
Abstract
Abstract
Background and Aims:
Incisional hernia is a common complication of laparotomy. The long-term effectiveness of the laparoscopic repair compared to the open approach remains to be proven. We investigated the 1-year impact of open and laparoscopic repair of incisional hernia on quality of life outcomes.
Methods:
Single-center cohort study. The clinical data of patients who underwent open or laparoscopic surgery for primary midline incisional hernia were retrieved from hospital records and from a research database. Criteria of exclusion were emergency procedures, associated bowel resection, and recurrent incisional hernia. Complications and recurrence rates were analyzed. The visual analog scale (VAS) and the Short-Form 36 (SF-36) were used to assess pain and quality of life 1 year after surgery in patients free of recurrence.
Results:
One hundred twenty-four patients were eligible for inclusion in the study. The mean follow-up was 3 ± 2 years (interquartile range [IQR] 2.0). Overall, 9% of patients in the open group and 7% in the laparoscopic group presented with hernia recurrence (P = .685). Sixty-six of the 124 patients, who were operated between 2009 and 2014 by the same surgical team with expertise in advanced laparoscopic surgery, were considered for the study. Nine (14%) of these patients were lost to follow-up and three (5%) had a recurrent hernia, reducing the final sample size to 54 patients of whom 26 operated through an open approach and 28 through laparoscopy. The two groups were comparable according to demographic variables, comorbidity, and postoperative morbidity. The laparoscopic approach required less operative time (<.001) and length of hospital stay (P = .002). The VAS and the SF-36 scores were similar in the 54 patients, 26 in the open group and 28 in the laparoscopic group, who completed the 1-year assessment.
Conclusions:
Health-related quality of life at 1 year was similar in patients undergoing open or laparoscopic repair of incisional abdominal hernia.
Introduction
I
The widespread concept of tension-free repair of incisional hernia with mesh has resulted in a reduced recurrence rate compared with direct suture approximation. 6 The next significant change has been the minimally invasive laparoscopic approach. 7 From the early 1990s, several studies and reviews have compared the early results of the open and laparoscopic approach. Recently, a Cochrane collaboration report, including 10 RCTs and 880 patients with either primary ventral or incisional hernia, has confirmed the favorable early results of the laparoscopic technique, especially the reduced risk of wound infection, but there was a lack of long-term results in the studies analyzed. 8 Therefore, it is still debated whether the laparoscopic approach should be considered standard of care in the treatment of incisional hernia. In addition, only a few studies have reported the quality of life assessment as the primary outcome for their analysis.
The aim of this study was to compare safety, efficacy, and quality of life in a cohort of patients with incisional hernia repaired through an open or laparoscopic approach.
Materials and Methods
A single-center cohort study was performed to assess safety, efficacy, and impact on quality of life of open and laparoscopic repair of incisional abdominal wall hernia. To limit confounding factors, only patients who have been operated over the last 5 years for primary midline incisional hernia with either an open or a laparoscopic approach were considered for the study. Criteria of exclusion were the following: patients with a primary ventral hernia, patients with subxifoid, subcostal, sovrapubic, or parastomal defects, emergency procedures, associated bowel resection, and recurrent hernia. All patients were evaluated preoperatively by physical examination and abdominal wall ultrasound scan under Valsalva maneuver; in selected patients, especially those with severe obesity, basal CT scan or MR was also performed to obtain a more precise assessment of the abdominal defect and/or to rule out concomitant intra-abdominal disease. The surgical approach was decided preoperatively at the surgeon's discretion and taking into account the patient's wishes. Detailed informed consent was obtained from all the patients.
Demographic, clinical, and operative data were obtained from the hospital records and, more recently, from the research database. The variables included age, gender, body mass index (BMI), smoking, American Society of Anesthesiologist score, operative time, hospital length of stay, defect size, and mesh size. The mesh/defect ratio was also calculated for each patient to assess the relationship between the size of the implanted mesh and the original wall defect. Postoperative complications such as prolonged ileus, seroma, hematoma, infection requiring early or late mesh removal, hernia recurrence, and trocar site herniation were recorded.
