
Abstract
Abstract
Background:
Laparoscopic surgery is considered the standard approach for the treatment of paraesophageal hernias (PEHs). Despite its advantages, this approach is technically demanding with a significant learning curve. Data about the safety and utility of the robotically assisted paraesophageal hernia repair (RA-PEHR) are scarce. The aim of this study is to assess the feasibility and safety of robotic assistance for the treatment of PEH.
Materials and Methods:
Between June 2010 and December 2015, patients who underwent elective RA-PEHR were included in a prospectively collected database. Demographic data, American Society of Anesthesiologists (ASA) classification, preoperative testing, operative time (OT), length of hospital stay (LOS), conversion rate, morbidity, and mortality were recorded and reviewed retrospectively.
Results:
Sixty-one patients underwent RA-PEHR with mesh, 72% were female (mean age of 63 and mean body mass index [BMI] of 30). ASA classification was 2.6 (57% of patients had an ASA III). With respect to the type of the hernia, the preoperative diagnosis was: Type II 26%, III 64%, and IV 13%. OT averaged 186 minutes (88–360), including robot setup time. After the 16th case, OT significantly decreased by 4.09 minutes (P = .01). There were no conversions. The average blood loss was 51 mL. Perioperative complications, including intraoperative and 30-day complications, were 6% and 23%, respectively. The mean length of hospitalization was 2.6 (1–18) days. There were no deaths. Forty patients (66%) were available for follow-up, and length of follow-up was 17 ± 15 months. Anatomic recurrence was observed in 42% of patients and only 23% of patients were symptomatic.
Conclusions:
This report represents the largest series to date of RA-PEHR. RA-PEHR has proved to be feasible and safe with a learning curve comparable to the standard laparoscopic approach.
Introduction
F
There is consensus today that laparoscopic surgery is the mainstay of surgical treatments. The use of this approach has rapidly spread, due to the decreased morbidity and mortality compared to the open approach. Numerous series have demonstrated the safety profile of the surgery.5–8 Despite the encouraging low morbidity and mortality rates, the reported rates of recurrence remained high at 12%–54%. 9 Most studies have noted that PEH repair is a technically demanding operation with a significant learning curve.10,11 Patient factors, the complexity of the disease process, and the high technical demands of the surgery play a significant role in the learning curve and may influence the long term durability of the repair.9,12
Of all the heated controversies surrounding the current treatment of PEH, robotic surgery is perhaps an uncommon topic of debate. Robotic surgery is a proliferating technology in general surgery, although there is a paucity of data concerning benefits of robotics for the treatment of PEH. The aim of this study is to demonstrate the feasibility and safety of the robotically assisted paraesophageal hernia repair (RA-PEHR) with mesh and the value of its addition to the surgical armamentarium.
Materials and Methods
A retrospective review was performed of all the patients who underwent elective RA-PEHR between June 2010 and December 2015.
Demographic data, American Society of Anesthesiologists (ASA) classification, preoperative testing, operative time (OT), length of hospital stay (LOS), conversion rate, estimated blood loss (EBL), morbidity, mortality, and length of follow-up were recorded. To assess the learning curve, two types of variables were evaluated: operative and patient outcomes (OT, EBL, intraoperative complications (IC), and 30-day complications).
Preoperative evaluation
The preoperative workup included a barium esophagogram to clarify the anatomy, esophagogastroduodenoscopy, and for most of the patients a high-resolution esophageal manometry. Esophageal pH monitoring was only performed if patients had disabling reflux symptoms.
Operative technique
Patients were advised to ingest only clear liquids 2 or 3 days before surgery to decrease the risk of aspiration during induction of anesthesia. Operations were performed by a fellowship trained minimally invasive surgeon (C.A.G.) using the da Vinci Surgical System™ (Intuitive Surgical).
