
Abstract
Abstract
Objective:
To compare the surgical outcomes of Kasai Portoenterostomy (PE) and investigate the learning curve of laparoscopic Kasai Portoenterostomy (Lap-PE).
Materials and Methods:
Retrospective chart review of 80 cases of biliary atresia (type III) undergoing Lap-PE at Shenzhen Children's Hospital from January 2011 to June 2015, all of which were performed by the same surgical team. According to the operative sequences, the cases were equally divided into four phases (Phase I, II, III, and IV), which contain 20 cases in each. The age, weight, and gender, the volume of intraoperative blood loss, the postoperative clearance rate of bilirubin, the incidence of postoperative cholangitis, and the first and second year native liver survival rate were all reviewed.
Results:
There was no significant difference among the four phases regarding age, weight at operation, and gender (P > .05). Statistical difference was observed with respect to operative time, the volume of intraoperative blood loss, the postoperative jaundice clearance, and the first and second year native liver survival rate among Phase III and IV compared to Phase I and II (P < .05), but showed no significant difference in neither the first two phases nor the latter two phases (P > .05). The incidence of postoperative cholangitis showed no significant variation among the four phases.
Conclusion:
A surgeon is able to become more experienced after performing approximately 40 laparoscopic Kasai Portoenterostomys.
Introduction
T
Materials and Methods
Study population
From January 2011 to June 2015, 80 unrelated patients with type III BA were involved at the Shenzhen Children's Hospital. This study included 42 males and 38 females with age range 46–123 days and weight range 5–6.5 kg at the time of surgery. None of the patients had any other associated congenital malformations. All the patients were followed up from 1 to 5 years after Lap-PE through phone call and outpatient clinic checkups, and were excluded if they have undergone liver transplantation or died.
Operation group
All operations were performed by the same operation group, which consisted of surgeons in department of hepatobiliary surgery of Shenzhen Children's Hospital. The operator and assistant in this group have rich experiences in open abdominal surgery, laparoscopic choledochal cystectomy hepaticojejunostomy, and laparoscopic biliary exploring operation, and can skillfully complete every procedure of laparoscopy.
Operation method
All patients underwent the laparoscopic Roux-en-Y hepaticojejunostomy reconstruction successfully. The detailed methods of the operation were reported in our previous study. 8 Parental written consent was given.
Evaluation index
According to the operative sequences, 80 patients were equally divided into four phases (Phase I, II, III, and IV). The age, weight, gender, operative time, intraoperative blood loss, jaundice clearance (the total bilirubin < 20 μmol/L within 6 months of Lap-PE), the incidence of postoperative complications, and the first and second year native liver survival rate were recorded and compared. Timing started when the artificial pneumoperitoneum was established and finished when the abdominal drainage was placed. The intraoperative blood loss was evaluated by the number of gauze (5 mL blood for each) plus the volume of aspiration. The final data were subject to anesthesia and operation records.
Statistical methods
Statistical analysis was performed using SPSS software V.22.0 (SPSS, Chicago, IL); measurement data were showed as (
Results
A total of 80 incident cases of BA were enrolled in this study, 20 cases in each phase. There was no significant difference in gender, age, and weight distribution among the four phases (P > .05) (Table 1). However, the operative time and intraoperative blood loss of Phase I and II were more than Phase III and IV, significantly (P < .05). Regarding the ratio of jaundice clearance, it was higher in Phase III (15/20) and Phase IV (16/20) than Phase I or II (P < .05).
Operative time
The operative time of Phase I, II, III, and IV were 4.8 ± 1.8 hours, 4.1 ± 1.3 hours, 3.1 ± 1.5 hours, and 3.0 ± 1.1 hours, respectively. When comparing Phase I and II with III and IV, we observed significant differences. However, no difference was found between Phase I and II or III and IV (Table 2).
Significant differences between groups.
Intraoperative blood loss
The volume of blood loss was 44 ± 11.2 mL, 46 ± 13.7 mL, 26 ± 9.1 mL, and 28 ± 7.2 mL in Phase I, II, III, and IV. Therefore, what we found was the patients in Phase I or II bleeding more than patients in III or IV (P < .05). Also, no significant difference in bleeding volume was observed between Phase I and II or III and IV (Table 2).
Jaundice clearance
There were 15 patients of Phase III and 16 patients of Phase IV recovery from the jaundice, which were significantly more than Phase I (8 cases) or II (7 cases) (Table 2 and Fig. 1).