Postoperative clinical evaluation, combined with the visual analog scale (VAS) self-assessment, was performed on day 1, day 30, and 1 year after surgery. The VAS score is a unidimensional measure of pain intensity ranging from 0 to 10 (0 no pain, 10 worst possible pain). 9 All patients with suspected hernia recurrence were evaluated with a confirmatory abdominal ultrasound scan.
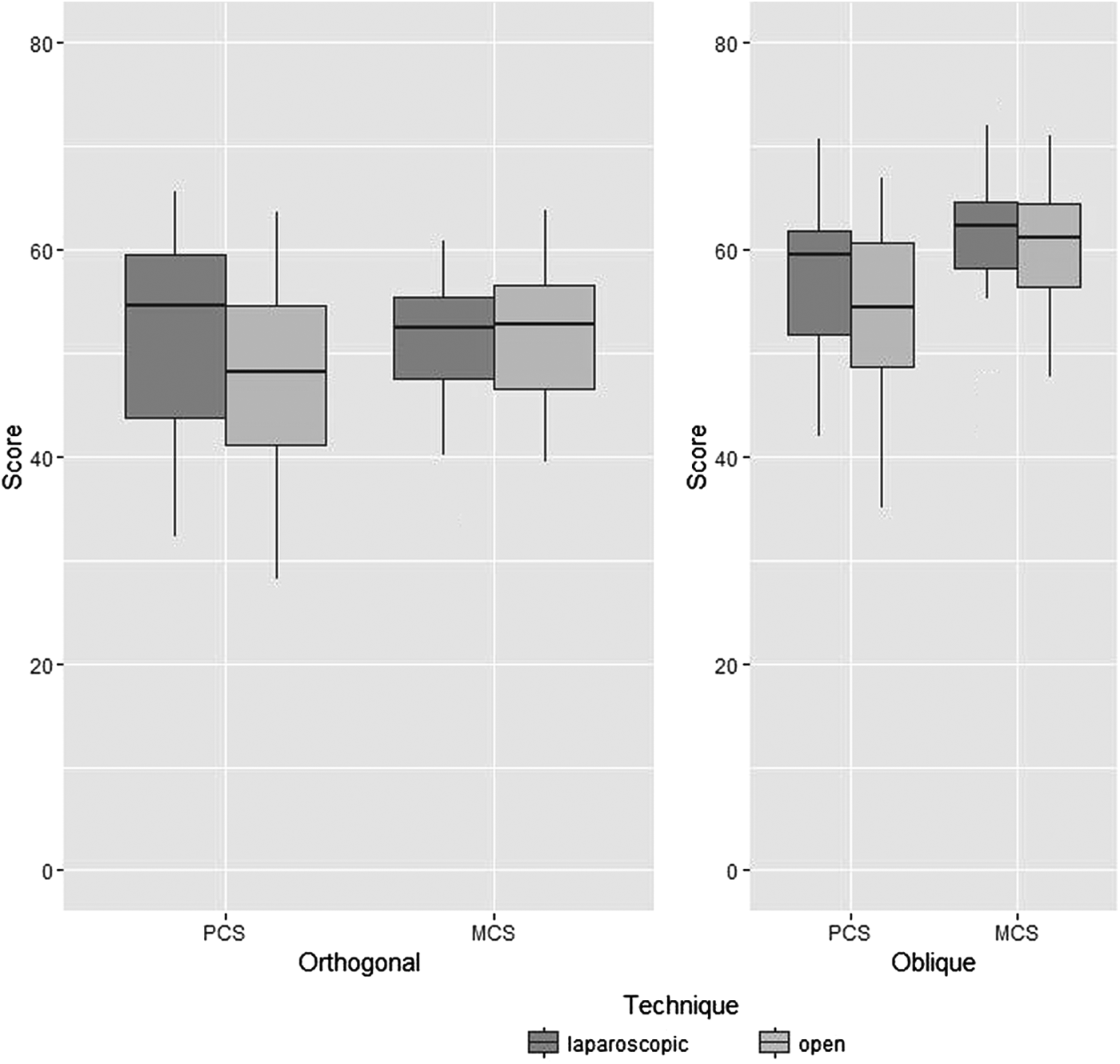
The Short-Form 36 (SF-36) survey was administered to patients who were willing to return to the outpatient clinic and were free of recurrence at 1 year. The SF-36 health survey is a multidimensional questionnaire composing 36 items to determine the health-related quality of life. 10 The SF-36 consists of eight different health quality domains: physical function (10 items), role limitations due to physical function role (4 items), bodily pain (2 items), general health (5 items), vitality (4 items), social function (2 items), role limitations due to emotional function (3 items), and mental health (5 items). The results from each scale vary from 0 to 100 (worst to best possible health status). In addition, the SF-36 physical component summary (PCS) and the mental component summary (MCS) scales were calculated, ranging from zero (lowest well-being) to 100 (highest well-being). SF-36 data were mapped to eight domain scores and showed in a standardized scale ranging from 0 to 100. The weights used to construct the summary scores MCS and PCS from SF-36 were derived from both orthogonal and oblique factor rotations. Orthogonal rotations identify factor weights that minimize the correlation between the PCS and MCS; oblique rotations allow the composite measures to be correlated.10,11
The primary outcome of the study was quality of life at 1 year; secondary outcomes were perioperative complications and recurrence rates.
Statistical analyses
Continuous and discrete variables are presented as median and interquartile range or mean and standard deviation, categorical variables with number and percentages. Chi square or Wilcoxon–Mann–Whitney for unpaired data tests were performed as appropriate. Two-sided P value and 95% confidence intervals (CIs) were computed. Type I error level at .05.