Description of the technique
After satisfactory induction of general endotracheal anesthesia, the patient is placed in the semilithotomy position over a “bean bag.” Pneumatic compression stockings are placed on both legs routinely, and the legs are placed in split-leg attachments (Fig. 1a). An orogastric tube is placed to decompress the esophagus and stomach. Preoperative antibiotics are given. A 12-mm trocar is initially placed, under direct vision using an optical trocar system, in the left mid-abdomen two fingerbreadths lateral to the umbilicus and one palm-width inferior to the left costal margin. This port is used for the robotic camera. Three 8-mm trocars are then placed: one on the left subcostal midclavicular line (Arm #1), one on the right subcostal midclavicular line (Arm #2), and one in the left flank (Arm #3) (Fig. 2). A 5-mm subxiphoid incision is used for the placement of the Nathanson liver retractor. An assistant port (10 mm) is inserted in the left anterior axillary line, 2 cm below the costal margin (Fig. 1b). At this point, the robotic surgical cart was approximated into position and the arms are attached to the three specific trocars. A Cadiere Forceps is placed in the surgeon's left hand (Arm #2) and in Arm #3, and in the right hand, the articulated robotic vessel sealer device is introduced (Arm #1) (Fig. 2). The assistant at the bedside usually performs the setup of the robot. The assistant surgeon is positioned on the patients' left side. During the case, the assistant is in charge of cutting, suction, and retraction, and if needed, switches the robotic instruments for the operating surgeon. For this reason, basic training in laparoscopic surgery and robotics is essential for the assistant surgeon.
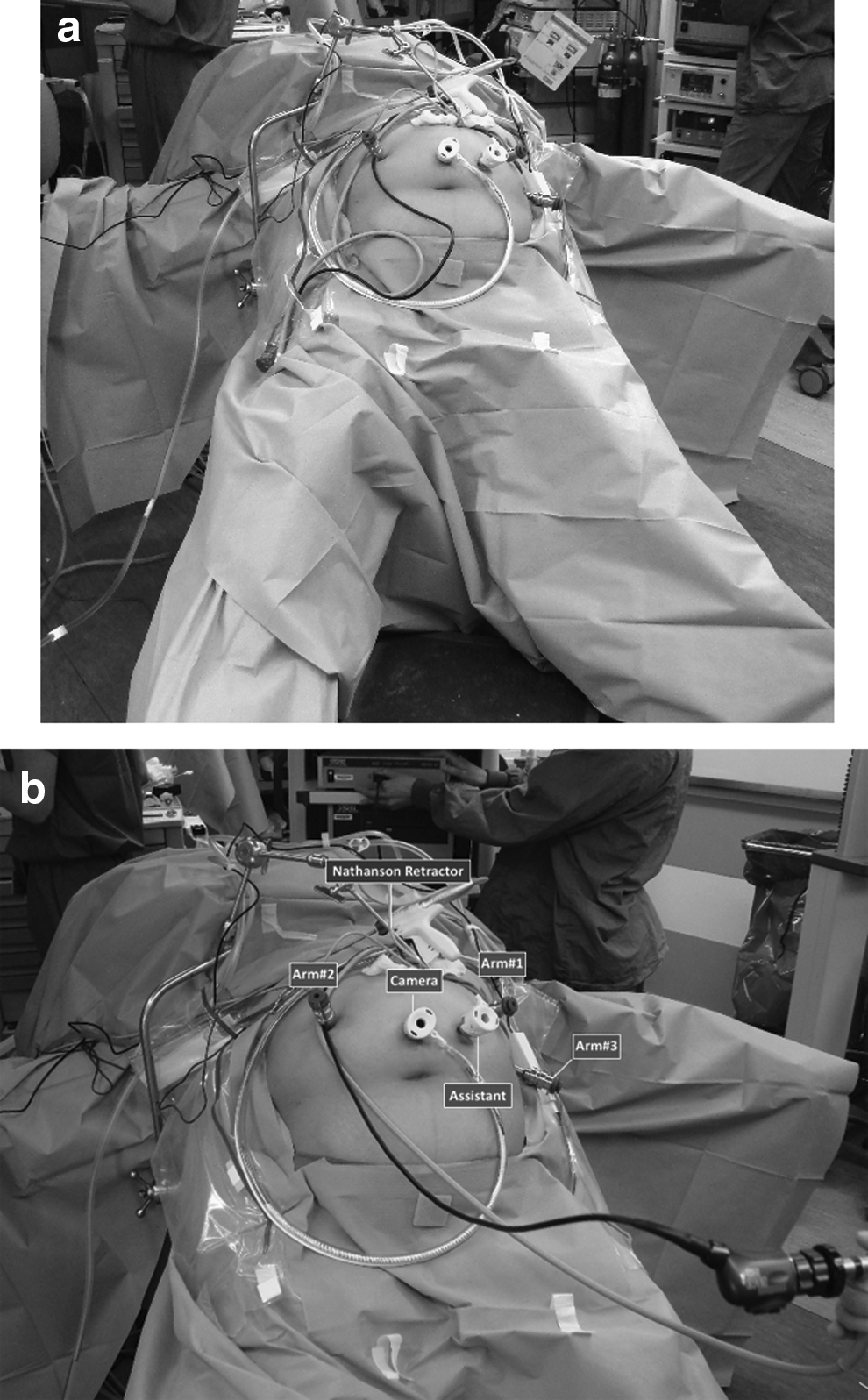

The robotic cart is brought into the operating theater over the patient's head and attached to the specific trocars.
