
Abstract
Abstract
The etiology of pneumatosis and portal venous gas in ischemic colitis is debated, but one theorized cause is transmural ischemia and subsequent bacterial translocation. Traditionally though as a surgical emergency, today not all patients with pneumatosis and portal venous gas need an operation. We have reviewed recent published algorithms and applied them to our practice.
A 68
Upon examination, the patient was afebrile with a pulse rate of 68 beats per minute, and a blood pressure of 99/53 mmHg. His laboratory examinations showed a leukocytosis of 12,700/μL, a lactate of 1.4 mM, a blood urea nitrogen of 31 mg/dL, and a plasma creatinine of 1.8 mg/dL. He underwent a computed tomography (CT) scan of the abdomen and pelvis without contrast (Fig. 1).
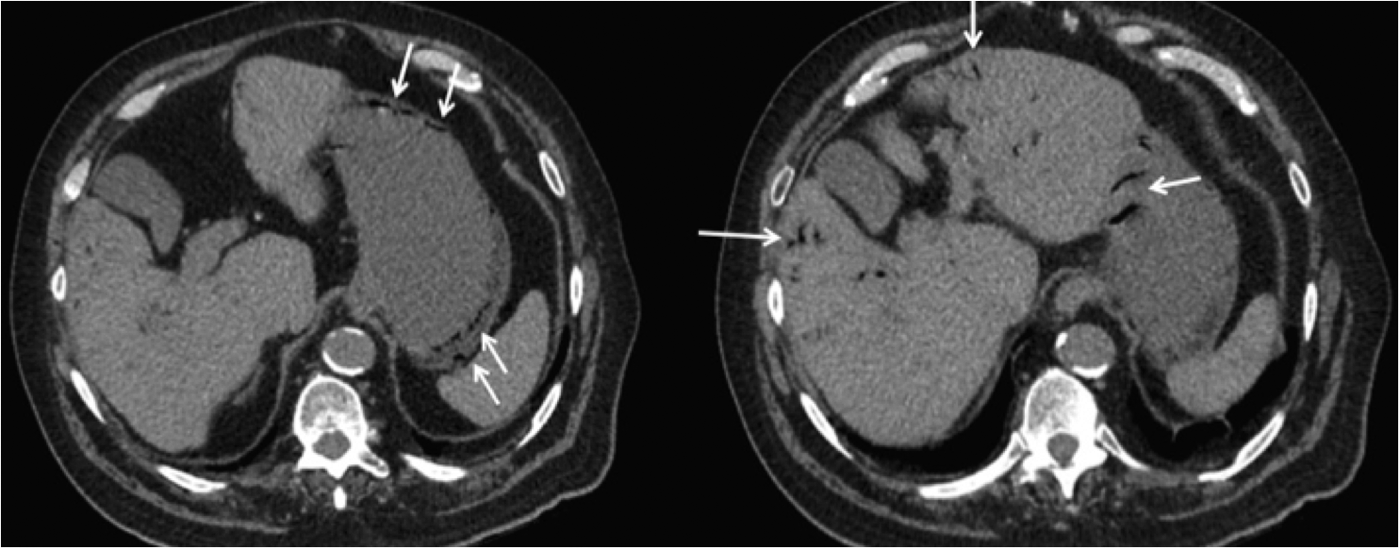
Computed tomography of the abdomen and pelvis upon presentation showing (arrows—left panel) intrahepatic venous gas and (arrows—right panel) gas in the gastroepiploic veins along the greater curvature.
This patient was diagnosed with ischemic colitis and the CT scan revealed thickened sigmoid colon, gas in the portal and gastroepiploic veins, and diffuse atherosclerotic disease involving the ostia of the mesenteric arteries. These findings altogether indicated a relative volume loss, supporting evidence of a state of low arterial blood flow, which ultimately contributed to the ischemic colitis.
