
Abstract
Abstract
Introduction:
We studied operating team acceptability of Video Telescopic Monitor (VITOM®) exoscope by exploring the ease of use of the device in two centers. We also assessed factors affecting surgeon musculoskeletal discomfort.
Methods:
We focused on how the operating team interacted with the VITOM system with surrogate measures of usefulness, image quality, ease of use, workload, and setup time. Multivariable linear regression was used to model the relationships between team role, experience, and setup time. Relationships between localized musculoskeletal discomfort and use of VITOM alone, and with loupes, were also analyzed.
Results:
Four surgeons, 7 surgical techs, 7 circulating nurses, and 13 surgical residents performed 70 pediatric surgical and urological operations. We found that subjective views of each team member were consistently positive with 69%–74% agreed or strongly agreed that VITOM enhanced their ability to perform their job and improved the surgical process. Unexpectedly, the scrub techs and nurses perceived more value and utility of VITOM, presumably because it provides them a view of the operative field that would otherwise be unavailable to them. Team members rated perceptions of image quality highly and workload generally satisfactory. Not surprisingly, setup time decreased with team experience and multivariable modeling showed significant correlations with surgeon and surgical tech experience, but not circulating nurse. An important finding was that surgeon neck discomfort was reduced with use of VITOM alone for magnification, compared with use of loupes and VITOM. The most likely explanation for these findings is improved posture with the neck at a neutral position when viewing the VITOM images, compared with neck flexion with loupes, and thus, a less favorable ergonomic position.
Conclusion:
This study suggests that there may be small drawbacks associated with VITOM use initially, but these reduce with increased experience and benefit both the surgeon and the rest of the team.
Introduction
I
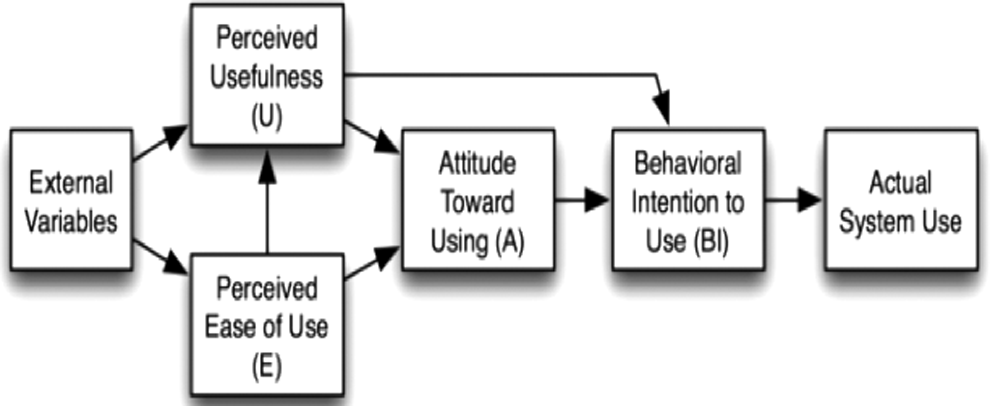
Technology acceptance model demonstrates how perceived ease and perceived usefulness (as well as a range of other variables) predict use of a new technology.