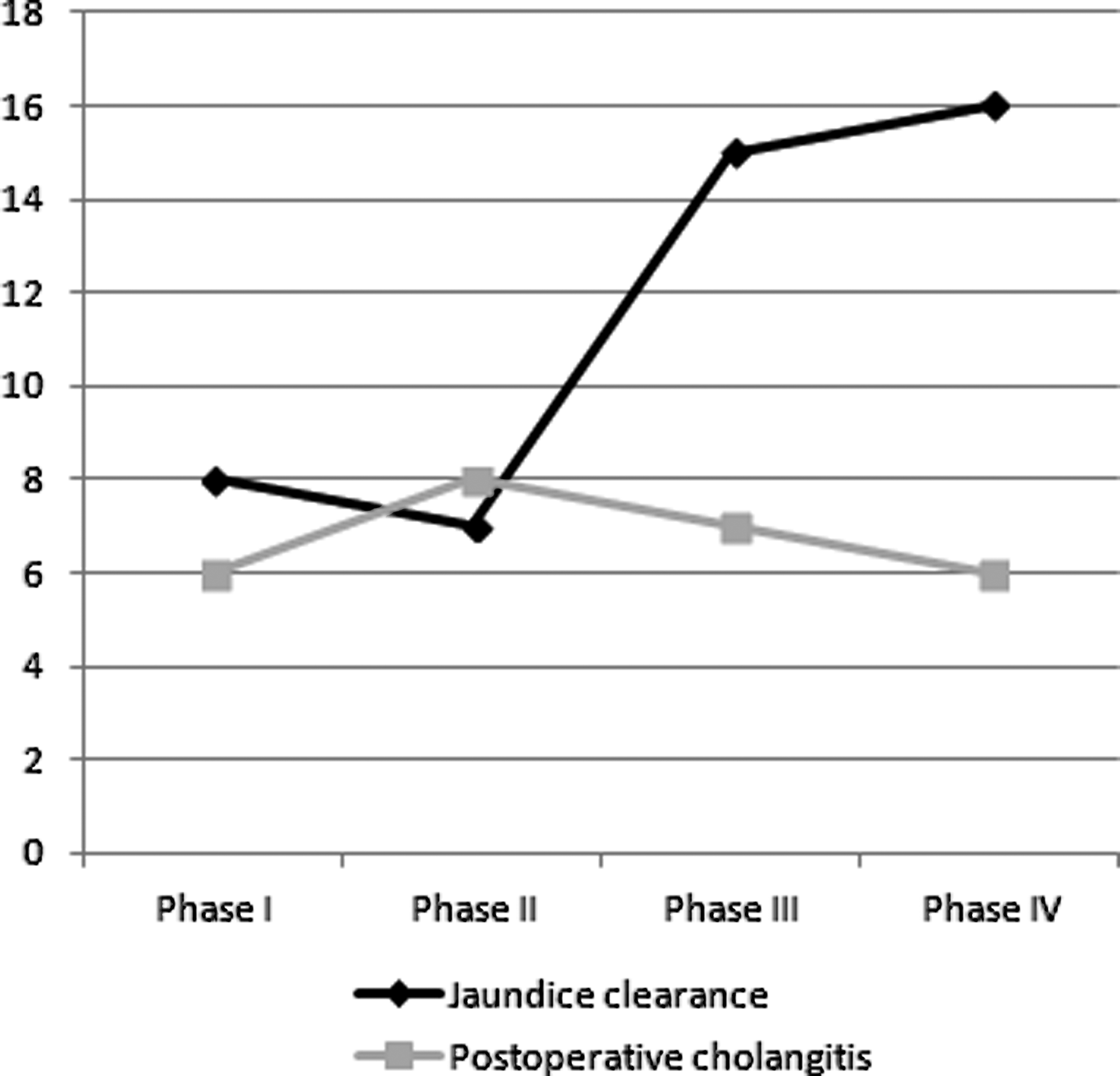
Jaundice clearance, postoperative cholangitis cases of different phase.
Postoperative complications
The comparison of postoperative cholangitis among four phases exhibited no significant difference. There were 6 cases that happened in Phase I, 8 cases in Phase II, 7 cases in Phase III, and 6 cases in Phase IV, respectively (Table 2 and Fig. 1).
