
Abstract
Abstract
Purpose:
Postoperative pneumothorax and effusion remain a concern following congenital diaphragmatic hernia (CDH) repair. Despite a recent trend away from intraoperative thoracostomy, few studies have actually compared outcomes with and without a chest tube. Rationale commonly cited for the more minimalistic approach include the presumed low likelihood of postoperative complications, potential risk of patch infection, and prolonged intubation. We evaluate these theories, as well as the implications of intraoperative chest tube (IOCT) placement.
Methods:
We performed a retrospective chart review of 174 patients who underwent CDH repair at our academic children's hospital from 2004 to 2015. We compared incidence of clinically significant pleural events between patients who received an IOCT (n = 49) and those who did not (NIOCT, n = 124). We also evaluated time to extubation and rate of patch infections.
Results:
Clinically significant pneumothorax or effusion occurred in 28% of NIOCT patients versus 10% of IOCT patients (P = .01). After thoracoscopic repair, time to extubation averaged 5.2 days in IOCT patients, 5.4 days in NIOCT patients with no postoperative complications, and 6.4 days in NIOCT patients requiring postoperative intervention. After open repair, time to extubation averaged 13.8, 13.6, and 22.5 days, respectively. There were no documented patch infections.
Conclusions:
Chest tube placement during CDH repair is associated with significantly lower incidence of clinically significant pleural complications, does not delay extubation, and results in shorter ventilator times than cases that require postoperative intervention. Patch infections are extremely rare. There is no evidence that chest tube placement increases this risk.
Introduction
C
CDH has historically been repaired through an open procedure with a chest tube left in place. Perioperative management included aggressive hyperventilation with high peak inspiratory pressures, ventilator rates, and O2 concentrations. Studies linking poor outcomes to ventilator barotrauma led to a shift toward gentle ventilation and permissive hypercapnia.4–6 This trend, as well as the onset of minimally invasive surgery (MIS), prompted a decrease in the use of prophylactic intraoperative chest tubes (IOCTs). Reasons commonly cited for choosing not to leave a chest tube are that it is minimally effective, that negative pressure may damage the hypoplastic lung, that increased pain and subsequently decreased respiratory effort will prolong ventilator time, and that it increases the risk of patch infection. 7
As there are few studies examining IOCT placement dedicated to the CDH population, direct comparison of outcomes after CDH repair with and without IOCT placement is warranted. The goal of our study was to evaluate the effect of placing a chest tube on the need for postoperative interventions, time to extubation, and patch infection.
Materials and Methods
We performed a retrospective chart review of all patients (n = 174) who underwent first-time CDH repair at Children's Healthcare of Atlanta (CHOA) from 1/1/2004 to 6/1/2015. To reinforce the diaphragm repair, small intestine submucosa (SIS®, Cook Medical, Bloomington, IN), a porcine extracellular matrix material, was used as a “living scaffold” at the discretion of the attending surgeon. When primary repair was not possible, GORE-TEX® soft tissue patches (Gore Medical, Newark, DE) were used. Following IRB approval, demographic, operative, and postoperative data were collected from electronic medical records from the time of surgery to last follow-up.
The primary outcome was clinically significant pneumothorax or pleural effusion. Given the presence of obligate pneumothorax in a majority of postoperative CDH patients, need for postoperative aspiration or chest tube placement was used to indicate clinically significant pleural events. Patients requiring one of these interventions were evaluated in groups labeled accordingly. In addition, the cohort of patients requiring either aspiration or chest tube was evaluated as a whole. One patient who underwent laparoscopic repair (as opposed to thoracoscopic) was excluded from postoperative intervention analysis. To evaluate the potential drawbacks of leaving a chest tube, secondary outcomes included time to chest tube removal, time to extubation, and incidence of patch infections. As MIS and open repairs are associated with significant differences in ventilator time and length of stay, patients in these two cohorts were evaluated separately. Time to extubation was calculated from the day of surgery to the day of endotracheal tube (ETT) removal, and chest tube time was calculated from day of chest tube insertion to day of chest tube removal.
