
Abstract
Abstract
Background:
To investigate the similarities and differences of laparoscopic complete mesocolic excision (CME) to a colon resection with a D3 lymphadenectomy for the stage II/III left-sided colon carcinoma.
Methods:
Patients between July 2011 and August 2014 were randomized into D3 and CME groups. Mesenteric area, log odds of positive lymph nodes (LODDS), and other operative parameters were collected and assessed.
Results:
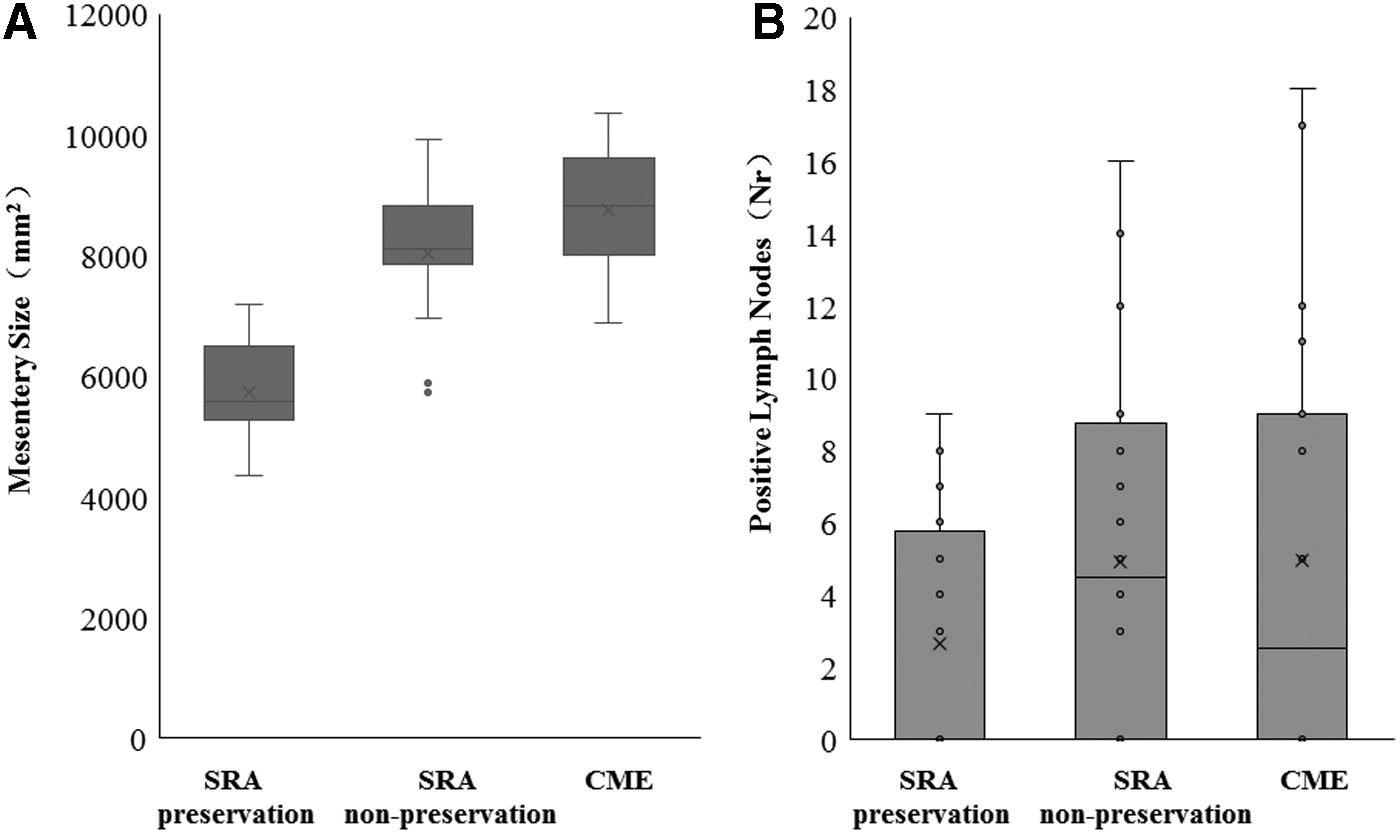
The average specimen sizes were 5730 ± 828 mm2 in superior rectal artery (SRA)-preserving D3, 8145 ± 1022 mm2 in SRA-nonpreserving D3, and 8745 ± 1039 mm2 in the CME group; the differences were significant (P < .0001). The number of lymph nodes collected from CME specimens was larger, but the CME specimens did not contain an elevated value of LODDS or positive nodes or lymph node ratio (LNR). There were also no significant differences between recovery times of bowel function. Although it took more operation time in D3 approach, especially in SRA-preserving D3 operation, the difference was not significant. Concerning the leakage rate (P = .34) and vessel-related complications (P = .64), there were no significant differences either.