The first and second year native liver survival rate
There were 16 patients of Phase III and 17 patients of Phase IV who survived within native liver in the first year of operation, which was significantly more than Phase I (10 cases) or II (10 cases). Also, there were 12 patients of Phase III and 13 patients of Phase IV who survived within native liver in the second year of operation, which was significantly more than Phase I (7 cases) or II (8 cases) (Table 2).
Discussion
Regarding to a new technique, it needs continual practice to make perfect, especially for the inexperienced operators. Moreover, every surgeon will undergo a process to handle a laparoscopic surgery, which can be reflected by a learning curve and measured with the completed operation cases. The learning curve of laparoscopic cholecystectomy showed stable after about 15 cases 10 ; then, the laparoscopic nephrectomy needs about 40 cases experience to learn it. 11 Due to lack of researches of laparoscopic Kasai surgery, no learning curve of it was reported. Hence, we summarized our experience and progress of laparoscopic Kasai to describe the learning curve of this operation.
In this study, referred to the research made by Wada et al., 7 we reviewed 80 cases to summarize the surgical treatment for BA in Shenzhen Children's Hospital. We compared the age, weight, and sex, the operative time, volume of intraoperative blood loss, the postoperative jaundice clearance, the incidence of postoperative cholangitis, and the first and second year native liver survival rate of four phases; and the results suggested that the operative time, bleeding volume, jaundice clearance, and the first and second year native liver survival rate in Phase III and IV were superior to Phase I and II. Namely, a surgeon team needs to complete at least 40 cases to master the Kasai procedure. However, there was no difference in those factors between Phase I and II or III and IV, which means that, after the first 40 cases, they may probably not gain an evident improvement, but when after 60–80 cases, the technical level became stable. Therefore, we considered that the operator might run into a bottleneck when they did 40 Lap-PEs. So, we proposed that, with the increase of frequency, the operative time, intraoperative blood loss, and jaundice clearance ratio will be more stable after 40 cases (Figs. 1 and 2).
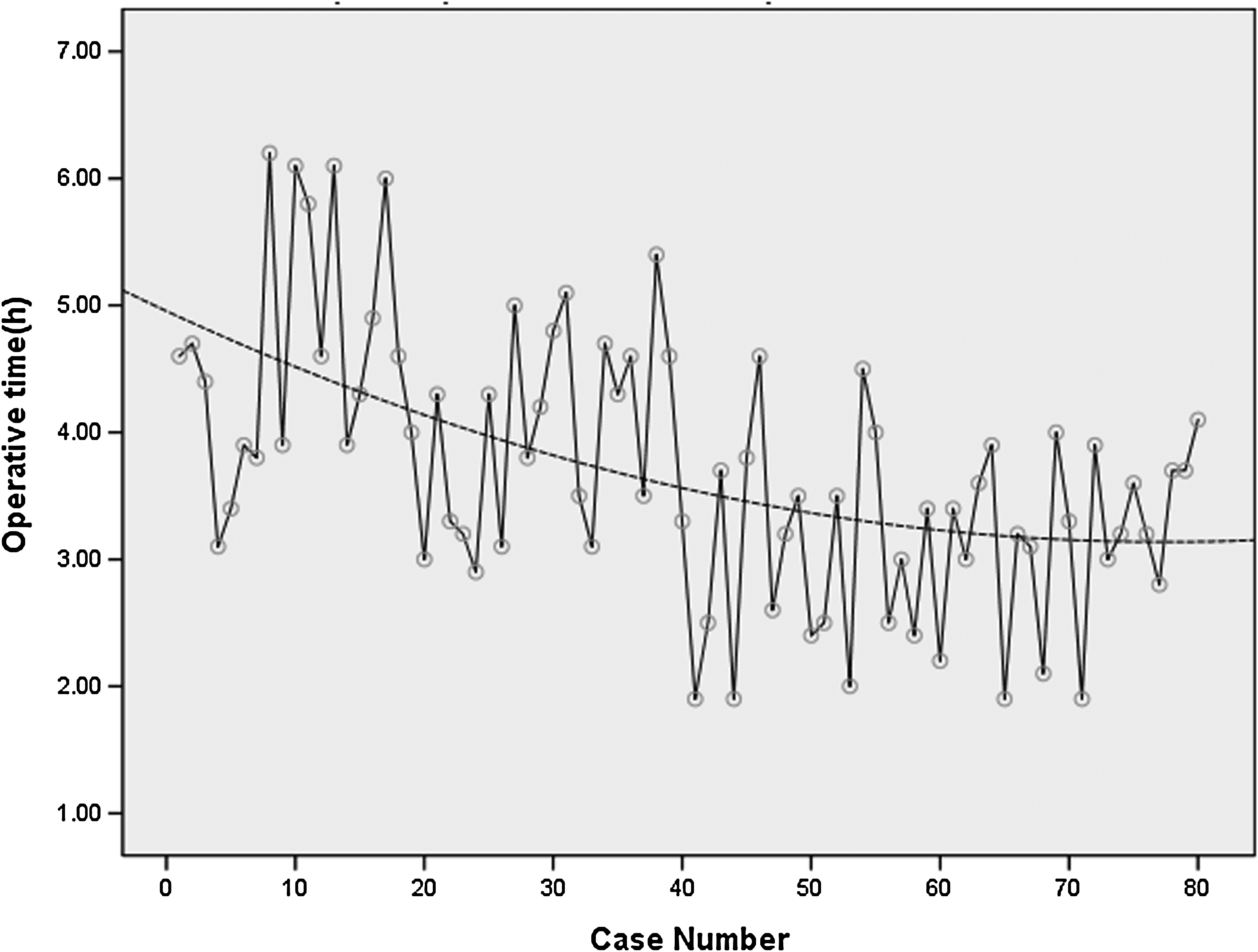
Scatter plot of operative time data with quadratic trend line.
Specially, an obvious difference of jaundice clearance ratio and the first year native liver survival rate were observed between Phase I–II and III–IV; therefore, the study was suspended provisionally and a discussion was given after phase I and II. We suggested that the prevention postoperative complication such as cholangitis and the modification of operation have been needed to settle this problem. Because of the difficulty and risk of the Lap-PE in Phase I and II, a beginner needs a long-time