
Abstract
Abstract
Background:
A Z-shaped colorectal side-to-side anastomosis was introduced to improve the Duhamel procedure by eliminating the rectal blind pouch. We retrospectively reviewed all total colonic aganglionosis patients treated by laparoscopy-assisted Duhamel-Z (LapDZ) between 2009 and 2014 focusing on annual fecal continence evaluation scores (CES) as an indicator of outcome.
Methods:
LapDZ was performed conventionally. Postoperatively, defecation was regulated with medications and enemas according to our standard protocol. Stool frequency, stool consistency, fecal soiling/incontinence, growth, and severity of enterocolitis were each scored (0–2) to give a total CES (maximum: 10).
Results:
Eleven subjects (6 males and 5 females) were reviewed. Mean age and mean weight at LapDZ were 10.2 months and 8.4 kg, respectively. Mean length of the aganglionic ileum resected was 19.5 cm. Mean operative time was 6.2 hours. Postoperative recommencement of oral intake took 5.7 days on average. There were no intraoperative complications, no anastomotic leaks or strictures, and no intestinal obstruction. Postoperative blood transfusion was required in 1 case complicated by chronic bleeding. No subject has been constipated postoperatively. Follow-up was for 5 years. The number of subjects who had CES assessments each year was: after 1 year (n = 11), after 2 years (n = 10), after 3 years (n = 10), after 4 years (n = 8), and after 5 years (n = 5). Average annual CES during follow-up were 4.5, 6.1, 7.7, 8.1, and 8.4, respectively.
Conclusion:
LapDZ and strict management of postoperative bowel function may have contributed to improving CES over time.
Introduction
T
The original Duhamel procedure has the benefit of less pelvic dissection and less anastomotic stricture formation, but the most common postoperative complication is fecalith formation secondary to a rectal blind pouch or remnant colorectal septum.5,6 The Z-shaped colorectal side-to-side anastomosis was introduced by Ikeda in 1967 5 to improve the Duhamel procedure by eliminating the rectal blind pouch and completely dividing the colorectal septum.
The aim of this study was to review TCA cases we treated using laparoscopy-assisted Duhamel-Z (LapDZ) from 2009 to 2014 focusing on postoperative outcome assessed by using annual fecal continence evaluation scores (CES).
Materials and Methods
We conducted a retrospective review of the medical records of all patients diagnosed with TCA between 2009 and 2014. To obtain a relatively homogenous group of subjects, patients with trisomy 21, patients with total intestinal aganglionosis, or patients followed-up for less than 1 year postoperatively were excluded.
For LapDZ, initially, four 5-mm ports were used for dissection of the entire colon beginning from the peritoneal reflection at the sigmoid colon progressing proximally to the ileostomy site following the bowel wall closely using conventional laparoscopic techniques. After the ileostomy was taken down under laparoscopic control, 7 a small Pfannenstiel incision was made to create a retrorectal route for pull-through of ganglionic ileum. The Z-shaped colorectal side-to-side anastomosis was performed through the Pfannenstiel incision (LapDZ). The rectal stump was resected 2 cm above the peritoneal reflection through the Pfannenstiel incision, and a transverse incision was made on the anterior wall of the ganglionic ileum at the level of the proximal rectal end. The posterior wall of the upper rectum and lower edge of the incised anterior wall of the ileum were then anastomosed very tightly using interrupted sutures. The incised posterior wall of the rectum and pulled-through ileum were anastomosed at the anus in a single layer using interrupted sutures. An Endo-GIA™ stapling device (60 mm Articulating Vascular/Medium Reload with Tri-Staple™ [2.0, 2.5, and 3.0 mm]; Covidien) was inserted through the anus to divide the posterior rectal wall and anterior ileal wall; usually two cartridges being required to completely resect the septum. Finally, the anterior wall of the upper rectum and the upper edge of the incised anterior wall of the normal ileum were anastomosed into two layers to complete the Z-shaped colorectal side-to-side anastomosis without a blind pouch (Fig. 1). Wounds were closed conventionally. Creating and closing the Pfannenstiel incision contributed to prolong the operative time.