Patients with severe cardiac or tracheal anomalies, which precluded extubation, were excluded from extubation analysis. The following groups were compared using a Student's t-test: those with an IOCT versus those with no IOCT who required postoperative intervention and those with an IOCT versus those with no IOCT who avoided postoperative intervention. For patch infection analysis, all patients were included. A Student's t-test was used to compare the rate of patch infection between those who never had a chest tube versus those with any perioperative chest tube (placed intraoperatively or postoperatively).
Results
One hundred seventy-four patients were identified who underwent primary CDH repair at CHOA within the specified time frame. Mean follow-up was 2.47 ± 2.5 years. Sixty-three percent of patients were male. Median gestational age was 38 weeks and patients ranged from 1 day to 2 years of age. One hundred fifty-four (89%) were less than 1 month, and 130 (75%) were less than 2 weeks of age. Eighty-seven percent had a Bochdalek hernia, and 74% were left sided. Forty-five percent were performed through thoracoscopic approach, 43% through laparotomy, and 11% through thoracotomy. Patient characteristics and operative data are found in Table 1.
Figures 1 and 2 and Table 2 demonstrate the incidence of clinically significant pneumothorax or pleural effusion as indicated by need for postoperative intervention. In 174 patients, there were 40 clinically significant adverse pleural events: 21 pneumothoraces, 15 pleural effusions, and 4 hydropneumothoraces. The specific indications for the pleural interventions are delineated in Tables 3 and 4. Five of the effusions were chylous. One patient with a tension pneumothorax developed cardiorespiratory failure and required cardiopulmonary resuscitation with epinephrine and bilateral thoracentesis.
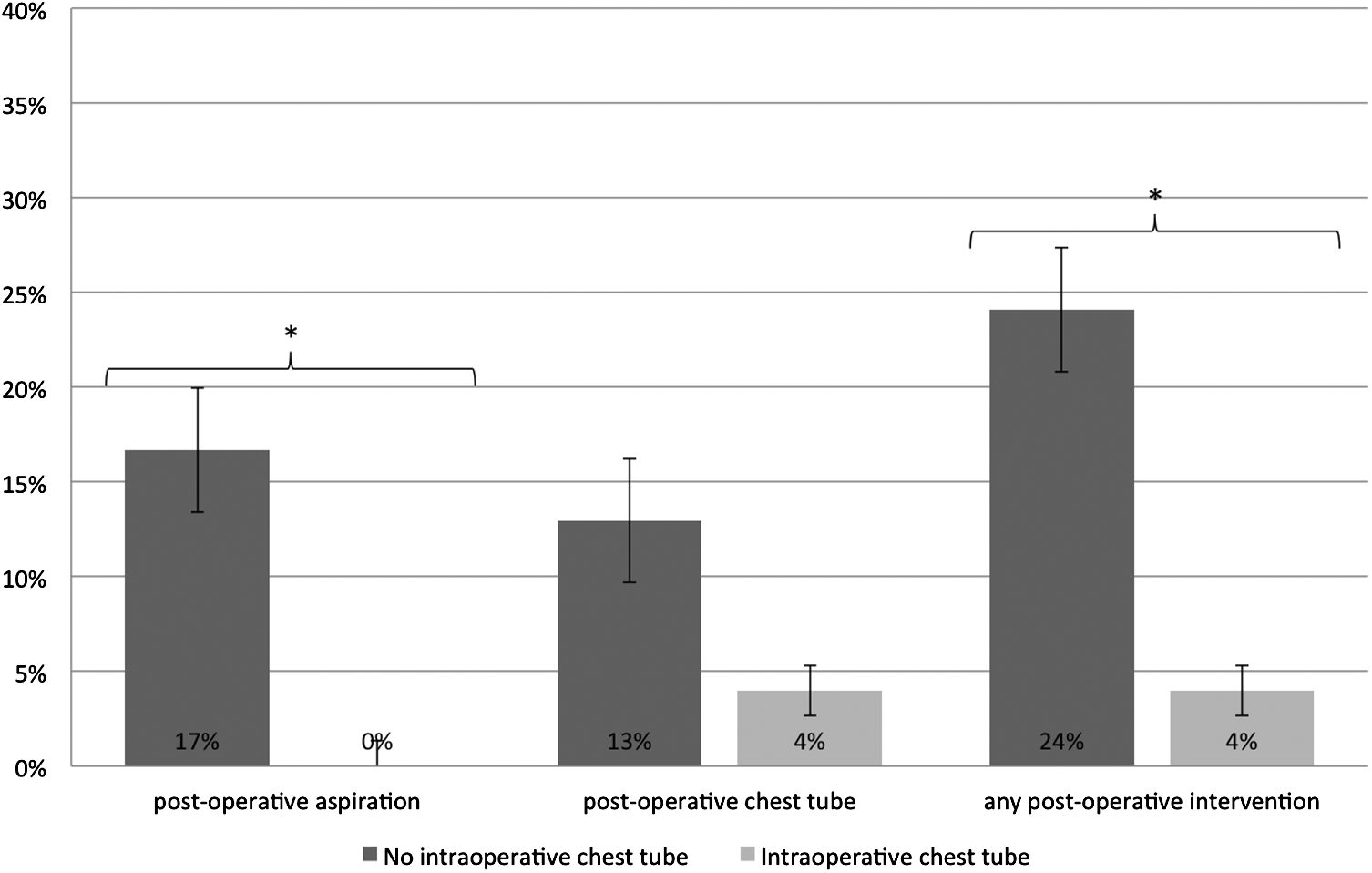
Percentage of patients with clinically significant pleural events following thoracoscopic CDH repair. CDH, congenital diaphragmatic hernia. * designates a statistically significant difference.
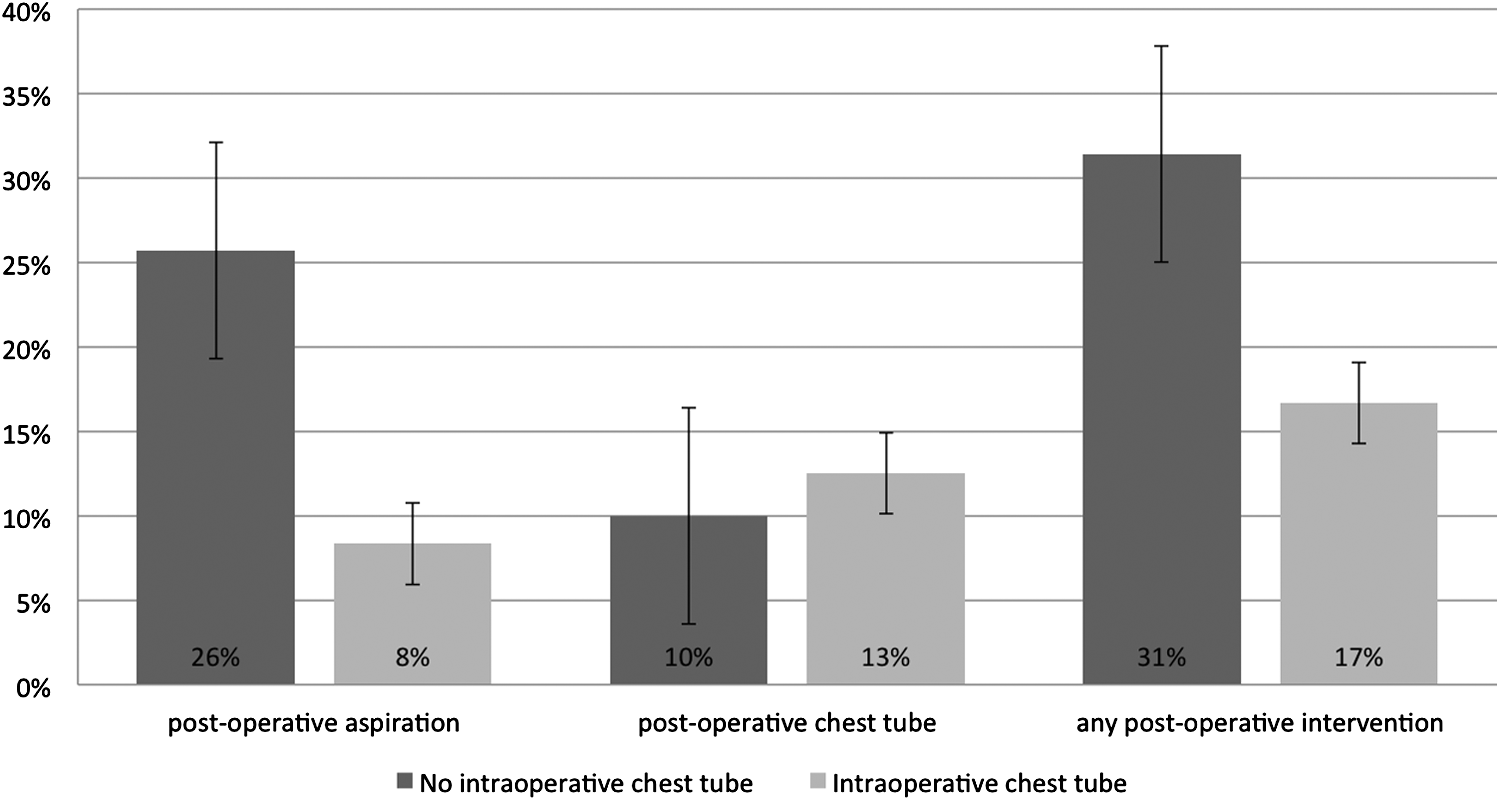
Percentage of patients with clinically significant pleural events following open CDH repair.