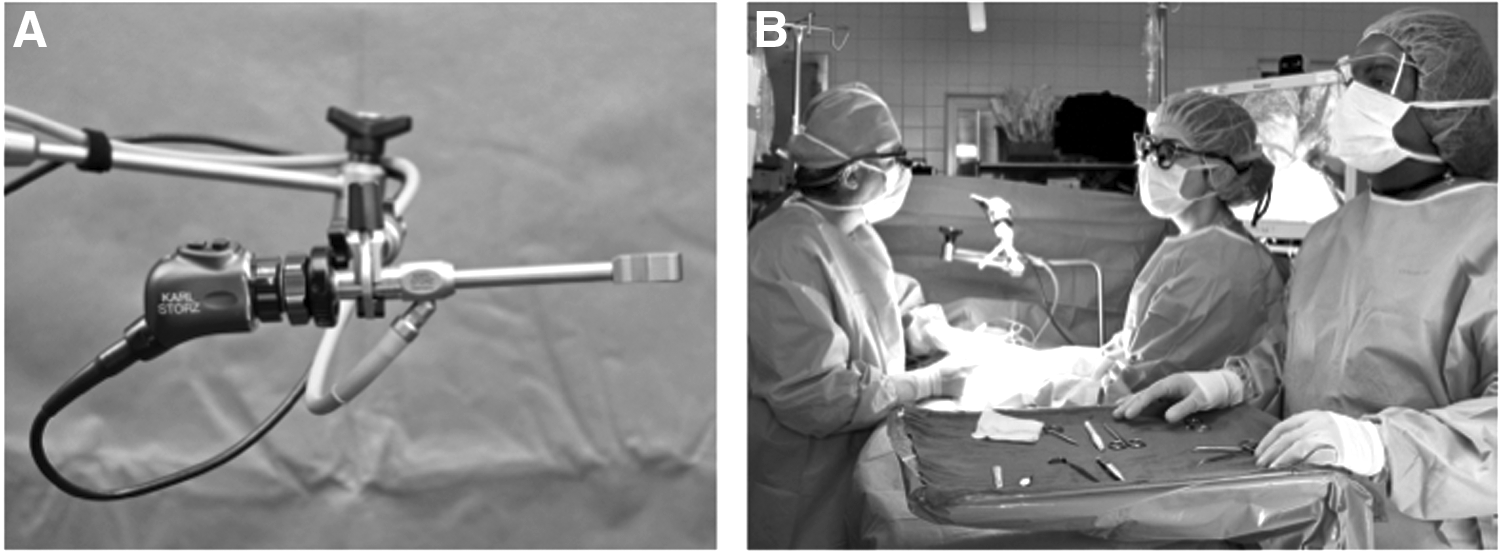
The Video Telescopic Monitor (VITOM®) exoscope system is a unique technology that displays high-definition magnified images of open surgery on a video screen (Fig. 2). The VITOM has been used in various surgical fields, although little information exists regarding how surgeons, surgical technologists, circulating nurses, and residents view and accept this novel technology. Earlier studies suggested that image quality, ease of use, and reduction in musculoskeletal strain and fatigue were potentially beneficial, with advantages for teaching. 4 Intraoperative flow remained either unaffected 5 or possibly improved. 4
We studied the use of the VITOM exoscope to assess the acceptability by exploring the ease of use of the device. We created a two-center study with both subjective and validated tools, to offer a more quantitative approach to evaluate proposed benefits. To do this, we evaluated how operating room personnel interact with VITOM system for pediatric surgical and urological cases using a range of surrogate measures of usefulness, image quality, ease of use, workload, and assessment of setup time. We also evaluated upper body musculoskeletal discomfort of the operating surgeon and surgical resident.
Materials and Methods
Institutional review board approval was obtained at CSMC (Pro00033783, coordinating site) and CNMC Pro00004673; a total of 70 VITOM operations were prospectively studied at the two sites, with four surgeons (two in each center). Other participating personnel included 7 surgical technologists, 7 circulating nurses, and 13 surgical residents.
Operations were performed utilizing the 90° VITOM II (Karl Storz Endoscopy–Tuttlingen, Germany) with an articulating stand in which the images were viewed on a 26-inch flat screen monitor. After every operation, a questionnaire was administered to each team member (Supplementary Data; Supplementary Data are available online at www.liebertpub.com/lap). This contained five questions regarding perceptions of VITOM usefulness and eight components of image quality. Perceived workload was assessed by the team (excluding residents) using the NASA Task-Load Index (TLX6,7). Musculoskeletal discomfort was measured using the Borg CR10 localized musculoskeletal discomfort (LMD) method. 8 Metrics of VITOM system setup time and surgical time were recorded either by the study coordinators or a member of the operating team for each case. The proportion of operative time spent setting up the VITOM was calculated. We also measured the number of adjustments that were made by the surgeon or operating team during the operation, to assess the amount of ongoing effort that was required to maintain performance. Multivariable linear regression was used to model the relationships between team role, experience, and setup time. Relationships between LMD and use of VITOM alone, or VITOM with surgical loupes, were also explored using multivariable linear regressions.
Results
Operations were a mixture of pediatric surgical and urological procedures such as inguinal hernia repair (n = 32), hypospadias repair (n = 10), hydrocelectomy (n = 5), orchiopexy (n = 5), and a variety of other surgeries (n = 18). The median patient age was 24 months (0.8–204 months), and median weight was 12.7 kg (2.3–71.8 kg). Mean operative duration was 1 hour 32 ± 42 minutes (range 32 minutes to 4 hours 03 minutes). Fifty cases were conducted at Cedars-Sinai Medical Center in Los Angeles and 20 at Children's National Medical Center in Washington, DC.