Conclusions:
Both standard D3 resection and CME could achieve a high quality of mesocolic plane grade for stage II/III colon cancer. The LODDS and LNR were comparable, and those were not relevant to mesenteric size.
Introduction
D
Based on the anatomy and embryology, CME has already been the standard procedure for colon cancer excision, which ensures the complete removal of the mesocolon by “high ligation of central vascular,” “cutting off main vessel,” and “central lymph node dissection.” However, D3 excision has also achieved more than 15 years of satisfactory clinical outcomes in Asia, especially in Japan, China, and South Korea. 5 D3 excision underlined the dissection of lymph nodes that were located at the root of the central vessels.6,7 This study is to investigate the similarities and differences of laparoscopic CME to a colon resection with a D3 lymphadenectomy for the stage II/III left-sided colon carcinoma.
Materials and Methods
Patient selection
A prospective trial was performed in the Shanghai Minimally Invasive Surgery Center between July 2011 and August 2014. Forty-one cases with colorectal cancer went through laparoscopic left-sided colon resection and were randomly divided into two groups: the D3 and CME group. Primary outcome (lymph node ratio [LNR]) and secondary outcomes (size of mesentery specimen, positive lymph nodes, leakage, etc.) were compared between the two groups.
The inclusion criteria were patients with descending colon, sigmoid-descending colon junction identified by preoperative histopathological biopsy, computed tomography (CT) scan, MRI, and endoscopy findings; with preoperative tumor stage II or III according to the AJCC 7th, emergency resections were excluded, so that 38 patients were included in this study. Video and photographs of the operation and the resected samples were assessed by three independent professional observers to evaluate the quality of the approaches.
Informed consent was obtained from all patients. The primary outcome of this study was the LNR, which ranges from 0.2 to 0.4; a previous study demonstrated that the values were well spread across 0.2–0.4, with a mean of 0.28 and standard deviation (SD) of 0.27 and 20 patients per arm. An independent t-test would provide 80% power to detect a difference between groups at two-sided α of 0.05. Assuming a dropout rate of 20%, we thus aimed at enrolling 20 subjects in each arm.
Eligible patients were randomly allocated to CME or D3 colorectal surgery. To obtain a balanced distribution of different surgical procedures in the two groups, randomization lists were generated by a computer program, assuming that all patients had the same probability of undergoing CME or D3 surgery. Randomization by individual random numbers was also performed. Assignments were made by means of sealed sequenced masked envelopes that were opened, before the induction of anesthesia, by a nurse unaware of the trial design.
Ethics statement
Protocol approval for all research performed was obtained from the Medical Ethics Committee of Shanghai Ruijin Hospital according to the Declaration of Helsinki.
Operation procedure
Laparoscopic CME in left hemicolectomy
The dissection started at the left colic artery (LCA), and the root of inferior mesenteric artery (IMA) was then ligated with Ham-o-Locks, preserving the preaortic fascia (PAF)8,9 and the superior hypogastric plexus (SHP) 10 (Fig. 1A, B). Dissection was performed until the pancreas was detected after an incision of the Treitz ligament (Lig Treitz) (Fig. 1C). After separating the right gastrocolic ligament (RGL) and splenocolic ligament (SCL) (Fig. 1D), the origin of the inferior mesenteric vein (IMV) was ligated after dissecting the inferior edge of the pancreas (Fig. 1E). Lymph nodes surrounding the mid-colic artery (MCA) and its left branch were dissected, and the vessel was ligated. The dissection of the splenic flexure area was laterally followed by dissection of the left lateral peritoneal reflection, colofascial and mesofascial plane mobilization, and dissection of the peritoneal reflection at the base of mesosigmoid to the extraperitoneal space (EPS) (Fig. 1F). The Toldt's fascia was dissected from the iliac ridge to the splenic flexure to dissect the phrenicocolic ligament (PCL) and sustentaculum lienis, which acted as a brassiere to the lower pole of the spleen.