SF-36 scores were analyzed with nonparametric case resampling bootstrap linear regression, adjusted for centered age at intervention and BMI. Bootstrap P values, point estimation of regression parameters, and bias corrected accelerated CIs were computed with 3000 iterations. Double bootstrap and jackknife after bootstrap were used as diagnostics. 12
VAS score repeated measure data were analyzed with mean response profile method 13 through generalized estimating equations (GEE) using time as categorical variable, identity link function for linear predictor, sandwich estimator for standard errors, and unstructured working correlation matrix, selected by correlation information criterion. We tested the null hypothesis with multivariate Wald test as the equality of the difference of the mean between the two surgical techniques at each time point. In GEE regression, we adjusted for centered age at intervention and BMI. All analyses were carried out with R 3.2.2. 14
Surgical technique
The open surgical approach consisted of the Rives–Stoppa technique. The posterior rectus sheath was repaired with a polydioxanone (PDS) or a Maxon loop running suture. The size of the defect was measured intraoperatively, and the mesh was placed in the retromuscular space. The most used type of mesh was polypropylene (Angimesh®; Angiologica Pavia). The mesh was tailored with an overlap of 5 cm and fixed with nonresorbable stitches using the Reverdin needle. The anterior rectus sheath was closed with interrupted Vicryl sutures, and an interfascial suction drain was routinely placed.
The laparoscopic approach was performed using three trocars. The pneumoperitoneum was induced with a Veress needle usually inserted in the left subcostal area. After insertion of the first optical trocar, the abdominal wall was inspected and attention was paid to identify potentially misdiagnosed defects. Adhesiolysis was performed with limited or no use of cautery. By reducing the pneumoperitoneum pressure to 8 mmHg, the defect size was measured. A mesh overlap of 5 cm for each side of the defect was calculated. The most used type of mesh was Parietex™ Composite (Covidien) and Proceed® (Ethicon, Inc.). The mesh was suspended to the abdominal wall with four stitches and then fixed with not absorbable tacks in a double crown configuration.
