
Abstract
Abstract
Introduction:
Endoscopic techniques are rapidly gaining interest in esophageal cancer surgery due to lower pulmonary complication rates and faster postoperative recovery. Conventional two-dimensional endoscopic surgery has two main limitations: lack of depth perception and limited dexterity due to the use of rigid instruments. Theoretically, three-dimensional (3D) endoscopy can overcome these limitations, but to date, its use has not been reported in the context of esophageal cancer surgery. We studied our first series of 3D thoracolaparoscopic esophagectomies to document the safety and feasibility of implementing this technique.
Methods:
Patients who underwent a thoracolaparoscopic esophagectomy using a glasses-based 3D system with a 100° angulating camera tip were included. Continuity of the digestive tract was restored with gastric tube reconstruction and a cervical anastomosis.
Results:
All 13 resections were completed thoracolaparoscopically. Median duration of surgery was 360 minutes (range: 245–590 minutes), and median blood loss was 170 mL (range: 50–230 mL). A median of 20 lymph nodes was resected, and all resections were microscopically radical. Median hospital stay was 9 days. Two patients developed pneumonia (15%), and three patients experienced an anastomotic leakage (23%). All postoperative complications were managed on the ward.
Conclusion:
In this series, the newest generation glasses-based 3D systems proved safe and useful for the thoracolaparoscopic resection of esophageal cancer. Besides better visualization, dexterity seemed to be improved using the 100° flexible 3D camera. Implementation was without significant problems, and the first results are promising.
Introduction
C
The use of the first-generation 3D systems, developed to restore the surgeon's natural sight, was limited because surgeons experienced visual discomfort, fatigue, and headache due to stereopsis.9,11 In addition, the viewing conditions were suboptimal due to low-quality monitors and incongruent stereoscopic imaging. 11 Robot-assisted surgery, developed to overcome these shortcomings, is, however, associated with substantially higher costs.12,13 The latest generation glasses-based 3D systems with a 100° angulating camera tip theoretically fill the gap between conventional two-dimensional (2D) endoscopy and 3D robotic surgery. 14
Restoring depth perception and spatial orientation allows more precise and faster dissection, even in narrow operating spaces.9,14,15 Therefore, this technique may be of additional value in complex procedures as an esophagectomy. To date, the use of 3D thoracolaparoscopy has not been reported in the context of esophageal cancer surgery.
In this study, we describe our first series of 3D thoracolaparoscopic esophagectomies with the aim to document the safety and feasibility of implementing this technique into current practice.
Materials and Methods
Patients
From May to October 2014, a 3D glasses-based video system was available in our institute for a 6-month test period. The video system was implemented in the operating theater in June 2015. Patients who underwent a 3D thoracolaparoscopic esophagectomy during either the 6-month test period or the 6-month period after implementation were included in this study. During the test period, the availability of the 3D video system determined whether a routine 2D or a 3D procedure was performed.
The standard preoperative diagnostic workup consisted of an esophagogastroduodenoscopy with biopsy, endoscopic ultrasonography, a computed tomography (CT) of the thorax and abdomen, and 18F-fluorodeoxyglucose Positron Emission Tomography/CT scan.
Neoadjuvant treatment consisted of chemoradiotherapy according to the CROSS regimen, that is, weekly carboplatin and paclitaxel for 5 weeks with concurrent radiotherapy (41.4–50.4 Gy). 16 Surgery was planned 6–8 weeks after chemoradiation if no signs of distant metastases were seen after evaluation with a PET/CT.
3D imaging during surgery
For 3D vision, a 10-mm 3D endoscope with two optical channels and articulating camera tip with 100° of freedom was used. The 3D images were displayed on two high-definition 26-inch LCD monitors. The surgeons and scrub nurse wore lightweight glasses for perceiving a 3D image. A separate 2D monitor provided views for the nonoperating members of the personnel.
Operative technique
All procedures were performed by two surgeons (J.v.S. and K.H.). Patient positioning and surgical preparation did not differ from the standard 2D thoracolaparoscopic procedure. Surgery was performed under combined general and thoracic epidural anesthesia. All patients received antibiotic prophylaxis, a nasogastric tube, and a central venous catheter. Intubation was performed with a standard single-lumen endotracheal tube.
Patients were placed in a prone position with both arms forward. Hips and shoulders were supported by padded cushions. The head was placed in a ProneView mask facing downward in a mirror, providing sight of the endotracheal tube and leaving the eyes and nose free. Both surgeons were standing on the right side of the patient during the thoracic phase (Fig. 1) and in French position during the abdominal phase (Fig. 2) of the procedure. The scrub nurse stood on the left side. The two monitors were positioned next to the left shoulder of the scrub nurse and next to the right surgeon (thoracic phase)/above the head of the patient (abdominal phase).