Usefulness
Subjective views from all four team members (Fig. 3A) were consistently positive, with 71% disagreeing or strongly disagreeing it reduced anticipation; 73% agreeing or strongly agreeing it enhanced ability to perform; 69% disagreeing or strongly disagreeing it affected operation flow; 70% agreeing or strongly agreeing it improved the surgical process; and 74% agreeing or strongly agreeing that they would want to use the device in the future. There are some differences in responses between professional groups, with nurses and scrub techs generally agreeing more strongly of the value and utility of VITOM, presumably because it provides a view of the operation that would otherwise be unavailable to them.
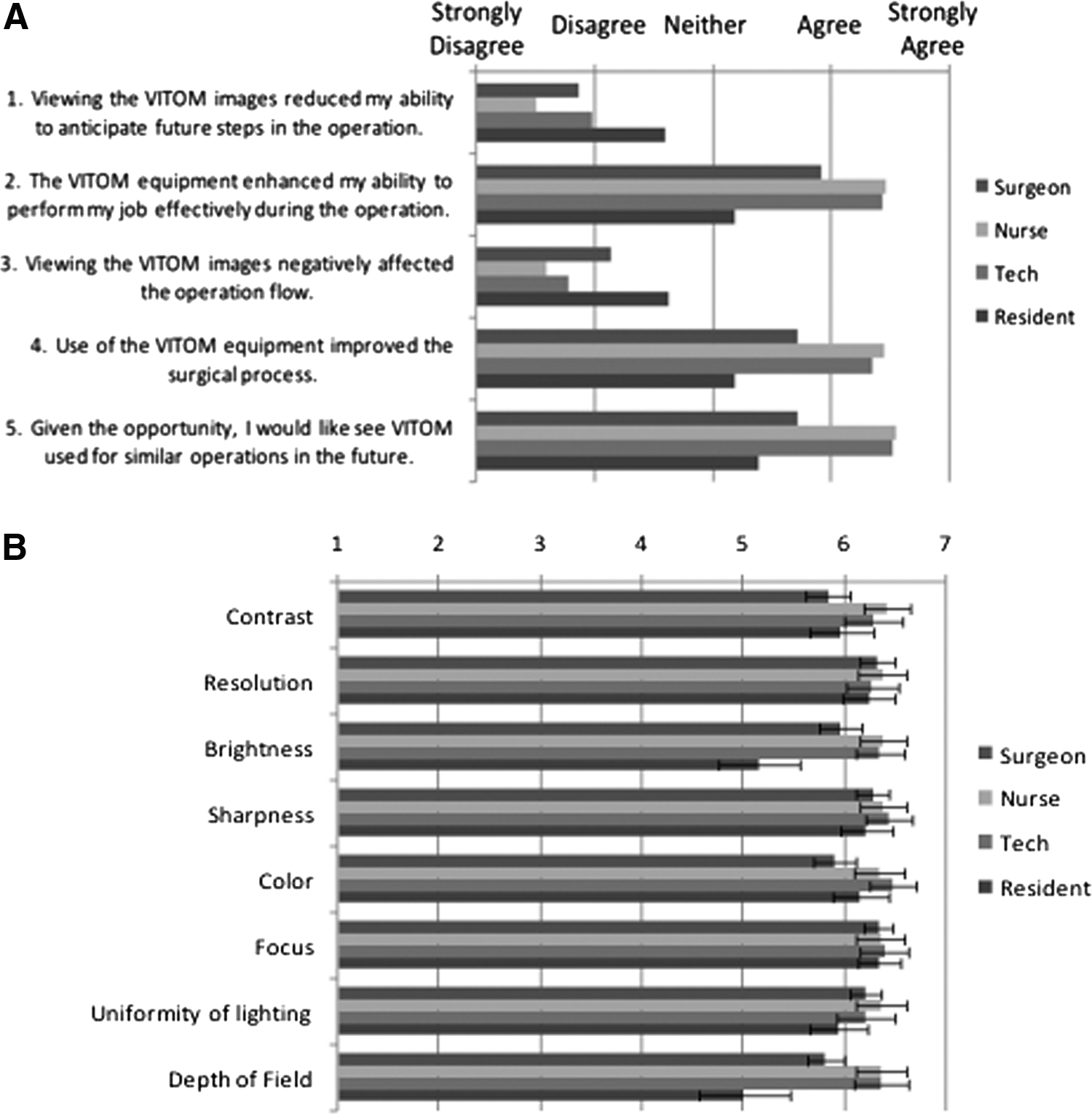
Image quality
Perceptions of image quality were almost universally high, but with some significant differences in the perception of image quality between different users. The surgeons generally perceived lower quality, with the residents scoring significantly lower for brightness and depth of field. However, nurse and tech are generally higher than the two surgeons (Fig. 3B).