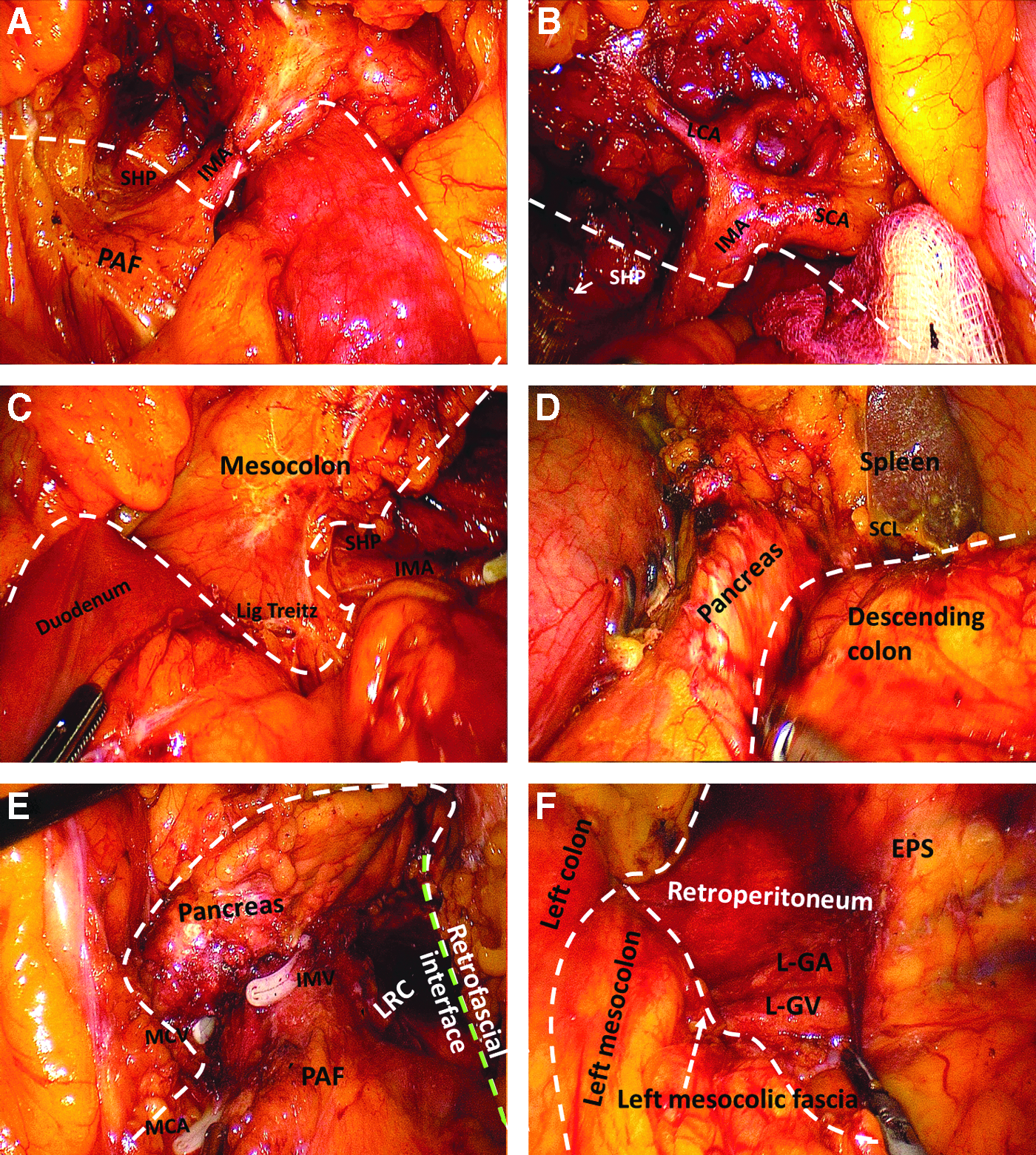
Laparoscopic CME in left hemicolectomy.
Laparoscopic D3 lymph node dissection
The harvested lymph nodes were mapped according to the Japanese guideline. According to this guideline, lymph nodes over the root of IMA were defined as N3 lymph nodes, 11 and therefore, the D3 lymph node dissection was performed as follows 12 : for the cancers of descending colon, and for those tumors whose feeding vessels proximal to sigmoid colon were the first branch of sigmoid colon artery (SCA), the root of IMA was exposed with an ultrasonic surgical device. The LCA was then exposed, clipped, and cut, however, the superior rectal artery (SRA) was preserved—SRA-preserving D3. In the other way (SRA-nonpreserving D3), the central vessel IMA should be ligated at the root. 13 After the lymph node (LN) dissection, the mesentery of the sigmoid and descending colon was mobilized posteriorly in a medial to lateral approach, maintaining the layer on the left ureter and gonadal vessels14,15 (Fig. 2).