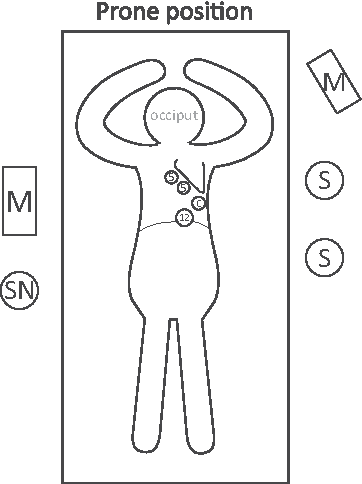
Thoracic phase: 5, 5-mm trocar; 12, 12-mm trocar. C, camera; M, monitor; S, surgeon; SN, scrub nurse.
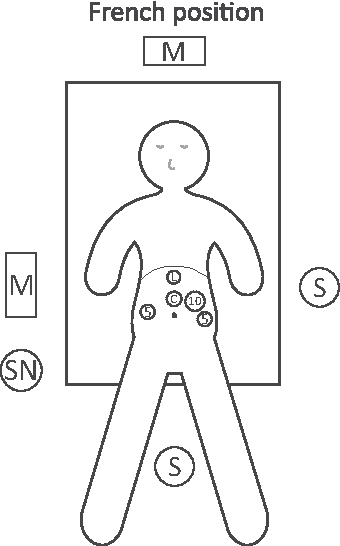
Abdominal phase: 5, 5-mm trocar; 10, 10-mm trocar; C, camera; L, port for liver retractor; M, monitor; S, surgeon; SN, scrub nurse.
Thoracoscopy was performed using four trocar ports placed in the right hemithorax: a 10-mm camera port placed at the seventh or eighth intercostal space, a 12-mm port placed at the ninth intercostal space (paravertebral), and two 5-mm ports placed at the third or fourth and fifth or sixth intercostal space. Tidal volumes were limited to 300–350 mL maintaining two-lung ventilation. An intrathoracic insufflation pressure of max 8 mmHg was retained. Dissection of the esophagus and lymph node stations did not differ from the standard 2D technique. First, the pulmonary ligament was divided, and dissection was continued cranially up to the level of the carina. After dividing the azygos vein, the thoracic esophagus was mobilized in the full length with periesophageal fatty tissue and en bloc subcarinal, right paratracheal, and paraesophageal lymph nodes. After insertion of a chest drain, the thorax was closed, and the patient was tilted in French position.
Laparoscopy was performed using four trocar ports between the umbilicus and xyphoid: a 10-mm camera port was placed supraumbilically, 5- and 10-mm ports were placed in the left hemiabdomen, and a 5-mm trocar was inserted in the right hemiabdomen. If no omni-tract device was used, a fifth trocar was inserted in the right hemiabdomen for liver-holding purposes. A pneumoperitoneum was created with a maximum insufflation pressure of 15 mmHg. To mobilize the stomach, the lesser and subsequently the greater curvature were dissected up until the level of the right and left diaphragmatic crus. A lymphadenectomy around the celiac trunk was performed, and the left gastric artery and vein were sealed. The esophagus was further mobilized from the crus by opening the hiatus. Then, via a cervical incision on the ventral border of the left sternocleidomastoid muscle, the cervical esophagus was mobilized and truncated.
The specimen was extracted via a supraumbilical minilaparotomy (6–8 cm) in the midline using a wound protector. Outside the abdomen, a gastric tube was made using a 55-mm stapler and, after suturing the stapled line, pulled to the neck through the mediastinum. A cervical end-to-side anastomosis was hand-sutured with PDS3/0 and via the minilaparotomy a jejunostomy was placed for postoperative feeding.
Data collection and statistical analysis
All patient data concerning baseline characteristics, neoadjuvant treatment, surgical details, complications, hospital admission, and histopathology were prospectively collected and analyzed using SPSS (version 22.0 for Windows). Data of patients who underwent a 2D thoracolaparoscopic esophagectomy in the same period were also collected.
Results
During the two 6-month periods, 13 patients underwent a 3D thoracolaparoscopic esophagectomy for esophageal cancer. All had received neoadjuvant chemoradiotherapy: one patient received 50.4 Gy and all others 41.4 Gy. Patient and tumor characteristics are presented in Tables 1 and 2, respectively.
Ten pack-years or more.
ASA, American Society of Anesthesiology; BMI, body mass index; 2D, two-dimensional; 3D, three-dimensional.
TNM, tumor node metastasis stage according to seventh edition TNM classification.
AC, adenocarcinoma; SCC, squamous cell carcinoma; 2D, two-dimensional; 3D, three-dimensional.
The median duration of surgery was 360 minutes (range: 245–590 minutes), none of the procedures needed to be converted (Table 3). Median blood loss was 170 mL (range: 50–230 mL). All resection margins were free of tumor, and a median of 20 lymph nodes was resected. Patient and tumor characteristics did not differ between patients who underwent a 3D or 2D esophagectomy (Tables 1 and 2).
R0: tumor-free resection margins.
ICU, intensive care unit; 2D, two-dimensional; 3D, three-dimensional.