When no chest tube was placed intraoperatively, 28.2% of patients required postoperative aspiration, chest tube placement, or both compared to 10.2% of patients in whom a chest tube was left (P = .01). Thoracoscopic cases were more likely to need intervention for pneumothorax, while open cases were more likely to need intervention for an effusion. In thoracoscopic cases, leaving a chest tube decreased the risk of postoperative aspiration, postoperative chest tube placement, and overall intervention rate. In open cases, the incidence of chest tube placement was not decreased. However, for open cases, intraoperative chest tube placement did decrease the rate of aspiration and overall need for intervention.
The length of time chest tubes were left in place is reported in Table 5. In our total patient cohort, chest tubes remained in place for an average of 4.09 days. Time until chest tube removal was similar, regardless of timing of placement or indication.
The time from surgery until extubation is demonstrated in Figures 3 and 4. The following patients were excluded from extubation analysis: 11 patients who died on the ventilator, 3 who became tracheotomy dependent, 8 with severe cardiac defects, 2 with severe tracheomalacia, and 2 for whom we were unable to determine the dates of ETT removal. After thoracoscopic repair, those who did not receive an IOCT, but needed postoperative intervention, were extubated after a mean of 6.4 days, while those with a chest tube placed intraoperatively were extubated after a mean of 5.2 days, although the difference did not reach statistical significance. Even in patients who never received a chest tube, the time to extubation was similar to those with an IOCT at 5.4 days.