Schema of laparoscopic D3 left hemicolectomy. The gray line shows the cutting strategy for SRA preservation and the black line shows the cutting strategy of the D3 dissection without SRA preservation. LCA, left colic artery; SCA, sigmoid artery; SRA, superior rectal artery.
Calculation of mesenteric size
Previous studies measured the length of specimens, or used softwares to measure the macroscopic area. Instead, this study calculated the area of left mesocolon with a formula. Important specimen parameters were included to reduce measurement errors induced by the inconsistency of proportional scale (Supplementary Fig. S1; Supplementary Data are available online at www.liebertpub.com/lap).
Assessments of the operation
The plane of dissection was evaluated by a histopathologist on the basis of the presence and extent of any identifiable mesocolic defect. The grading system referred to the system reported by West et al., 16 including dissection in the mesocolic plane (intact mesocolon), intramesocolic plane (significant mesocolic defects that do not expose the muscularis propria), or muscularis propria plane (significant and extensive defects that expose areas of muscularis propria).
Log odds of positive lymph nodes
First, the fresh specimens were examined by the surgeons, the lymph nodes were carefully mapped according to their location, and then, whether there were more lymph nodes that remained was double checked by the pathology department. The LNR was defined as the number of positive lymph nodes divided by the number of examined lymph nodes (NELN). Log odds of positive lymph nodes (LODDS) were classified according to log (number of positive nodes + 0.5)/(number of total examined nodes-positive nodes + 0.5) values as follows: LODDS0 (≤−1.36), LODDS1 (−1.36 to −0.53), and LODDS2 (≥−0.53). 17
Statistical methods
Logistic regression was performed to analyze the correlation of mesentery sizes and LNR. A paired Student's t-test and ANOVA were also used. Analyses were performed with Stat View 5.0 for Windows (SAS Institute, Inc., Cary, NC). The χ2 test or Fisher's exact test was applied to analyze the categorical variables, as appropriate. A probability (P) value of <.05 was regarded as statistically significant.
Results
There was no significant difference in age (P = .35), gender (P = .57), BMI (P = .54), tumor location (P = .20), ptumor stage (P = .74), intraoperative blood loss (P = .46), and splenic bleeding (P = .65) among these groups.
Assessment of plane grades
Eighteen cases were considered as mesocolic plane grade in SRA-preserving D3 group, 19 cases were considered as mesocolic plane grade in the SRA-nonpreserving D3 group. In CME group, mesocolic plane grade and intramesocolic plane grade were 19 and 1 cases; the differences between the two groups were insignificant.
Mesentery size
The average specimen sizes were 5730 ± 828 mm2 (SRA-preserving D3), 8145 ± 1022 mm2 (SRA-nonpreserving D3), and 8745 ± 1039 mm2 (CME group), respectively. The differences between SRA-preserving and SRA-nonpreserving groups were significant (P < .0001), so were the differences among the three groups (P < .0001). It was because that the incisal margin should be ∼10 cm longitudinally in D3 excision, following the so-called 10 cm rule, the length was measured by laparoscopic forceps during the operation. However, there was no significant difference between the SRA-nonpreserving group and CME group (P = .0538) (Figs. 3 and 4).