Musculoskeletal discomfort
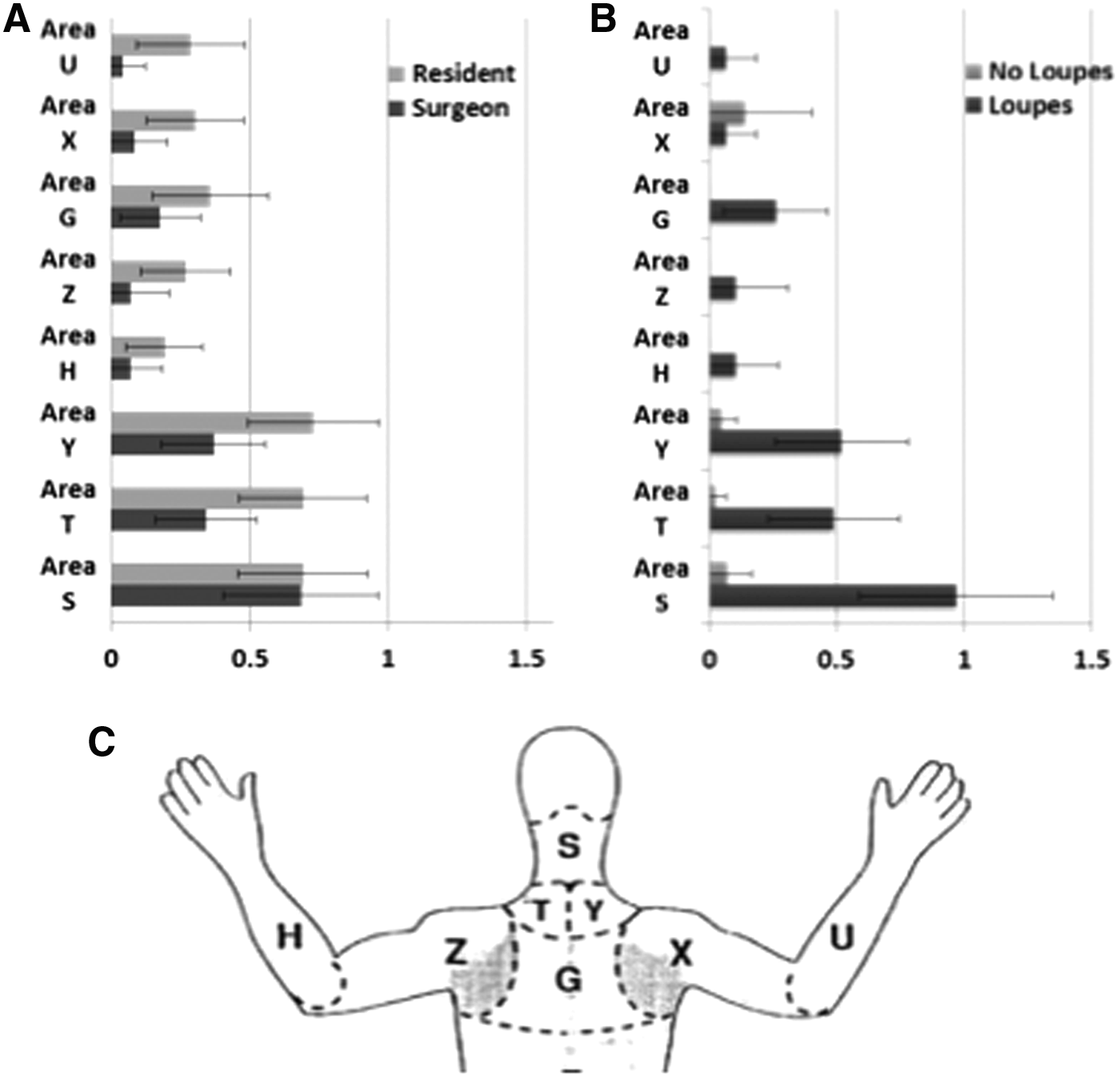
LMD ratings in general reflect little discomfort overall. Resident scores were slightly higher than the attending surgeon scores (Fig. 4A). When exploring the effect of operative duration and loupes on LMD of the surgeons, there are several significant effects. Not surprisingly, there was increased discomfort in areas S, T, Y, G and X with increased operative duration for all operations (Table 1). Conversely, surgeons experienced reduced neck discomfort (region S; r2 0.377, P = .043) yet mildly increased right shoulder discomfort (region X; r2 = 0.11, P = .0165) when the VITOM was used for magnification alone, compared with the use of loupes and VITOM (Fig. 4B, Table 1).