Several surgical principles are observed when performing these repairs to minimize complications and optimize outcomes as follows:
Reduction of the hernia and dissection of the sac
The left crura approach is routinely used. After the left lobe of the liver is retracted anteriorly using the Nathanson retractor, the hiatus is exposed. At this point, the hernia is visualized. As a first step of the operation, the herniated stomach is gently reduced, and early division of the short gastric vessels using the robotic vessel sealer is performed. Incision of the hernia sac is started at its junction with the left crura and continued in a circular manner around the rim of the hiatus. Next, using a combination of blunt dissection and Harmonic scalpel, the hernia sac is dissected off its mediastinal attachments, reduced into the abdomen, and left at the gastroesophageal (GE) junction level. Resection of the sac is performed as much as possible while avoiding injury to the anterior vagus nerve. Full mobilization of the fundus is carried out by dividing posterior adhesions to the anterior capsule of the pancreas. Once the left crus is exposed and the greater curvature of the stomach is completely free, the dissection is extended to the right side of the esophagus. The gastrohepatic ligament is opened, and the right crus is separated from the esophagus with a combination of blunt dissection and robotic vessel sealer. A retroesophageal window is created and a Penrose drain passed and clipped anteriorly. The vagus nerves are enclosed within the Penrose drain. The drain is used to encircle the esophagus for further manipulation as the dissection continues into the posterior mediastinum.
Esophageal mobilization
Transhiatal dissection of the esophagus is started and continued in a cephalad direction. The articulated vessel sealer device and the Cadiere forceps are used for the circumferential dissection of the esophagus. Soft tissue attachments are divided bluntly as the dissection continues into the posterior mediastinum. Esophageal mobilization is completed only after the GE junction is observed to be well into the abdomen without tension.
Crura closure
The esophagus is retracted ventrally and to the left by Arm #3. Closure of the diaphragmatic defect is started at the junction of the right and left crus to decrease tension on every stitch, and is carried out cephalad. The closure is performed using interrupted 0 silk stitches with intracorporeal knot-tying technique. A 56 Fr bougie is passed down the esophagus during the repair to tailor the closure and to avoid postoperative dysphagia. Furthermore, a U-shaped GORE® BIO-A® was used to reinforce the closure of the diaphragmatic defect. The mesh is secured in place to the edge of the right and left crura and at the bottom of the repair with nonabsorbable interrupted stitches.
Antireflux procedure
The construction of a floppy tension-free fundoplication is gauged over a 56 Fr bougie. Three 2-0 silk stitches are used to create the wrap, and the most distal stitch is used to attach the wrap to the esophagus. Upper endoscopy is routinely performed at the completion of the case to check the indemnity of the esophagus, stomach, and the adequacy and patency of the fundoplication.
Follow-up
Patients were seen in follow-up 2 weeks after surgery and every 3 months for the first year. At the 1-year follow-up, patients were asked to undergo a barium swallow to rule out recurrence. After this, patients were seen at regular 6-month intervals or they were followed by a telephone interview performed by a nurse practitioner or a fellow. During each follow-up visit, a detailed symptomatic evaluation was performed on all patients. Beyond this time, barium swallow, upper endoscopy, or esophageal function tests were ordered on an as-needed basis. Patients with less than 3 months follow-up were excluded from the analysis.
