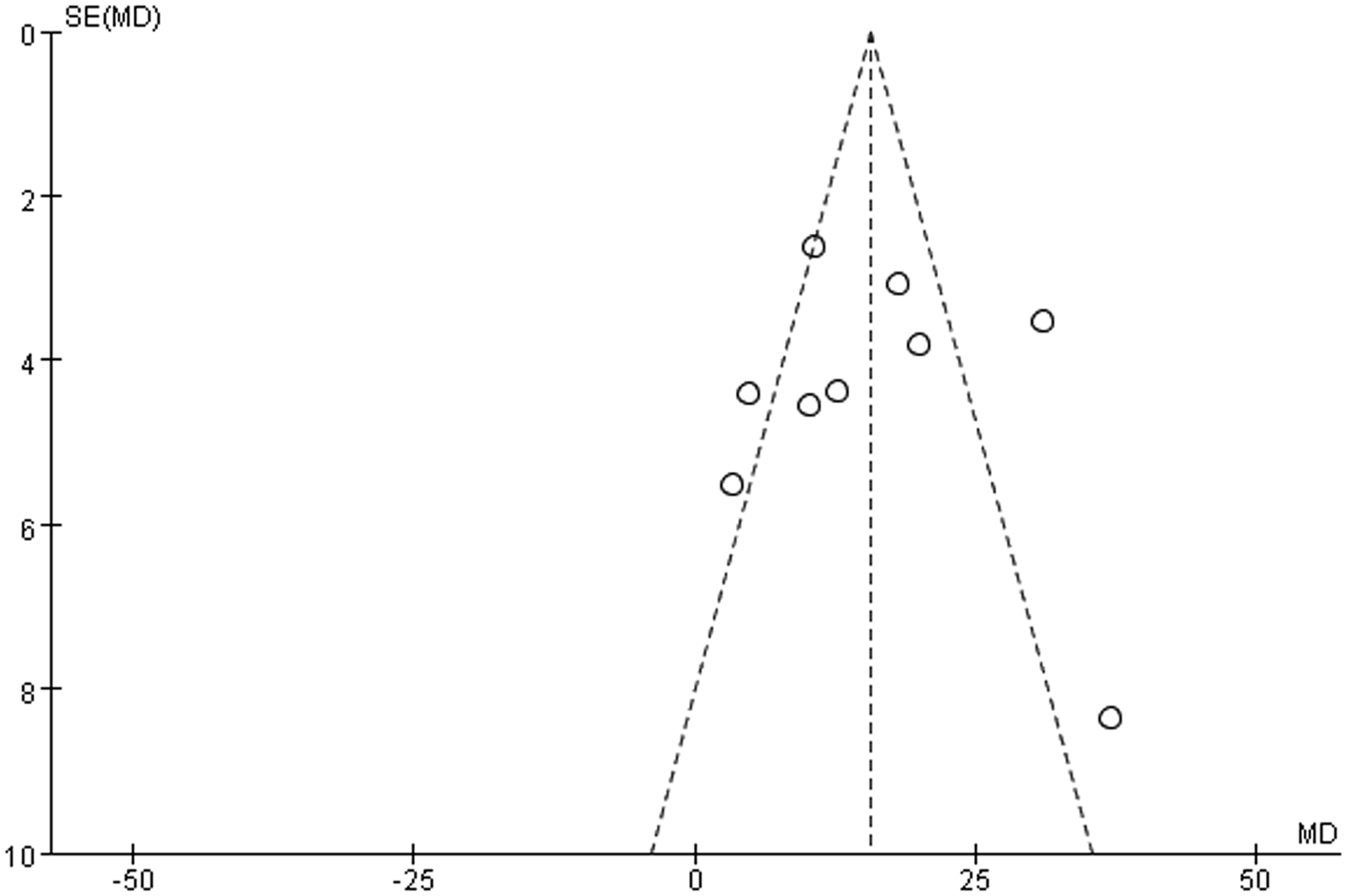
Funnel plot of operation time.