Results
Between September 2001 and December 2014, 322 consecutive patients underwent primary or incisional abdominal hernia repair with an open or laparoscopic approach. One hundred ninety-eight patients did not meet the criteria of inclusion in the study, leaving a total of 124 patients. The mean follow-up was 3 ± 2 years (IQR 2.0). Overall, 9% of patients in the open group and 7% in the laparoscopic group presented with hernia recurrence (P = .685). Sixty-six of the 124 patients who were operated between 2009 and 2014 by the same surgical team with expertise in advanced laparoscopic surgery were considered for the study. Nine (14%) of these patients were lost to follow-up and 3 (5%) presented with recurrent hernia, reducing the final sample size to 54 patients, 26 of whom operated through an open approach and 28 through laparoscopy.
Patients in the two groups were comparable for demographic variables, comorbidity, and postoperative morbidity. There were no statistically significant differences in terms of defect size and mesh size between the two groups. Instead, the mesh/defect ratio was almost double in the laparoscopic group (8.3 vs. 4.0, P = .0026). The laparoscopic approach required less operative time (<.001) and length of hospital stay (P = .0019; Table 1).
ASA, American Society of Anesthesiologist; BMI, body mass index; IQR, interquartile range; VLS, videolaparoscopy.
Fifty-four patients with a minimum 1-year follow-up returned to the outpatient clinic for reassessment and both VAS and SF-36 scores were obtained. The main characteristics of this group of patients are summarized in Table 2.
BMI, body mass index; IQR, interquartile range; VLS, videolaparoscopy.
Descriptive statistics for SF-36 domain scores and MCS and PCS summary scores are reported in Figures 1 and 2, respectively. Raw analysis and bootstrap adjusted analysis (Fig. 3) showed that the means of SF-36 domain and MCS and PCS summary scores, did not significantly differ between the two groups at 1 year follow-up (Tables 3 and 4). Figure 4 shows the two-dimensional profile of the SF-36 scores.

Box plot for SF-36 domain scores by surgical technique.
Box plot of PCS and MCS by surgical procedure and by factor rotation. MCS, mental component summary; PCS, physical component summary.
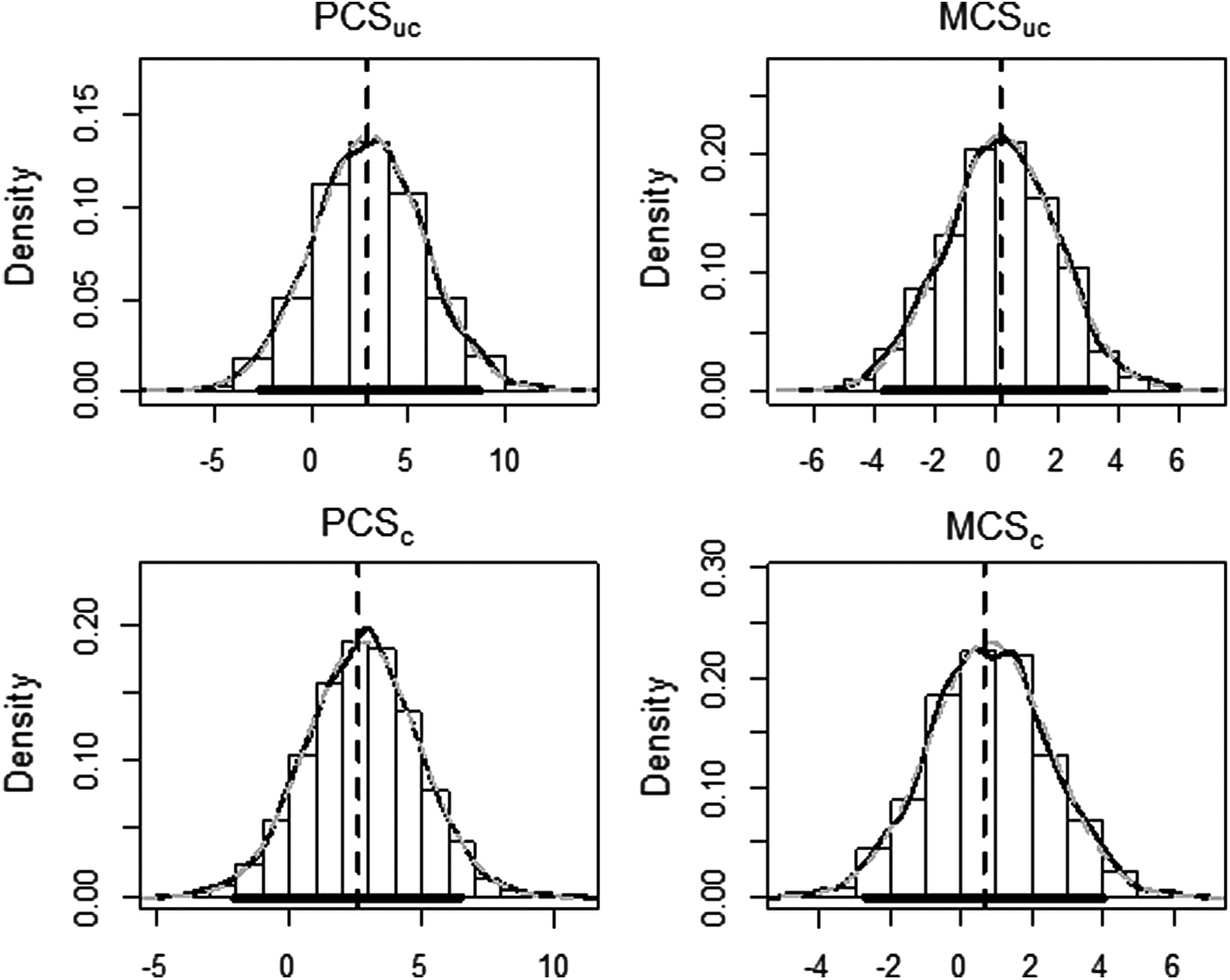
Distribution of the bootstrapped regression surgical technique coefficients: in solid black line the kernel density estimated, in gray dashed line fitted normal density. The thick black line on x-axis represents the estimated 95% BCa CI. BCa, bias corrected accelerated; CI, confidence interval.
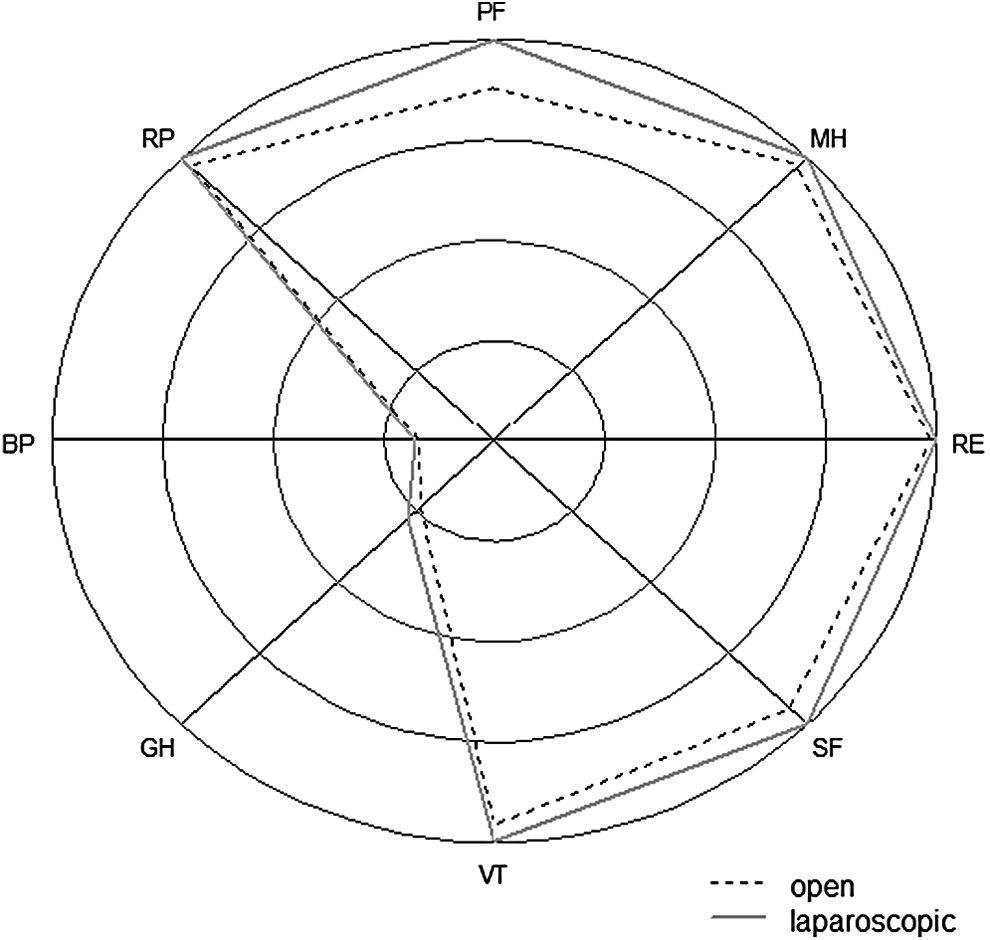
Radar plot for SF-36 domain scores by surgical technique.