training to handle it. Therefore, to overcome the bottleneck of the learning curve, shorten the training time, and make a better postoperative effect, we proposed several improvements: (1) make a suspension of the ligamentum teres hepatis and the liver edge to expose the operation field. (2) When dealing with the fibrous tissue of porta hepatis, there were many tiny rete venosums between portal vein and the fiber block; operator should use the 3-mm laparoscopic electric hook to dissociate carefully along the lower edge of the tissue. More importantly, do not cauterize the left and right sides of the tissue, otherwise it will lead to obstruction of the bile track. (3) Surgeons should be alert to use the laparoscopic scissors to cut the fibrous tissue; we suggest to slowly cut it along the visceral surface of liver. In addition, what should be noticed is, the operator should remove the fibrous tissue appropriately; do not leave too much tissue or damage the liver parenchyma. The residual tissue or cicatrice on liver would probably influence the bile excretion. (4) Surgeons should use a high-resolution laparoscope to get a more clear monitor image, which will provide more information about the fibrous tissue. (5) The teamwork, to some extent, is also very important. By continuously practicing and watching the operation video to train a group of surgeons, can effectively help them improve the proficiency and speed of the Lap-PE.
Meanwhile, cholangitis is the most common early-stage postoperative complication of Lap-PE, patients in post-Kasai presenting with agnogenic fever, pejorative jaundice, or clay-colored stools, cholangitis remains the primary diagnosis that needs to be considered. Although the incidence of postoperative cholangitis showed no significant variation among the four phases and the etiology of cholangitis has remained unknown precisely, it is a significant prognostic factor associated with outcomes after Lap-PE since it may injure the biliary drainage continuously; 12 so we considered that the overtreatment is more important and used broad-spectrum antibiotics such as cefoperazone for empirical coverage or chose meropenem when the efficacy of cefoperazone had decreased.
Certainly, there are many impacts for the learning curve of Lap-PE, including the experience of open surgery, the acquaintance of hepatobiliary anatomy, the image resolution of laparoscopy, and the cooperation of the whole team. Generally, the Kasai surgery in China is still in a starting stage, besides, lacking of multicenter study that limited further investigation to support our conclusion. Although some surgeons have mastered the laparoscopic Kasai operation completely, it still ought to be performed circumspectly to avoid postoperative complications.
Footnotes
Acknowledgments
This study was supported by The Innovation of Science and Technology Committee of Shenzhen City, No. JCYJ20160429174611494.
Disclosure Statement
No competing financial interests exist.