The correlation among area of mesentery
The correlation among positive lymph node ratio
Positive lymph node, LODDS, and LNR
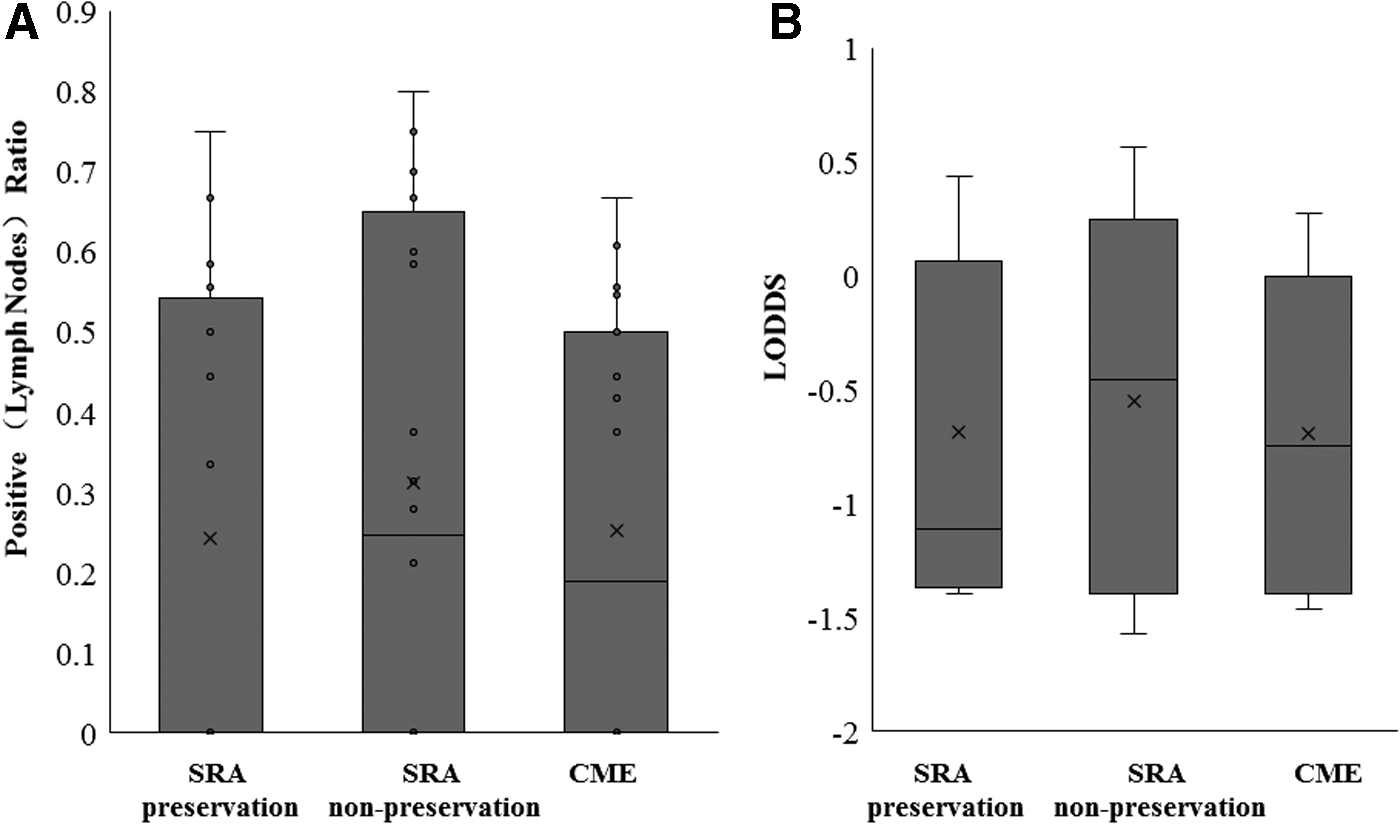
More lymph nodes were harvested in SRA-nonpreserving D3 and CME specimens compared to SRA-preserving D3 specimens (P1 = .004, P = .05), but not between the former two groups (P = .67) (Table 1 and Figs. 3 and 4). The LNRs were 24%, 31%, and 25% in those groups and did not show a significant difference (P = .75, P1 = .57, P2 = .49). Furthermore, the regression analysis showed that the mesentery size was related to total LN, but not to the LNR. Nine in 31 cases of stage III patients had the positive center lymph nodes. Interestingly, we also found unilateral double ureters in one of the patients (Fig. 5C).

P1, P-value between SRA-preserving and SRA-nonpreserving D3; P2, P-value between SRA-nonpreserving D3 and CME; P, P-value among the three groups.
CME, complete mesocolic excision; ED, excision edge; LN, lymph node; LRC, left retrocolic space; LNR, lymph node ratio; LODDS, log odds of positive lymph nodes; PM, proximal margin mesocolon; SRA, superior rectal artery.
Other articles suggested that LODDS provide more valuable information than LNR independently of the NELN. In the present study, there was no significant differences in LODDS among each group (P = .80). And notably, LODDS and LNR curves have a similar trend.