IQR, interquartile range; MCS, mental component summary; PCS, physical component summary; SF-36, Short-Form 36.
Boot bias indicates the difference between the average bootstrapped value of the mean and its original sample value.
BCa, bias corrected accelerated; CI, confidence interval; MCS, mental component summary; PCS, physical component summary; SF-36, Short-Form 36; VLS, videolaparoscopy.
The GEE analysis indicates that the two groups have parallel mean response profiles and then the patterns of VAS change over time did not differ in the two groups (P = .41; Table 5). Furthermore, the GEE analysis showed that the mean VAS score decreased over time in both groups (P < .001) and that the VAS score did not differ in the two groups at postoperative day 1 (P = .13). One year after surgery, the mean VAS score reached ∼0 (Fig. 5).
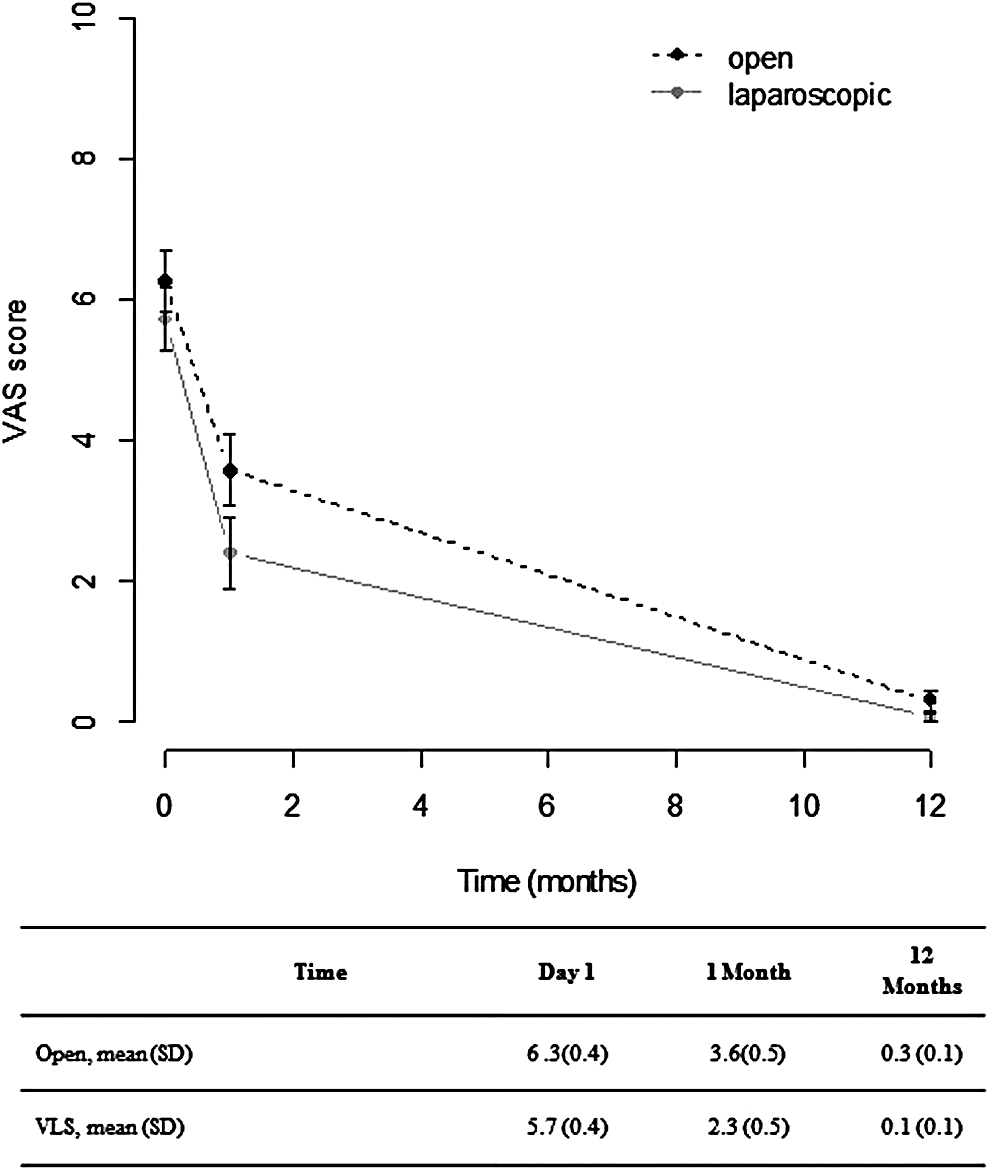
Mean VAS scores and relative standard error on postoperative day 1, day 30, and 1 year after surgery. VAS, visual analog scale; VLS, videolaparoscopy.
BMI, body mass index; GEE, generalized estimating equation.
Discussion
The results of this study confirm that open and laparoscopic repair of abdominal wall incisional hernia are comparable in terms of safety and that there was no statistically significant difference in the recurrence rate at 1 year. Interestingly, the quality of life scores at 1 year were similar in the two groups. As recurrence rates have decreased after both open and laparoscopic repair of incisional hernia, the issue of quality of life has become an important indicator of outcome. A matched-pair analysis by Mussack et al. 15 compared SF-36 scores in 24 patients who underwent laparoscopic incisional hernia repair with 24 patients who underwent an open approach. After a mean follow-up of 16 and 28 months, respectively, none of the SF-36 Health Survey domains and summary scores revealed significant differences between the two surgical techniques. Hope et al. 16 compared quality of life outcomes using the SF-36 survey