Statistical analysis
The data were analyzed using R package (R Core Team, Vienna, Austria). Results are expressed as mean and standard deviation for quantitative variables and ratios and percentages for qualitative variables. The level of statistical significance was set at 0.05. Logistic and nonparametric regression was performed to explore the relationship between each of the perioperative outcomes and the number of cases. An empirical fluctuation process based on cumulative sums of ordinary least square residuals was performed to identify the potential change points. The number of change points was determined by Bayesian Information Criteria. The change point analysis was performed using R package “strucchange.” Once the change point was identified, piecewise linear regression was performed to evaluate the relationship between each outcome and the number of cases before and after the change point while controlling for patient's characteristics (e.g., age, gender, body mass index [BMI], and ASA). Before fitting the piecewise linear regression model, data were transformed if necessary.
Results
A total of 61 consecutive patients underwent RA-PEHR at University of Arizona, Tucson. Of these, 44 (72%) patients were female, and the mean age was 63 (36–91) years. The average BMI was 30 (17–49), with 39% of patients considered obese and 18% morbidly obese. Patient demographics are listed in Table 1.
ASA, American Society of Anesthesiologists; BMI, body mass index.
Preoperative diagnoses were as follows: Type II 26%, Type III 64%, and Type IV 13%. The ASA classification was 2.6 (57% of patients had an ASA III).
Operative and postoperative course
The operation was completed with robotic assistance in all patients. Perioperative data are listed in Table 1. Primary repair was performed in 55 (90%) patients and 6 (10%) patients had a redo hiatal hernia repair. Resection of the hernia sac was performed in all patients. The crural repair was primary with mesh reinforcement in all patients. A Nissen fundoplication was performed in 57 (93%) patients, a Toupet fundoplication in one patient (2%), and Roux-en-Y gastric bypass was performed in three patients (5%) due to associated morbid obesity.
Overall, OT was 186 (88–360) minutes, including robotic setup time (i.e., draping of the arms of the robot, surgical cart positioning, and instrument setup). Logistic and nonparametric regression showed that there was a change point for each of the three variables analyzed (i.e., OT, EBL, and LOS). Specifically, OT displayed change points corresponding to the 16th, 22nd, and 30th cases. Based on the change point at the 16th case, the OT significantly decreased by 4.09 (P = .01) with every additional case after adjusting for patient's characteristics (BMI, age, gender, and ASA) (Fig. 3). Similarly, EBL