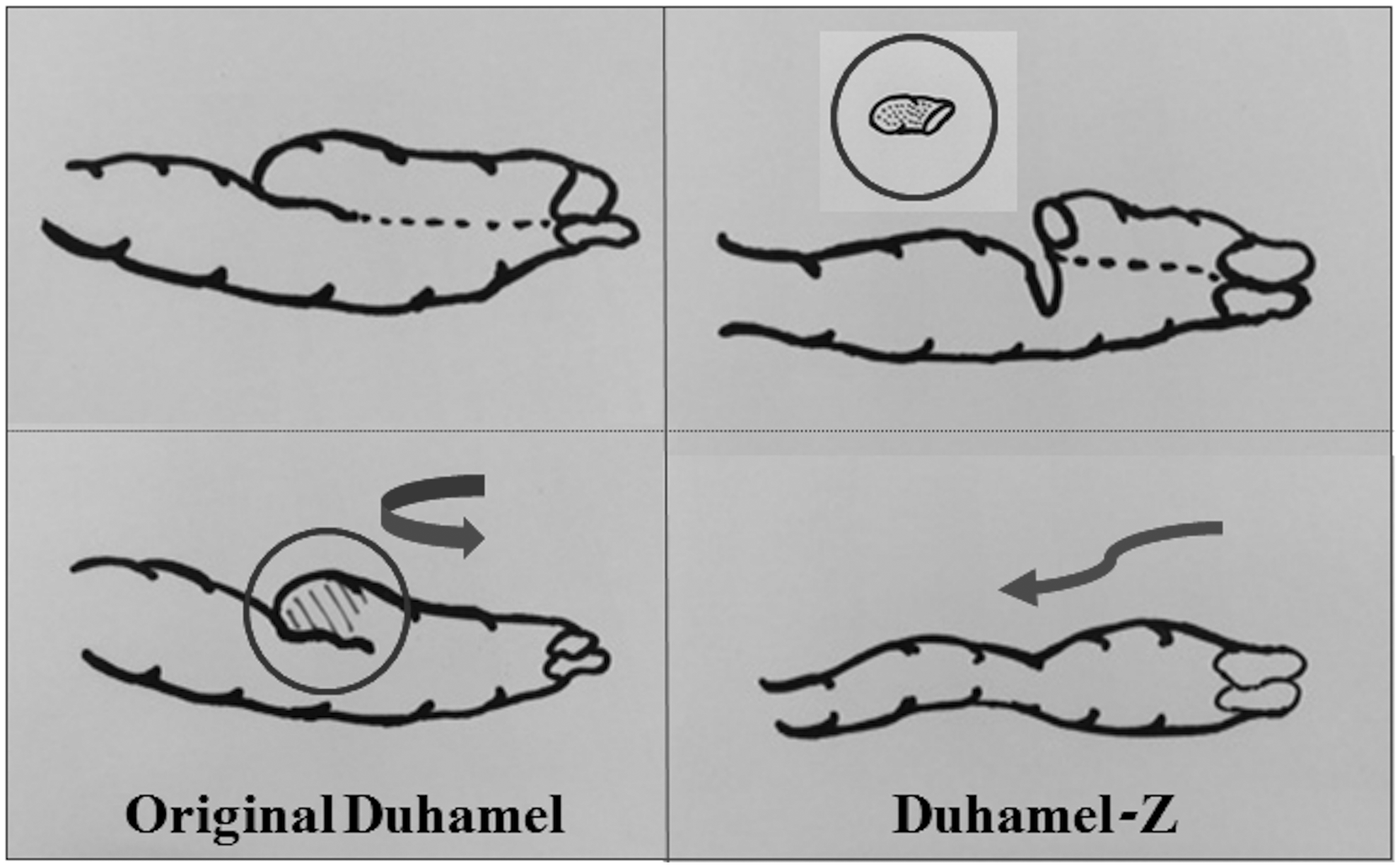
Duhamel procedure. Original Duhamel procedure (left). Duhamel-Z procedure (right). The posterior wall of the upper rectum and lower edge of the incised anterior wall of the ileum were anastomosed, and the incised posterior wall of the rectum and pulled-through ileum were anastomosed at the anus. An Endo-GIA was inserted through the anus to divide the posterior rectal wall and the anterior ileal wall. Finally, the anterior wall of the upper rectum and the upper edge of the incised anterior wall of the normal ileum were anastomosed to complete the Z-shaped colorectal side-to-side anastomosis without a blind pouch.
Postoperative bowel function was managed according to our standard protocol with daily administration of an antiflatulent (and/or antidiarrheal) medication and regular enemas supervised strictly by experienced nursing staff until discharge from hospital. From 6 months postoperatively, the frequency of daily enemas was reduced until they were ceased by 12 months postoperatively. The purpose of these enemas was more for decompression than for evacuation and as bowel function stabilized over time they were ceased, but reintroduced whenever there was any suggestion of enterocolitis, defined as the presence of abdominal distention, diarrhea, vomiting, and fever. Parents were instructed to contact us immediately by telephone for instructions if they were concerned about possible enterocolitis. Generally, our advice was to commence twice daily enemas and visit the outpatient clinic for assessment if there was no improvement.
Data were collected for demographics, clinical presentation, presence of associated anomalies, surgical management, and pre-, intra-, and postoperative complications. Continence evaluation was assessed with a standardized questionnaire covering growth, stool frequency, stool consistency, fecal soiling and incontinence, and severity of enterocolitis. A scoring system (0–2) was used for the assessment of responses to each criterion to give a maximum score of 10 (Table 1). Since our subjects were too young to be assessed for voluntary defecation, the length of time between motions as observed by the parents was used instead and scored.