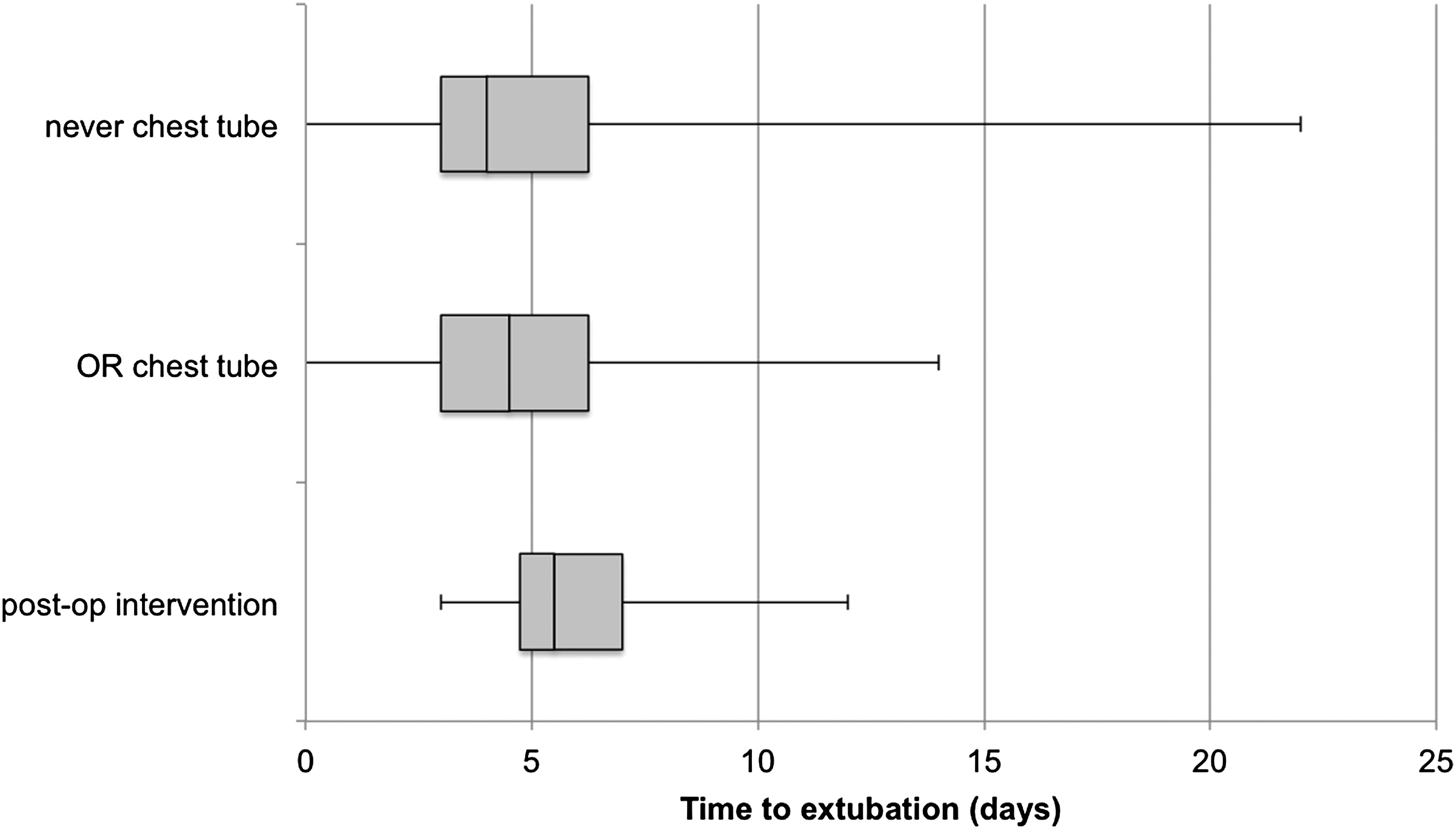
Time from surgery to extubation after thoracoscopic CDH repair. For each group, the boxes represent the second and third quartiles, respectively, within the sample and the horizontal lines represent the first and fourth quartiles of the population (range).
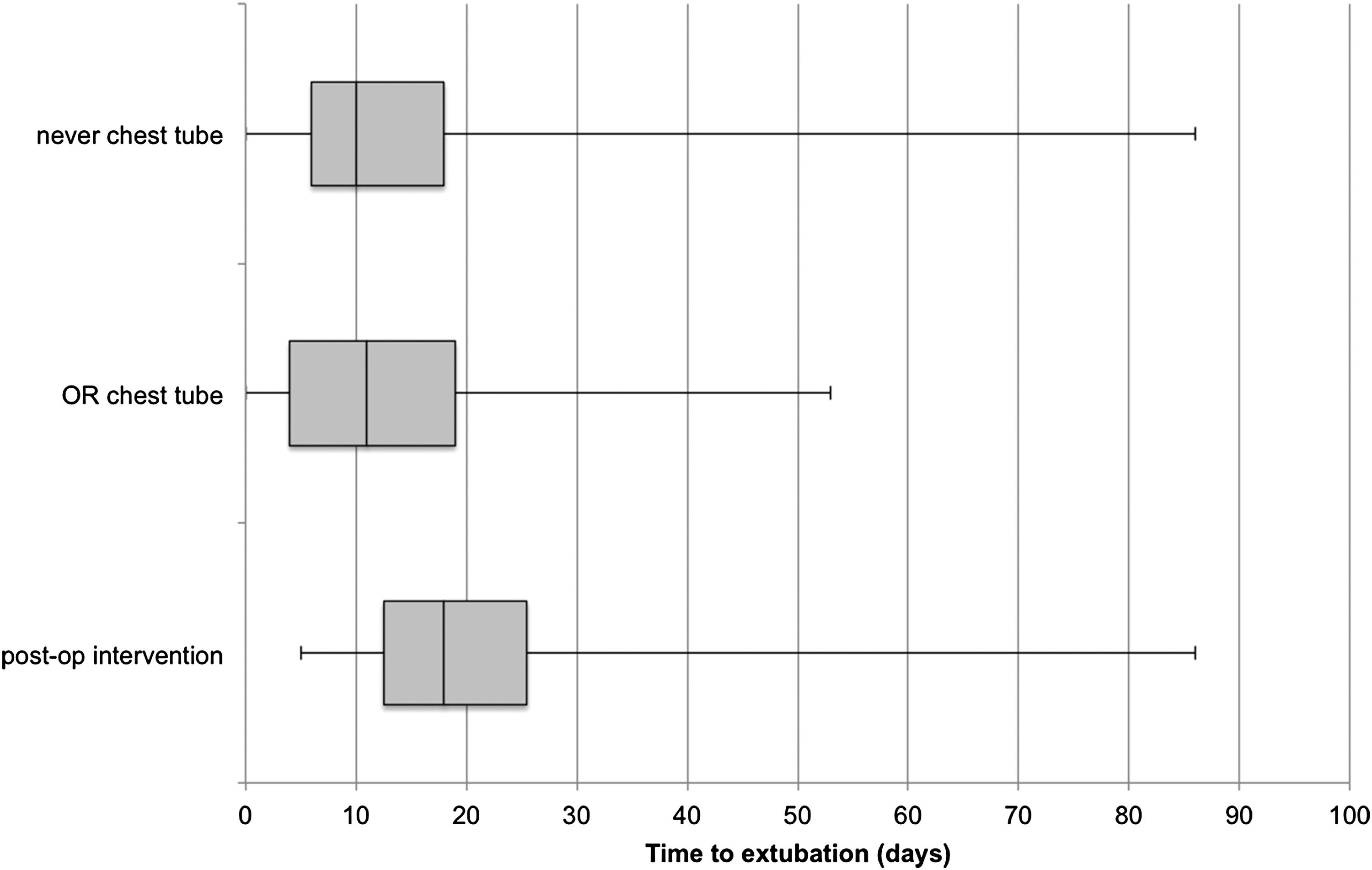
Time from surgery to extubation after open CDH repair. For each group, the boxes represent the second and third quartiles, respectively, within the sample and the horizontal lines represent the first and fourth quartiles of the population (range).
In open cases, patients requiring postoperative intervention were extubated after a mean 22.5 days, compared to a mean 13.8 days in those with an IOCT, although the difference was not statistically significant. In patients who never required a chest tube, the time to extubation was similar to those with an IOCT at 13.6 days.
Incidence of patch infections is reported in Table 6. Sixty-three patients had a perioperative chest tube placed. Of these, 25 patients had a GORE-TEX patch, and SIS was present in 34 (20 had both). Of the 111 patients who never required a chest tube, 52 had a patch and SIS was present in 30 (50 had both). There were no patch infections in any of these patients.
Discussion
The current trend in CDH management is toward less aggressive measures, including decreased use of prophylactic IOCTs. We report the impact of IOCT placement in 174 primary CDH repairs at our facility between 2004 and 2015.