showed a single change point at 16th case and after adjusting for BMI, age, gender, and ASA, there was a significant decrease of 8.46 (P < .0001) with every additional case (Fig. 4). A single change point in length of hospital stay was identified at the 22nd case, and after adjusting for BMI, age, gender, and ASA, the length of hospital stay significantly decreased (P = .02) with every additional case (Fig. 5).
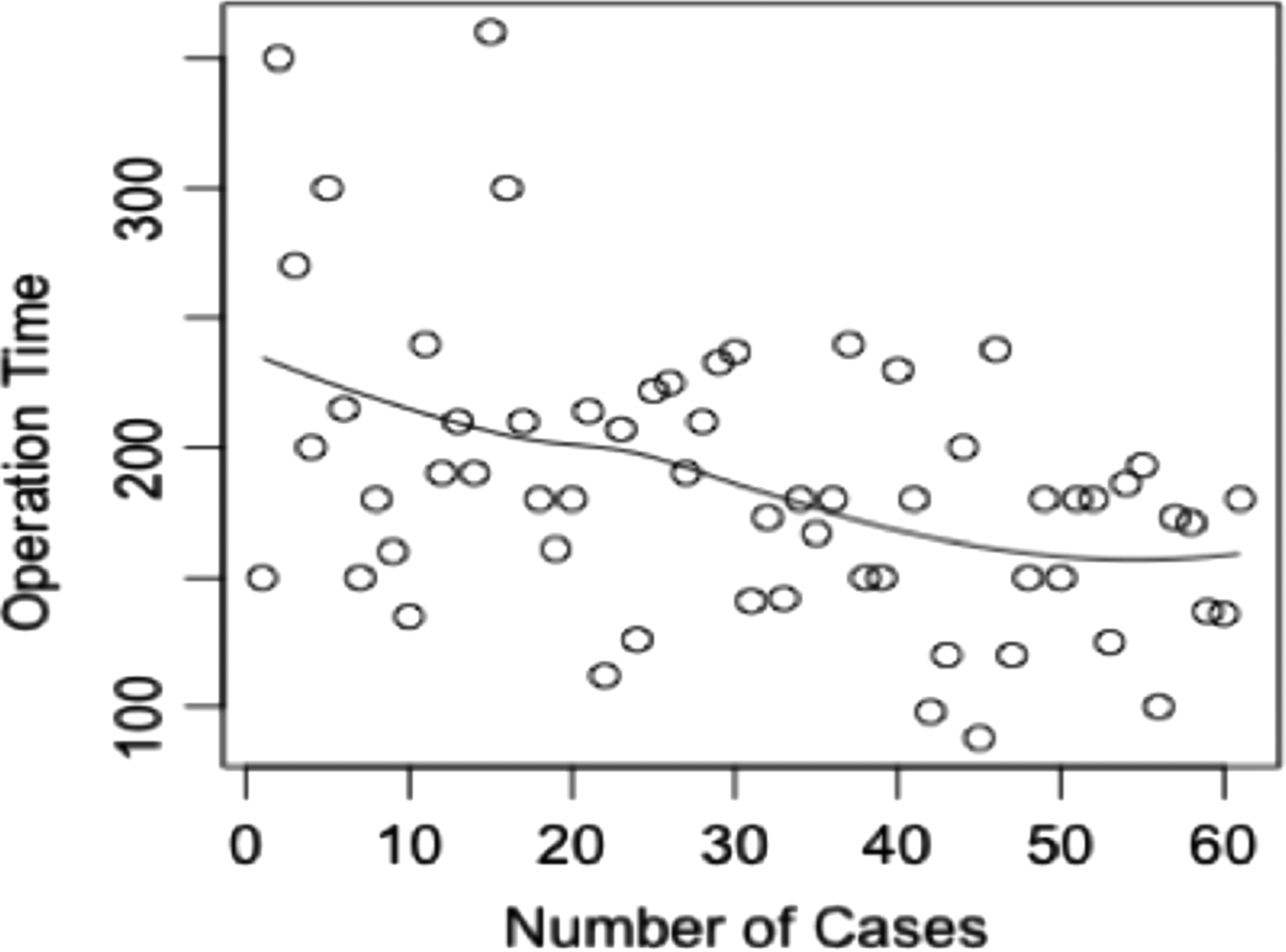
Scatter plot of operative time against number of cases.
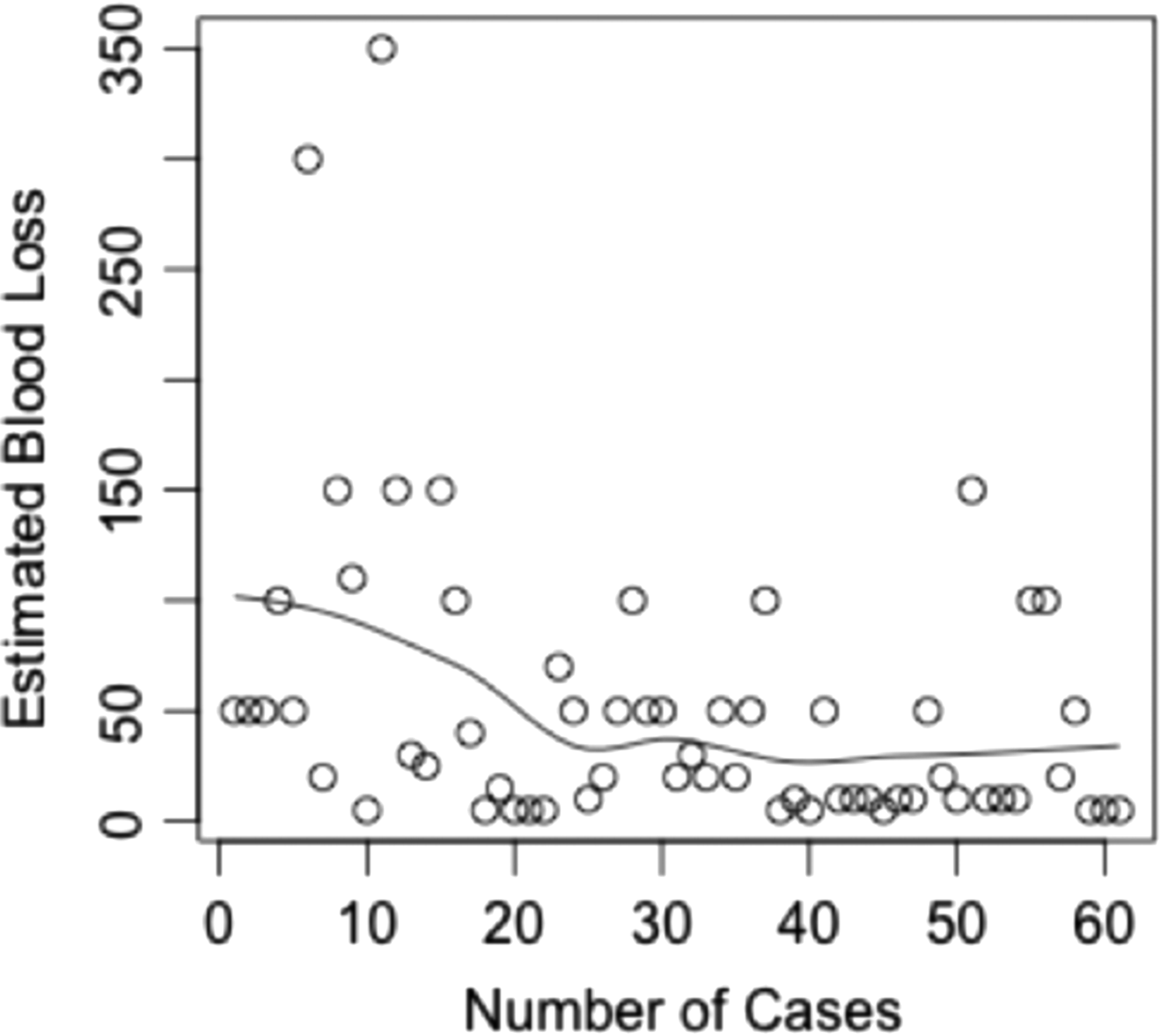
Scatter plot of estimated blood loss against number of cases.
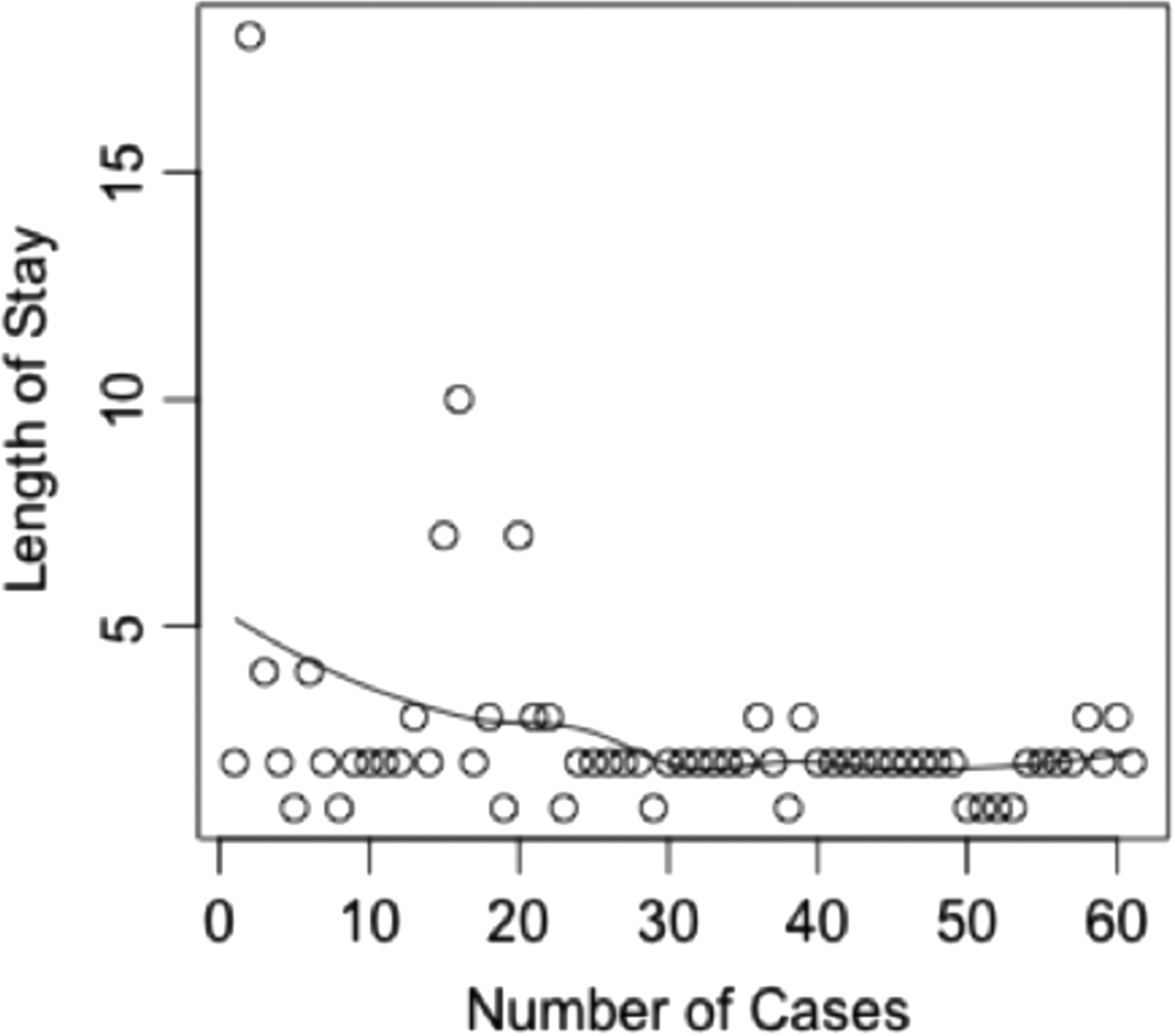
Scatter plot of length of hospital stay against number of cases.
Of the 61 patients, 4 had intraoperative complications. Specifically, one esophageal muscle tear repaired primarily with no consequences, one liver laceration due to the Nathanson retractor in an obese patient, one esophageal mucosal tear due to the 56 Fr bougie diagnosed during intraoperative endoscopy and treated conservatively, and one gastric perforation in a patient with a previous repair that required a wedge resection at the fundus of the stomach. After controlling for patient's characteristics, the complication rate decreased with the number of cases (OR = 0.85; P = .06).