Statistically significant results are shown in bold.
Values of WMD.
CI, confidence interval; OR, odds ratio; RCTs, randomized controlled trials; WMD, weighted mean difference; ThuRP, thulium laser resection of prostate; PKRP, plasmakinetic resection of prostate.
Discussion
TURP, which is still considered as the standard surgical treatment of BPH, is being challenged by new improved techniques. As a modification of conventional monopolar TURP, bipolar plasmakinetic TURP has been demonstrated as a safe and efficient procedure. It is performed using normal saline for irrigation, reducing the risk of TUR syndrome, and possesses better hemostasis, providing a more clear operation visibility. PKRP has similar efficacy of TURP, but a significantly lower complication rate and shorter irrigation and catheterization duration. 6 As a promising technique, PKRP has been considered as the preferred choice instead of TURP.
The laser techniques such as HoLEP and PVP have been widely used and their advantages in terms of safety and efficacy have been proven compared with conventional TURP. 5 HoLEP is suitable for prostate of any volume, even those who required open prostatectomy before and PVP can achieve genuine instant tissue ablation, promising for durable results. 2 Thulium laser was introduced for the resection of prostate in 2005, 8 and since then, this kind of technique has developed rapidly. Thulium laser has two wave modes, continuous or pulse with a wavelength tunable from 1.75 to 2.22 μm, which matches the water absorption peak of 1.92 μm for more efficient tissue ablation. 11 Its power can be raised up to 150 w with minimal thermal injury and perfect ability of hemostasis allowing safe surgery in patients who are taking oral anticoagulation. 25 Compared with the other two widely used laser techniques for the treatment of BPH, thulium laser theoretically has several advantages such as more efficient operation, improved spatial beam quality, and more precise incision of tissues.8,26,27 Unlike PVP, ThuRP can also provide tissue specimens for pathological test with good maintenance of tissue histological characteristics and properties. 28
In our meta-analysis, the operation time was longer in ThuRP than PKRP. However, the difference of about 15 minutes was of limited clinically relevant significance. The probable explanation is that the surgeons were already practiced of standard procedure of PKRP, while for ThuRP they needed to overcome the learning curve. Thulium laser is suitable for resection, vaporization, and enucleation. Based on these characters, Xia designed a thulium laser procedure called “thulium laser resection of prostate-tangerine technique” (TmLRP-TT) 11 combined with resection and vaporization. Compared with HoLEP, this procedure shortens the operation time and improves laser efficiency with no need of morcellation. 29 For experienced urologists, although not significantly, the operation time of TmLRP-TT may be even shorter than standard TURP. 30 For patients with large prostates, PKRP was thought to be a better choice because the operation duration was significantly longer by ThuRP. 19 However, as technique developed, there was no significant difference in terms of operation time between PKRP and ThuRP for prostates larger than 80 mL (80–170 mL), as long as the surgeons were familiar with the new operation manner. 22 However, since available data about large prostates are still limited, more studies are needed to confirm the reliability of this result.