Localized musculoskeletal discomfort ratings using the Borg CR 10 Localized Musculoskeletal Discomforting ratings (0–10).
Statistical significance.
Workload
Workload (0–20) was generally satisfactory and below seven across all dimensions (Fig. 5). There were significant effects across different workload ratings between professional groups. In general, the surgical tech ratings are highest and the nurse ratings lowest. These data reflect the necessary work required by the surgeon and tech to setup and operate the device.
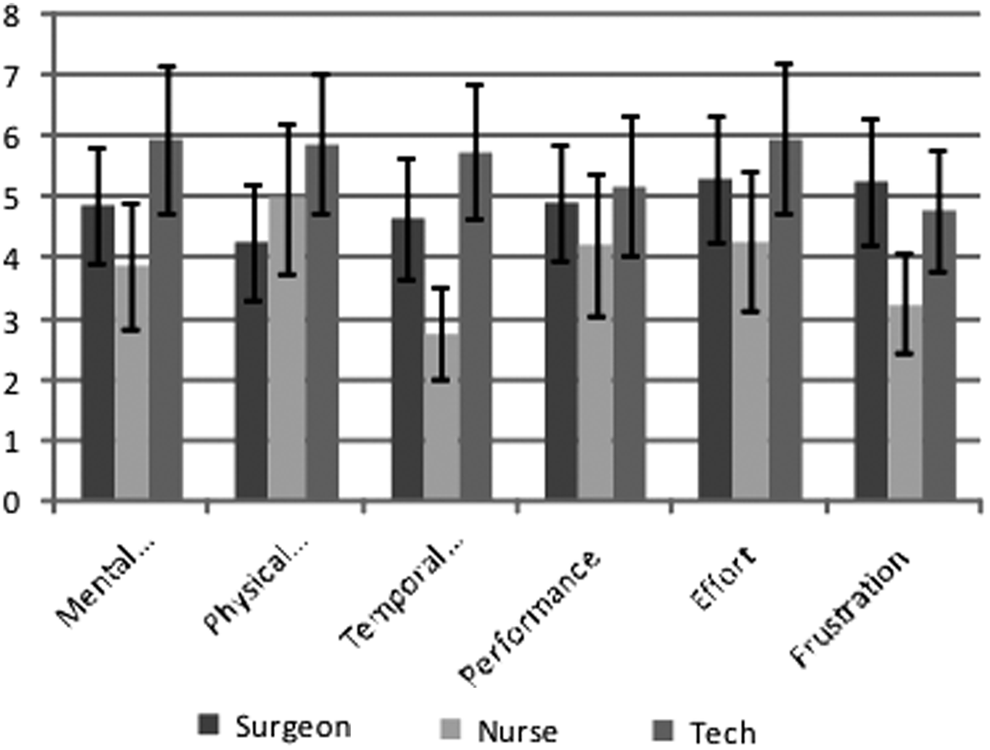
Perceived workload of VITOM setup and use by surgeons, circulating nurses, and surgical techs. Measured using NASA Task-Load Index (scale 0–20). Mean score ± SD. SD, standard deviation; VITOM, video telescopic monitor.
Setup time
Mean setup time was 4.9 minutes, or ∼8.5% of total operative duration. We noted a number of relationships between experience and the mean set up time, with an apparent curve related to experience and proportion of operative duration (Fig. 6A). When combined into a multivariable model (R2 = 0.59), this demonstrates that setup time is significantly affected by surgeon experience (F [1,5] = 9.82, P = .0037) and by tech experience (F [2,5] = 3.98, P = .0286), but not nurse (Fig. 6B).

Number of adjustments
The mean number of adjustments per case was 3.2. The most and least experienced surgeon made the most adjustments (Fig. 6C), suggesting a u-shaped function where initially adjustments are needed to setup the device, while an experienced user may then make fine-tuning adjustments to get the most out of the device. As might be expected, there is also a correlation with length of operation. Including both parameters in a linear regression demonstrates significant effect of both surgeon experience (P < .0003) and time (P < .0001), suggesting an adjustment every 20 minutes.