In this study, the distance between proximal margin/distal margin and central vessel was measured soon after the fresh specimens were collected, so were the Δa and sample length. There were significant differences among the three groups concerning the sinα (P < .0001), but not between the SRA-preserving group and CME group. Other data are shown in Table 1.
Postoperative short-term outcomes
There was no significant difference in bowel function recovery time, liquid diet time, and postoperative analgesia (P = .56) among these three groups (Table 2). It took more operating time in D3 operation (SRA-preserving D3, 124.6 minutes, SRA-nonpreserving D3, 119.8 minutes, CME 119 minutes, P = .67), especially in SRA-preserving D3 operation, owing to the separation and dissection for SCA and SRA, but the difference was not significant. We evaluated the postoperative complications, respectively: one patient got leakage 6 days after operation in the D3 group and one patient got leakage 5 days after operation in the CME group (P = .34). Concerning the vessel-associated complications, there was no significant difference (P = .64).
CME, complete mesocolic excision; SRA, superior rectal artery.
Discussion
CME and D3, unified and complementary
In 2006, the Japanese Society for Cancer of Colon and Rectum published the 7th edition guideline; the guideline defined again the lymph node grouping and recommended the same range for D3 dissection. A radical D3 lymph node dissection of colon cancer should be performed to remove the paracolic lymph nodes (N1), intermediate lymph nodes (N2), and central lymph nodes (N3). 18 In 2010, the Chinese Ministry of Health issued the Chinese standard for colorectal cancer treatment, 19 which recommended that lymph node dissection for advanced colon cancers without distant metastasis should cover the same three groups. For left-sided colon cancers, D3 dissection specially clears the lymph nodes located along the root of IMA (between the origin of the artery and that of the LCA). The advantage of D3 excision could be (1) to avoid excess mobilization of the transverse colon for anastomosis and (2) to preserve the normal sigmoid colon in view of minimally invasive surgery. What is the difference between the SRA-nonpreserving D3 and CME? Theoretically, they should be equivalent procedures with the principles of both procedures being the same. Rates for intact mesocolic plane were both high as were lymph node yield, but both were significantly greater in the CME specimens; however, lymph node positivity rates were equivalent. It was postulated that the differences between these specimens were likely related to the technique adopted by each country. The Japanese D3 has previously shown that positive lymph node spread rarely occurs beyond 10 cm from the tumor and as such, D3 rarely resects more than 10 cm from the tumor. The CME specimens in contrast were significantly longer, and hence, the resulting larger mesocolic surface area and lymph node counts. Survival and local recurrence data are similarly impressive.
Both CME and D3 approach advocate careful dissection along embryologic planes, resulting in a marked improvement in the oncologic quality of the specimen without increasing the postoperative complications or mortality rates. 20 Compared to SRA-nonpreserving D3, the CME technique usually includes removal of the next vascular arcade beyond the 10 cm margin to ensure that there was no remaining regional paracolic nodes; it probably also accounts for the marked increased resected area of mesentery in CME specimens. 21 In our previous study, which included 31 cases with left-sided colon cancer that underwent laparoscopic CME between September 2010 and December 2012, the complications were observed in 4 cases (12.9%), the total number of lymph nodes removed was 13.9 ± 5.0, including 4.7 ± 2.6 paracolic lymph nodes, 5.4 ± 3.7 intermediate lymph nodes, and 5.4 ± 3.7 nodes at the mesocolic root. 22
Center vessel ligation (CVL) and infarct layer dissection are the key points of CME technology, the main vessel ties are always performed at the root. The advantages of CVL are showed in several studies, while controversial conclusions also exist, which suggested no demonstrable benefit. Considering the harvested lymph nodes, several lines of evidence suggested that lymph node metastasis is a stochastic, rather than a stepwise, phenomenon, 23 therefore, it is not surprising that some clinical researches failed to identify a survival benefit from extensive lymphadenectomy compared to standard resection, which suggested that a therapeutic benefit of extensive lymphadenectomy in colon cancer may not be convincing. That might also explain the similarly impressive reported outcomes of left-sided colonic tumors in both CME and D3 excision. This study showed that mesentery size was not relevant to LNR or positive LN. As reported before, significant longitudinal spread is rare, about 0% for left-sided tumor; therefore, it was not surprising that the CME specimens did not contain an increased number of positive nodes. In contrast, Le Voyer et al. suggested that the number of total lymph nodes was relevant to prognosis of colorectal cancer although some of which were negative. 24 Especially for patients with pN1 tumors, survival improved as the number of collected lymph nodes increased. An absolute 23% improvement (90% vs. 67%) in a 5-year survival was achieved if more than 40 lymph nodes were identified, compared with those patients who had 10 or fewer nodes. 24
Some strategies for laparoscopic CME in left hemicolectomy
It is necessary to remove the perivascular sheath by sharp dissection for better central vessel root exposure, especially for patients with lymph node metastasis (Fig. 5A). Second, following the accurate surgical planes and spaces is also quite important, especially the mesofascial plane, 25 retrofascial interface, PAF, and LRC (Fig. 5B). Third, there are various vascular alterations. For instance, there are 6 kinds of variations of the branch vessels of sigmoid and LCA, 26 the routes of ureters also have kinds of variations (Fig. 5C,D).