In recent years, many have questioned the need for a chest tube, claiming that it does not make a difference in outcomes. A 2004 comparison of 42 lung biopsy patients with no chest tube versus 34 historical controls with an IOCT demonstrated no difference in need for postoperative chest tube. 8 A 2007 randomized controlled trial (RCT) in 60 lung biopsy patients reported no pneumothoraces in either group. 9 In a 2009 review of 333 thoracoscopic procedures, only 1 pneumothorax was reported, although a majority of the cases were lung biopsies. 7
Frequent pleural complications after CDH repair remain the most compelling reason to leave a chest tube. Obligate postoperative pneumothorax occurs in nearly all infants after repair. Clinically significant pneumothorax, however, has been reported in up to 30% of patients and effusion requiring postoperative drainage in up to 29% of patients in whom no chest tube is left.10–14 Chylothorax occurs in an average of 6% of cases with a higher risk after ECMO use or patch repair.14–16 Pneumothorax, pleural effusion, chylothorax, and need for aspiration have all been associated with increased mortality in the postoperative period.13,14,17
Our data corroborate these studies as 28% of patients with no IOCT had a pleural complication requiring intervention. In addition, we demonstrated that a prophylactic chest tube significantly decreases the need for postoperative intervention to 10% overall. The decrease in adverse events was present in all subsets, but was most marked in the group undergoing thoracoscopic repair. The rate of pneumothorax is higher relative to effusion after MIS compared to open repair. Pneumothorax has high risk for mediastinal shift and sudden deterioration, as occurred in one of our patients, offering further support for considering prophylaxis in thoracoscopic cases in particular.