Discussion
VITOM is perceived as having excellent image quality and to be of use for following the progression of the case and enhancing awareness and performance. This is especially true for the scrub tech and circulating nurse, who felt they particularly benefitted from viewing VITOM images. There is also a suggestion that using VITOM solely for magnification reduces surgeon neck and right shoulder pain compared with using surgical loupes and VITOM. The most likely explanation for the findings is improved posture with the neck at a neutral position when the VITOM images were viewed, while the neck was flexed when surgical loupes were used, thus creating musculoskeletal strain from the less favorable ergonomic position. These findings may have implications for pediatric surgeons and urologists who experience significant neck pain, as the VITOM may provide an alternative to using loupes.
Workload associated with use of VITOM is moderately low, but weighted toward the surgeon and the tech, with the nurse experiencing significantly less demand, although once again this difference is not substantial. This is also reflected in the setup time, which reduces with increased expertise of surgeon and tech, with what appears to be a clear effect of surgeon expertise in relation to the proportion of operative time used. This latter effect may be because initially surgeons select shorter, less challenging operations to use VITOM.
It is worth considering these findings from the perspective of the technology acceptance framework. The subjective ratings suggest that there may be important benefits in perceived usefulness of the device. There may also be benefits for the surgeons, in terms of reduction in neck discomfort, but these may not be immediately apparent. The learning curve suggests that between 10 and 30 cases are required to reach a point where impact on operative time is not significant. Interestingly, the people who perceive it to be of most benefit are the surgical techs and circulating nurse–not necessarily the surgeon who would normally decide to use the VITOM. Thus, there may be a period where staffs feel the device will be of use, with few usability problems–predisposing them to want to use the device–while surgeons' perceptions may not be as positive, either in utility or ease of use. Given that it is usually the surgeon who would decide to use the VITOM, this could be a barrier to realizing the real benefits of the device. This also demonstrates a weakness in TAM, which only accounts for individual perceptions, not the perceptions across the team and, thus, may not be entirely predictive. Given that most surgical technologies are used across team members, this may be an important future development of the model.
This was a moderate sized pilot study, using existing subjective measures on a relatively small sample of users and operations. The two-center design, in which one center (CSMC) had prior experience with VITOM while the other center (CNMC) did not, does create some bias in outcomes due to the learning curve of CNMC. While we acknowledge this potential drawback, we believe that this also provides valuable comparisons between more and less experienced team members highlighting the learning curve in using this technology. We cannot therefore draw generalizable conclusions from it, nor did we seek to develop a predictive computational model based on TAM. The effects we observed were relatively small, even though we found many significant differences. We did not evaluate surgeries which did not use VITOM, nor did we study process, teamwork, or outcome directly. These goals would, of course, be both desirable and achievable. Nevertheless, we have demonstrated why the evaluation of new technology in an operating room may not purely be one of clinical outcome or process comparison; how learning curves might impact not only outcomes but also acceptability; how a range of team members might have different perceptions and positive and negative motivations for using a device, and how subjective measurement techniques might be modeled to realize the benefits of user-centered design in surgical care.9–12
This study suggests that there may be small penalties associated with VITOM use, but these reduce with increased experience and benefit both the surgeon and the rest of the team. It also demonstrates how the subjective considerations of utility and usability might influence adoption and could be considered early in the design and testing process, well before the generation of patient outcome data. We recommend a direct comparison of VITOM and non-VITOM cases to explore these findings in more detail and the accelerated application of human-centered design analysis to VITOM and other devices.
Footnotes
Acknowledgments
The authors thank Lori Marum, NP, RNFA for study support and data collection.
P.K.F., A.L.F., and K.C. were responsible for study design. P.K.F., A.L.F., T.D.K., M.P., and Z.C. were responsible for data acquisition. P.K.F., A.L.F., and K.C. were responsible for data analysis and interpretation. K.C. and P.K.F. were responsible for drafting the article. P.K.F., A.L.F., T.D.K., Z.C., and K.C. were responsible for critical review and revision. P.K.F. and K.C. had full access to all of the data in the study and take responsibility for the integrity of the data and accuracy of the data analysis.
Disclosure Statement
P.K.F., A.L.F., and T.D.K. received funding support for this study from Karl Storz Endoscopy, GmbH. P.K.F. has served as a paid consultant of Karl Storz Endoscopy GmbH. A.L.F., T.D.K., Z.C., M.P., and K.C. have no personal financial or institutional interest in the device described in this study nor did they receive any financial compensation or honoraria in performance of this study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.