Splenic flexure mobilization
Around the splenic flexure, Toldt's fascia spreads to the dorsal side of pancreatic tail, and so, if the surgeon separates splenic flexure followed by Toldt's fascia, this might naturally enter the dorsal side of pancreas, which might damage the vessels and pancreatic structure. There are two approaches to separate the splenic flexure, one is lateral approach of splenic flexure mobilization (SFM-L), which is to separate the Toldt's fascia then upwards to splenic flexure, the other; is to open gastrocolic ligament first and gradually divide the left side toward splenic flexure, which is also named anterior approach of splenic flexure mobilization (SFM-A). In detail, in SFM-L, the surgeon would stand at the right side of patients, after mobilization of the omental bursa from the lateral side (close to the tail of the pancreas) was performed. In SFM-A approach, the right-sided patient position was changed to an anti-Trendelenburg position with the surgeon standing between the patient's legs. The camera should also be moved from the supraumbilical to the trocar in the middle abdomen to achieve sufficient distance to the splenic flexure. However, the latter might be easier to distinguish the pancreatic tail with visual control, so as not to damage the structure. It was suggested that there was a significantly higher rate of intraoperative complications in the SFM-L group compared to the SFM-A group. It is also reported that a shorter operative time can be taken during the medial to lateral approach (Supplementary Fig. S2).
Recognize PAF, retrofascial interface, and the mesofascial plane
There were prerenal fascia posterolateral to the left mesocolon, PAF median to the left mesocolon, parietal layer of the pelvic fascia posterolateral to the mesorectum, which continued at different sites. Peritoneum resection was performed along the aorta to the top, the PAF is exposed under the peritoneal connective tissue, which extends upward till the dorsal side of the duodenum and contains autonomic nerve fibers inside.
Recently, Coffey et al. found that the peritoneal occurs wherever the mesenteric organ is opposed to the retroperitoneum, so that to gain access to the mesofascial plane, a peritonotomy of the peritoneal reflection in this location is required. When this is lengthened, and the interface placed on stretch, it might be possible to separate sharply the components of the mesofascia interface without disrupting the integrity of either.27,28
It also showed the contiguity among the mesorectal fascia, the mesosigmoidal fascia, and the left mesocolic fascia. 29 Thus, these represent different regions of the same fascial entity. In keeping with this, the mesorectal fascia, Gerota's fascia, and the anterior pararenal fascia are different regions of the same entity. 30
Preserve the SRA or not?
Both D3 and CME could get a high rate of mesocolic plane grade for stage II and stage III patients, 31 and CME extends longitudinal mesocolon resection. In this study, a long-term follow-up and larger sample quantity would be essential. D3 excision is flexible in choosing whether to preserve SRA or not, which was determined by the clinical preoperative staging as well as intraoperative staging. SRA preservation may reduce the anastomotic tension compared to the SRA-nonpreserving D3 approach, so as to reduce the leakage rate 32 ; however, there were not enough evidences to show whether it promotes early bowel function recovery. In contrast, it was also reported that SRA preservation could be performed without compromising the quality of lymph node dissection and relapse-free survival, but no advantage of SRA-preserving approach was demonstrated. 33 In addition, the LCA might be absent in 12% patients, 34 and so, CT reconstruction is recommended for the D3 approach.
In conclusion, both D3 and CME can achieve high quality of mesocolic plane grade for stage II and stage III patients. The LODDS and LNR were comparable and without significant correlation with the mesenteric area.
Footnotes
Disclosure Statement
H.F. is currently receiving a scholarship from DAAD (Germany)-CSC (China Scholarship Counsel). For the remaining authors, none was declared. There is no conflict of interest.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.