There were fourteen 30-day complications (23%) in 13 patients. After controlling for patient's characteristics, there was no association between 30-day postoperative event and the number of cases (OR = 0.99; P = .49) (Table 2).
MI, myocardial infarction; PE, pulmonary embolism; UTI, urinary tract infection; DVT, deep vein thrombosis.
One patient (2%) had a reoperation, and there were 4 (7%) readmissions. The patient that had the reoperation was because he developed pulmonary embolism and required video-assisted thoracoscopic surgery due to left hemothorax after IV heparin was started. Blood loss averaged 51 mL (5–350). There were no conversions, neither to an open procedure nor to conventional laparoscopy. Patients were given clear liquids the night of the operation or the following morning. Mean length of hospital stay was 2.6 days (1–18), with 77% of patients discharged within 48 hours or less. There were no deaths.
Discussion
The purpose of this study was to determine if the robotic approach for the treatment of PEH provides results equivalent to the standard laparoscopic approach. Our goal was to resemble, with the assistance of the robotic system, the same surgical technique previously popularized by others.13–18 The essential technical principles followed were: (1) tension-free reduction of the stomach and esophagus with hernia sac resection, (2) primary crural closure with mesh reinforcement, and (3) intra-abdominal anchoring of the stomach with an antireflux procedure.