All postoperative complications are listed in Table 3. Two patients developed pneumonia; both were managed on the ward with antibiotics. Anastomotic leakage was seen in three patients; all recovered after dietary restrictions (nil per os) without surgical intervention. One patient (American Society of Anesthesiology [ASA] 3, body mass index: 16.6) was admitted for 29 days because of pneumonia, anastomotic leakage, and atrial fibrillation from which she successfully recovered. Patient outcome and length of hospital stay (median: 9 days) of all other patients were not affected by postoperative complications. There was no postoperative mortality.
No difficulties were encountered during implementation of the 3D system into the surgical procedure. No adjustments were made to the surgical protocol for thoracolaparoscopic esophagectomies besides a 2- to 3-cm lower placement of the camera port. None of the personnel involved in the surgical procedure (surgeons and scrub nurse) experienced visual discomfort, nausea, dizziness, headache, blurry sight, or fatigue.
Discussion
The safety and feasibility of conventional 2D thoracolaparoscopic surgery for esophageal cancer have been reported in several studies.4,17–19 Evidence has been provided for short-term benefits, that is, shorter hospital stay, less blood loss, and lower pulmonary complication rates, without compromising the quality of the resected specimen. 3 Limitations of conventional endoscopy, however, are the lack of a three-dimensional (3D) view, which disables the surgeons' depth perception and complicates orientation, and the limited degrees of freedom due to the 30° camera, which impairs the surgeons' dexterity.7–10 These limitations are most prominent in deep narrow spaces so, theoretically, in the thoracic phase of an esophagectomy. 20
For other surgical procedures, the value of 3D vision has been frequently described.9,14,21,22 The addition of the third dimension in endoscopy entails a natural view on the operating field, which facilitates orientation in space and identification of dissection planes. In addition, the flexible camera tip of the new-generation 3D systems contributes to a more intuitive way of tissue preparation by allowing a broader range of motion of up to 100° instead of the conventional 30°.
Early generation 3D systems failed to overcome the visual side effects of stereopsis (each eye receiving different projections): eye strain, blurry sight, headache, and fatigue. In addition, projecting a good-quality stereoscopic image onto screen was a challenge.9,11,21,23 Robotic surgery is able to surmount these obstacles, but large-scale use is hindered by high costs.13,24 The new-generation glasses-based 3D systems are able to overcome the limitations of earlier 3D and 2D endoscopic surgery. In addition, these new systems are less expensive than robotic surgery. 14 For surgeons, the transition from 2D to 3D laparoscopy is rapid.9,15,21,25
There are no randomized studies comparing 3D with 2D esophageal cancer surgery. This study describes our first series of patients treated with 3D thoracolaparoscopic esophagectomies. Both clinical and pathological short-term outcomes of our study population were good and comparable to patients operated using a 2D endoscope. Traditionally, pneumonia is the most common complication after an esophagectomy. 26 Prolonged duration of surgery is known to be associated with pulmonary complications. 27 In our study, the duration of surgery was slightly longer than in other minimally invasive esophagectomy studies (median: 360 minutes versus 330 minutes).3,28 The incidence of postoperative pneumonia (15%), however, was comparable with previously published prospective series (7.7%–30%).3,5,28 The median hospital stay (9 days) was also similar to other reported data (10–11 days).28–30 Measures to prevent postoperative morbidity in thoracolaparoscopic esophageal surgery are similar in 2D and 3D surgery. During surgery, these measures include restrictive fluid administration, prone positioning, and lung-protective small tidal volume two-lung ventilation. Other important measures irrespective of the surgical approach of an esophagectomy are intra- and postoperative thoracic epidural analgesia, as well as postoperative early detubation (usually in the operating room), early mobilization, and daily physiotherapy.31,32
In this report, we describe our first experience with 3D thoracolaparoscopic esophagectomies in a small number of patients. No conclusions should be drawn with regard to the superiority of 3D over 2D vision in esophageal cancer surgery because of the nonrandomized setting and the small number of patients. In our experience, the additional value of 3D endoscopy lies in its ability to enable an intuitive and dexterity-improving way of working using a flexible camera in combination with comfortable viewing conditions (i.e., natural view and sharpness of monitors). Supported by the results, we conclude that 3D vision can be safely integrated in conventional—2D—esophageal cancer surgery without adjusting current surgical protocols. It is unlikely that prospective studies comparing 2D with 3D procedures will take place. Theoretically, only visual and dexterity-improving features are added to an already existing technique.
Conclusion
The use of the newest generation glasses-based 3D systems proved useful in this series. Besides better visualization, dexterity seemed to be improved using the newest generation glasses-based 3D systems with a flexible camera. Implementation was without significant problems, and the first results are promising.
Footnotes
Acknowledgments
The authors thank Karen Vork and Hanneke van den Bosch for facilitating the implementation of 3D thoracolaparoscopy in the operation theater. This research was funded by Stichting Cornelis Vrolijk Development Fund.
Disclosure Statement
No competing financial interests exist.