Another commonly cited reason to avoid chest tubes is that their presence worsens postoperative pain with decreased respiratory effort leading to atelectasis, pneumonia, and extended ventilator time and hospital stay. 7 Watanabe's comparison of lung biopsy patients with and without chest tubes revealed no difference in length of stay, although Luckraz's RCT demonstrated a longer hospital stay in patients with drains.8,9 Our CDH patients with no IOCT who ultimately required postoperative intervention had, on average, one additional ventilator day in comparison with those who received an IOCT. More importantly, patients with a prophylactic chest tube had no difference in ventilator time from those with the best case scenario–no IOCT and no need for postoperative intervention. This indicates that placement of a prophylactic chest tube does not slow the extubation process in this patient population.
Another argument against chest tube insertion is the risk of patch infection associated with foreign material presence. 18 Reports of this complication after CDH repair, however, are rarely found in literature. One retrospective review of 99 patch repairs in 184 cases demonstrated one patch infection, although presence or absence of a pleural drain was not recorded. 19 Other case series examining complications after patch repair record no patch infections, although again, chest tube status is not reported.10,20–24 In our 39 cases with both a chest tube and foreign material in place, there were no patch infections, nor did any occur in the entire 131 patient cohort with patches in place. This low risk of patch infection may mitigate fears when considering placing a small patch to alleviate tension on the repair.
Furthermore, it may be argued that the placement of a chest tube in the sterile operating room environment is far superior to less-sterile intervention placing an emergent chest tube postoperatively. For those concerned that chest tube diminishes the aesthetic appeal of MIS, an operative chest tube uses one of the previous incisions, whereas a postoperative chest tube often gets placed through an additional incision.
Of particular concern in this case series are the outliers. The hospital stay of one patient with no IOCT was complicated by acute respiratory failure requiring CPR and epinephrine secondary to a severe pneumothorax. Patients who developed a chylothorax were intubated for an average of 35 days after surgery and one died on the ventilator. In addition, all 34 patients who required postoperative intervention experienced the trauma of an urgent bedside procedure.
In recognition of the potential morbidity associated with postoperative pneumothorax and pleural effusion, use of a prophylactic chest tube during CDH repair should be revisited. Our study demonstrated decreased incidence of clinically significant pleural events and failed to demonstrate prolonged chest tube time or ventilator time associated with IOCT placement. Patients in our study had a chest tube for an average of 4 days, and almost all were removed before extubation. As several studies have demonstrated the safety of removal within 2 days, we predict that even earlier removal may be possible in the future.25–27 Therefore, as the risks of adverse postoperative events are significant and the detrimental effect of prophylactic placement is minimal, IOCT placement should be considered in conjunction with individual clinical factors in patients undergoing CDH repair.
Limitations
As a nonrandomized study, the decision whether or not to place an IOCT and the selection of operative approach (MIS vs. open) was subject to selection bias, as was the selection of a thoracoscopic versus open approach.
The sample size is limited to a single case series at a single institution and should be compared to data from other facilities and evaluated for generalizability.
Conclusions
IOCT placement during thoracoscopic CDH repair is associated with significantly fewer postoperative interventions for pneumothorax or pleural effusion. Use of an IOCT results in the same average length of time with a chest tube in place as placement of a postoperative chest tube. Patients who receive an IOCT have similar time to extubation as those who never require a chest tube and shorter time to extubation than those who require postoperative intervention. Our facility has had no patch infections associated with chest tubes after synthetic patch or SIS repairs.
Footnotes
Disclosure Statement
No competing financial interests exist.