Advocates of robotics have suggested that the ease of robotics may decrease the learning curve in complex cases. 19 However, the validation in clinical practice is insufficient. Since the beginning of our experience, we observed some distinctive features of the robotic procedure worth noting. First, a variety of time-saving features were observed such as a surgeon-controlled camera and the use of the fourth arm to facilitate practically “solo surgery.” Second, the increased length and wristed movements of the instruments simplified the transhiatal dissection of the hernia sac from the mediastinum and the circumferential dissection of the esophagus. The aforementioned benefits have allowed us to minimize intraoperative complications by enhancing visualization of the operative field in the posterior mediastinum with minimal assistance from the patient bedside. Finally, the steadiness of the crural repair using intracorporeal sutures, replicating the open technique, allowed us to approximate the hiatus primarily in every case.
Early in our experience, it made sense to avoid morbidly obese patients, patients who had previous hiatal hernia repair, and patients that required simultaneous procedures, as this would likely increase the complexity of the surgery. However, with experience, patients with previous repairs or even patients that required concurrent bariatric surgery were performed safely with this approach. Nonetheless, we felt it was meaningful to define the learning curve for the use of robotics in paraesophageal hernia repair. Okrainec et al. determined that surgeon experience was an independent prognostic factor of recurrence after laparoscopic hiatal hernia repair. 11 The authors established that about 20 cases were necessary to decrease the recurrence rate. However, they did not consider the surgeon or surgeon-related factors in their analysis. Others believe that the learning curve should be defined by the relationship between experience with a new procedure and perioperative variables that a surgeon needs to be able to perform with a reasonable outcome. 20 To define the learning curve, we used nonparametric regression to explore the relationship between each of the outcomes and the number cases. Our analysis established the existence of a steep learning curve with OT showing change points as early as case 16 and sustained improvements extending until case 30. Analogous change points were detected for EBL and hospital stay with every additional case (Figs. 4 and 5). Therefore, with increased surgeon's experience and standardization of the operative steps, a steady decrease in OT, amount of blood loss, and length of hospital stay was observed. In addition, complications also decreased over time.
This relatively short learning curve for this procedure compares favorably to the learning curve described recently by Neo et al. 10
Undoubtedly, the fact that in our center we perform a wide variety of cases increased our expertise with robotics.21–24
These results suggest that even in our early phase of experience with robotic paraesophageal hernia repair, we were able to obtain clinical results similar to those of larger laparoscopic series as demonstrated in a recent systematic review, including more than 900 patients 25 (Table 3).
Conv., conversion; EBL, estimated blood loss; OT, operative time; IC, intraoperative complication; PC, postoperative complication; LOS, length of hospital stay.
Although our experience demonstrates that RA-PEHR is feasible, it is still a technically difficult procedure. In the first half of the experience, OTs were longer and there were more complications associated with the procedure, which eventually resulted in longer hospitalization. These difficulties may elucidate that there is a distinct learning curve while introducing a new technology. Therefore, before embarking on RA-PEHR, sufficient experience in robotic surgery is essential to maintain technical skills along with advanced laparoscopic skills and careful patient selection since these may help reduce the slope of the learning curve. Hence, the learning curve might be longer for surgeons who are not experienced in advanced minimally invasive techniques.
Finally, the rate of radiologic recurrence shown in this study was 42%. Interestingly, the median follow-up for patients with anatomic recurrence was 24 months, indicating that the durability of the repair deteriorates over time. Despite the increased rate of anatomic recurrence, the majority of patients were still asymptomatic.
The present report represents the learning curve of one surgeon (C.A.G.) and tries to offer a more mature perspective on the emerging field of robotic general surgery.
Obvious limitations of this study are the retrospective nature of the analysis, the lack of a control group, and the short follow-up.
Conclusion
This report represents the largest series of RA-PEHR to date and the outcomes seem to be comparable to those achieved by the conventional laparoscopic technique. RA-PEHR is a safe procedure that has a learning curve of about 36 cases. With increased experience, the OT, hospital stay, and complications decrease without compromising the surgical principles. Future studies with larger number of patients and prospective randomized control trials are needed to demonstrate the durability of this procedure compared with the current laparoscopic approach.
Footnotes
Disclosure Statement
Dr. Galvani received a research grant from Karl Storz. The other authors declare no competing financial interests exist.