SD, standard deviation.
Data were analyzed using standard statistical methods. Demographic data were compared using the Student's t-test. The chi-squared test and Fisher's exact test were used for analyzing the incidence of complications. For all statistics, P < .05 was used to determine significance.
Results
There were 11 TCA cases (6 males and 5 females) treated by LapDZ. The mean age at LapDZ was 10.2 months (range 7–16 months) and the mean weight at LapDZ was 8.4 kg (range 6.5–9.7 kg). The mean length of the aganglionic ileum segment resected was 19.5 cm. The mean operative time was 6.2 hours. There were no intraoperative complications. The mean time taken to recommence oral intake postoperatively was 5.7 days. The mean postoperative hospital stay was 18.8 days. One subject died from congenital heart disease 2 years after LapDZ. Another subject had chronic lower gastrointestinal tract bleeding causing iron deficiency anemia requiring blood transfusion 4 months postoperatively as a postoperative complication. There were no anastomotic leaks, strictures, or intestinal obstruction recorded, and no patient required redo surgery.
All subjects were managed postoperatively according to our standard protocol. No subject was constipated during the immediate postoperative period. The number of subjects who had CES assessments each year was: 11 at 1 year, 10 at 2 years, 10 at 3 years, 8 at 4 years, and 5 at 5 years; followed-up over 5 years (n = 5), 4 years (n = 3), 3 years (n = 2), 1 year (n = 1). The mean annual CES improved gradually during follow-up from 4.9, 5.9, 7.6, 8.2, and 8.5, respectively. Scores for each criterion of our continence evaluation assessment are shown in Table 2.
Number of subjects assessed after 1, 2, 3, 4, and 5 years, respectively.
Discussion
Several laparoscopic Duhamel-type procedures have been reported.8–10 However, when these procedures were performed, there was usually a short blind pouch or the upper colorectal septum may be left intact. Enterocolitis is a well-known complication of TCA, and previous studies have reported incidence rates ranging from 30% to 75%.11,12 In a 58 subject series, 13 55% of cases with TCA had one or more episodes of enterocolitis postoperatively, which is comparable to another series 14 ; 5 subjects out of 58 patients required anal dilatation, Botox® injection, or sphincterectomy to treat enterocolitis. 13
Some centers in Japan use a Z-shaped anastomosis preferentially with excellent clinical results reported mainly in patients with classical HD, 15 and recently, laparoscopic Duhamel Z-shaped anastomosis was reported for classical HD. 16 Here, we reported our experience of using LapDZ for treating TCA with bowel function assessed by annual CES. In one series, 17 only 15 of 26 patients with TCA older than 3 years were continent, which reflects a pattern reported by other authors. In 1999, Tsuji et al. reported a series of 48 subjects, of whom 82% had fecal incontinence when they were 5 years old, 14 but this had improved to 57% at 10 years of age and 33% at 15 years of age. More recently, Laughlin et al. performed a systematic review of outcomes of patients with TCA 18 ; of 739 pull-through cases investigated, long-term follow-up was available for 396, of whom 60% had satisfactory or normal bowel control, 25% had soiling, and 40% had poor outcome overall.
In our series, short- to mid-term annual fecal CES improved gradually for each criterion over time and we believe that the Z-shaped anastomosis could have contributed to the lower incidence of enterocolitis by eliminating the blind pouch at the upper rectum. Another influence on the steady improvement in CES we observed may have been our strict postoperative management protocol that involved daily enemas for the first 6 months and administration of medications and supplements both short- and long-term. After 6 months, a decision was made to commence reducing the frequency of enemas provided, parents were comfortable to recommence them at the first signs of enterocolitis and telephone the hospital for advice.
A limitation of our study is the absence of control groups. Because of this, we cannot assume that the gradual improvement in continence and lower incidence of enterocolitis observed were related just to using a Z-shaped anastomosis and strict postoperative bowel management. We could also not assess the degree to which control of bowel function improves with age because we did not have an age- and sex-matched control group. The Z-shaped anastomosis contributed to the overall improvement in annual CES observed, but the exact connection requires further study to elucidate. In the future, we plan to use a control group for direct comparison and perform longer-term postoperative fecal continence evaluation taking into account factors related to the needs and lifestyles of older children, such as presence of urge to defecate and ability to distinguish flatus from stools.
In conclusion, we believe that the laparoscopy-assisted Z-shaped anastomosis and our strict management protocol for postoperative bowel function contributed to the gradual improvement in CES seen over time in this study.
Footnotes
Disclosure Statement
No competing financial interests exist.