ThuRP was associated with less estimated blood loss and less drop in hemoglobin level due to its sufficient hemostasis, as our meta-analysis showed. Even though the difference may be of limited clinical significance and severe bleeding was not common in both PKRP and ThuRP, less bleeding intra- and postoperation is very important for the clear operation visibility and postoperative recovery. As we know, PKRP has a coagulation layer of 0.3–1.0 mm and significantly reduces the blood loss than TURP, which helps to provide a clear operation visibility. 6 However, ThuRP has the ability to provide a nearly bloodless procedure with a 0.5–2.0 mm coagulation band, and the operation visibility was described “surprisingly clear” by surgeons. 30 Better operation visibility leads to more precise cutting and shorter operation time. The postoperative recovery was also shorter in ThuRP than PKRP; like hospitalization, irrigation and catheterization duration was decreased. As the urine was back to clear quickly because of minimal bleeding, irrigation was not necessary and catheter could be removed on the second postoperative day. 9 In some countries like America, ThuRP can be even performed in outpatients. 25
The efficacy of the surgical treatment of BPH was evaluated by IPSS, QoL score, Qmax, and PVR; all these tests were assessed at least 1 month after operations. Our meta-analysis showed that there was no significant difference in terms of preoperative IPSS, QoL score, Qmax, and PVR between ThuRP and PKRP. The postoperative data showed that IPSS, QoL score, and PVR decreased and Qmax improved significantly, indicating that both ThuRP and PKRP had satisfied efficacy, and no significant difference was found between the two groups except QoL score, which was even better in the ThuRP group. Transurethral vaporization of prostate, including GreenLight and plasmakinetic energy, was considered to be associated with early irritative voiding symptoms, which usually manifest as frequency after the removal of catheter. The rate of irritative symptoms was about 11.4% in PKRP according to the published studies, 31 while no severe irritative symptoms were reported after ThuRP, which might reflect the difference in the evaluation of QoL score between the two groups. For large prostates (>80 mL) and elder patients (>70 years old), ThuRP also showed feasible efficiency and stability, based on 18 months of follow-up assessment. 32
We pooled the data about complications, including severe bleeding, temporary urinary retention, temporary urinary incontinence, urinary tract infection, and urethral stricture. There was no difference with regard to the occurrence of these complications between the two groups. The two techniques have some similar advantages based on their characteristics, for example, they are both performed in normal saline with no risk of TUR syndrome, and they both have precise cutting with minimal thermal injury, which can reduce urethral stricture formation. 19 Ejaculatory dysfunction is another common postoperative complication of BPH, and no case was reported in trials included in our meta-analysis. According to the conclusion of Giancarlo's study, the occurrence of ejaculatory dysfunction was considered to be similar between ThuRP, PKRP, and TURP. 33 The follow-up period of the trials included in the meta-analysis ranged from 1 to 18 months; long-term trial was absent, as thulium laser was newly introduced in urological surgery. Sun et al. published a long-term observation up to 8 years after ThuRP, concluding that ThuRP was a safe and effective procedure with excellent durability for the surgical treatment of BPH. 10 However, until now, long-term RCTs about ThuRP are still limited.
To our knowledge, this is the first meta-analysis comparing PKRP and ThuRP. Our study proved that ThuRP had sufficient efficacy and preferable ability of hemostasis and shorter recovery time. The sensitive analysis also reinforced the confidence of the results in our meta-analysis. However, we have to admit the certain limitations of our meta-analysis. First, all these included trials were all performed in China, except one in Korea. We only searched studies published in English and Chinese, some studies in other languages may have been missed. For different races and different skills or procedures of surgeons in other countries, the results may be different. Second, no long-term study was involved, and the follow-up duration was different in the included trials. We only pooled the postoperative data, but the parameters of efficacy may change as time goes on. Finally, the accuracy and stability of the results may be more or less influenced by the inherent heterogeneities for several continuous variabilities, which may result from many factors, and the potentially existing public bias that could not be completely excluded. Given those limitations, more worldwide, multicenter long-term RCTs are still required to establish the advantages of ThuRP.
Conclusion
Our meta-analysis demonstrated that both ThuRP and PKRP are safe and effective procedures for the surgical treatment of BPH. ThuRP is superior over PKRP concerning less blood loss and shorter recovery time like irrigation duration, catheterization time, and hospital stay. As a promising technique, more worldwide, multicenter long-term studies are still needed for the development and reference of ThuRP.
Footnotes
Acknowledgment
This study was funded by the National Natural Science Foundation of China (No.81170650 and NO.81370805). This article does not contain any studies with human participants or animals performed by any of the authors.
Disclosure Statement
No competing financial interests exist.