and the Carolinas Comfort Scale in 56 patients operated for ventral hernia repair, 41 by laparoscopy and 15 by open technique, and reported an advantage of the laparoscopic approach at 6-month follow-up. In contrast, Colavita et al. 17 examined a large international database, including 710 ventral hernia repairs, and found that there was no difference in quality of life assessed by the Carolinas Comfort Scale at 12-month follow-up. Our study differs from the previous because only primary midline incisional hernia patients were included to avoid confounding due to the mixture of patients with primary ventral hernia and incisional or recurrent hernia. We also excluded from the present study patients operated on an emergency setting and those who underwent bowel resection. We found that the health-related quality of life using VAS, SF-36, MPS, and PCS as outcome measures was similar in the two patient groups. A recent randomized clinical trial has confirmed that patients with incisional hernia benefit substantially from surgery in regard to quality of life, independent of the surgical approach, and that the SF-36 is a useful instrument for the follow-up of these patients. 18
A limitation of our study is that we did not collect the SF-36 surveys preoperatively. Another limitation is that, considering the observational nature of the study, postoperative quality of life may have been affected by unmeasured or unmeasurable confounding factors. In addition, we could not control for type II error and the sample size was too small to yield narrower CIs for more precise estimations.
We conclude that the 1-year outcome of patients with incisional hernia operated either through a open or laparoscopic approach is similar in terms of early complications, recurrence rate, and quality of life. However, in our opinion, the laparoscopic repair should remain the approach of choice in obese patients and in those who have failed prior open repairs.
Footnotes
Disclosure Statement
No competing financial interests exist.