The etiology of pneumatosis and portal venous gas is debated, but one theorized cause is transmural ischemia and subsequent bacterial translocation. The radiological finding often raises concern over the need for prompt surgical intervention. The use of CT has increased the incidence of this radiological finding in patients where surgical intervention is not indicated. 1
There is no prospective data regarding the management of patients with a finding of portal venous gas or pneumatosis intestinalis, but an increasing amount of retrospective evidence has identified those patients who would succeed with nonoperative management.1–5
In 2010, Wayne et al. studied 88 cases of portal venous gas and pneumatosis, showing that patients could be filtered into a treatment algorithm designed to delineate mechanical, ischemic, and benign causes of their findings and, therefore, to indicate modality of treatment. Eighteen of the 23 patients in the ischemic subgroup underwent surgical intervention, indicating that the ischemic subgroup itself could be identified as a predictor for surgical intervention. Patients were categorized in the ischemic subcategory based on a vascular risk score. Among the objective data of this score, the serum lactate level carried the most weight. 5
Nelson et al. presented a series of patients with portal venous gas along with a review of current literature. The authors suggested that the finding of hepatic portal venous gas with an elevated lactate or signs of bowel necrosis or ischemia had a mortality rate as high as 70% and, therefore, indicated aggressive, surgical management. 4
In the Eastern Association for the Surgery of Trauma multicenter study, 500 patients were studied across 8 centers. Only 20% of patients with the finding of pneumatosis or portal venous gas presented with peritonitis, leaving management in the remaining 80% to be driven by other markers of patient status. The study identified the use of vasopressors, hypotension, and a lactate greater than 2 mM as independent predictors of the need for surgical intervention. 2 Similarly, Duron et al. studied 150 patients with pneumatosis intestinalis on CT. Forty-one patients presented with a finding of portal venous gas and 28% of these patients underwent negative exploration or had successful nonoperative management. In this study, the predictors for surgical management were lactic acidemia and peritonitis, consistent with previous studies discussed. 3
In summary, data from the literature have begun to highlight a subgroup of patients with portal venous gas or pneumatosis who can be treated without surgical intervention. An elevated serum lactate and peritonitis has both been identified in several studies as predictors of the need for operative management. Our patient displayed no peritonitis, no hemodynamic instability, and no lactic acidemia. In accordance with the results of Duron et al., our patient did not have a strong indication for surgical management, and, in fact, improved both clinically and radiologically after intravenous fluid resuscitation, bowel rest, observation, and the administration of pipercillin/tazobactam to empirically cover gram positive, gram negative, and anaerobic bacteria. Figure 2 shows the CT scan that confirmed the resolution of portal vein gas after 24 hours of conservative treatment.
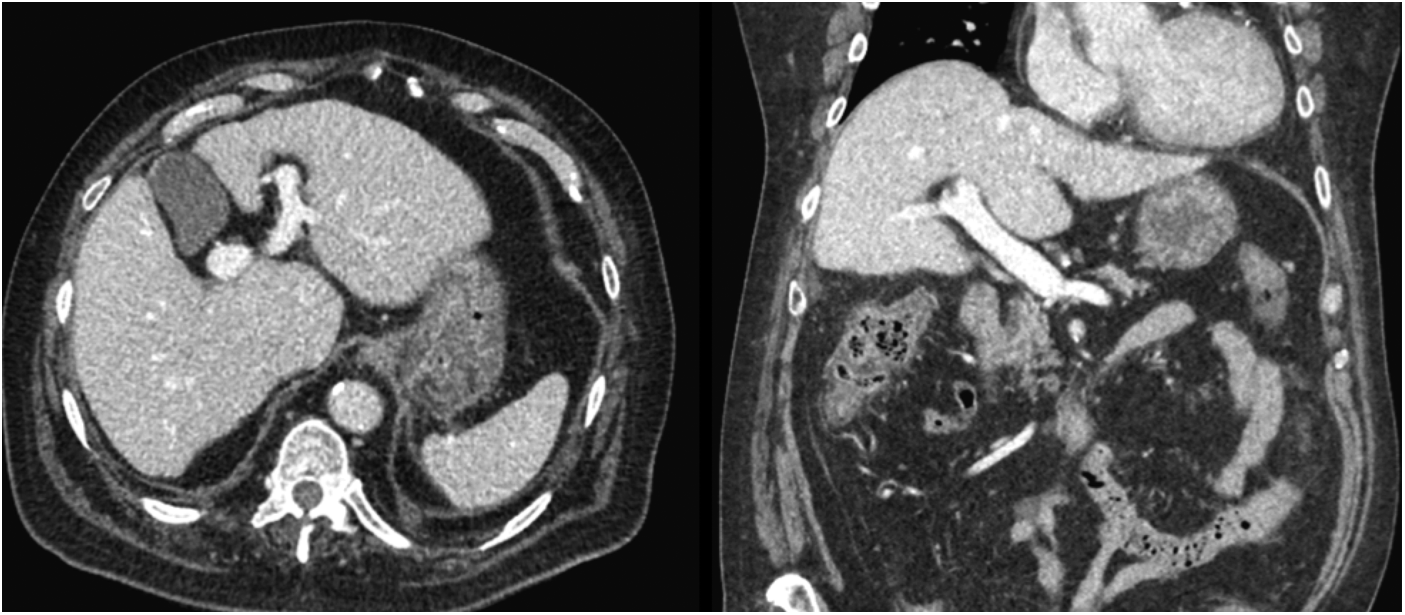
Computed tomography of the abdomen and pelvis 24 hours after conservative management. No visible venous gas present.
Footnotes
Disclosure Statement
No competing financial interests exist.