
Abstract
Abstract
Introduction:
Laparoscopic inguinal hernia repair in children is in evolution. Multiple methods of passing the suture around the peritoneum at the level of the internal inguinal ring exist. Cauterization of the peritoneum at the internal ring is thought to increase scarring and decrease recurrence. We have employed a sutureless, cautery only, laparoscopic single port repair of inguinal hernias and patent processus vaginalis (PPV) in girls.
Methods:
After institutional ethical review was obtained, a retrospective review of sutureless laparoscopic inguinal hernia repairs in girls by 4 surgeons at separate institutions was performed. Patient demographics, intraoperative findings, and postoperative outcomes were recorded and analyzed. The technique involves an umbilical 30° camera and either a separate 3 mm stab incision in the midclavicular line or a 3 mm Maryland grasper placed next to the camera, and the distal most portion of the hernia sac is grasped and pulled into the abdomen and cauterized obliterating the sac.
Results:
Eighty inguinal hernias were repaired using this technique in 67 girls between July 2009 and September 2015. The ages and weights ranged from 1 month to 16 years and from 2 to 69 kg, respectively. There was one conversion to open approach because an incarcerated ovary was too close to the ring. A single umbilical incision was utilized in 85%. Fifty-seven percent patients had hernias on the right whereas 42% had hernias on the left. Of the patients with presumed unilateral hernias, 22 patients were found to have PPV and were treated through the same incisions, 17/22 were found during a contralateral hernia surgery and 5/22 were found incidentally during appendectomy. Average operative time for unilateral and bilateral hernias was 22 minutes (5–38 minutes) and 31 minutes (11–65 minutes), respectively. No patient required a hospital stay because of the hernia repair. At an average of 25 months follow-up (1.6–75 months), there were no recurrences. The only complication was a single lateral port site hernia on a 2 kg, former 24 week postmenstrual age girl before adapting the technique to single-site surgery for all.
Conclusions:
Laparoscopic sutureless inguinal hernia repair is safe and effective in girls of all ages. The single-site modification allows for superior cosmetic result and lower complication profile. The Burnia allows for adequate treatment of unilateral and bilateral inguinal hernias with a single incision in the umbilicus.
Introduction
L
Girls offer a unique opportunity for innovation as the vas is not present and gonadal vessels are safely away from the internal ring. The great care taken to avoid these structures in boys is not a concern in girls. Given this freedom, it was hypothesized that simple inversion of the sac into the peritoneum and cauterization of the sac could provide a safe and effective hernia repair in a girl without the addition of a high ligation with suture or even additional port sites when the laparoscopic instrument is placed through the same skin incision at the umbilicus.
Materials and Methods
After institutional ethics review board approval, a retrospective review of 4 surgeons' experience at four institutions with laparoscopic sutureless inguinal hernia repair in girls was performed. Three institutions were located in Chile and one in the United States. Patient preoperative demographics were recorded as well as intraoperative methods and findings and postoperative outcomes. Statistical methods were used as appropriate (Microsoft Excel 2011, Redmond, WA).
Telephone follow-up to ensure validity of outcomes
Each patient was telephoned from the telephone number associated with her chart. Parents or guardians were asked two questions: (1) Has the patient undergone another surgery since the Burnia and (2) Has she experienced any symptoms of recurrence (bulge, pain, etc. at the site of the hernia or umbilicus).
Surgical procedure for the single-site sutureless laparoscopic inguinal hernia repair
A 3 or 5 mm telescope was placed in the umbilicus through a vertical incision in the umbilical skin. Through the same skin incision (but a different fascial incision), a 3 mm Maryland dissector was placed alongside. The Maryland dissector was used to grasp the distal most portion of the hernia sac (Fig. 1). The sac was inverted and cauterized causing obliteration of the hernia sac (Fig. 2) and allowing for the natural shuttering of the abdominal musculature closing the hernia. The final result is shown in Figure 3. In the event that complete inversion of the sac into the abdomen was impossible, the edges of the sac at the level of the internal ring were fulgurated to an extent that the entire ring was closed. Although this does not allow for the shuttering of the abdominal musculature, the repair relies on the natural postoperative scarring made by the cauterization.

Right inguinal hernia with inverted hernia sac.
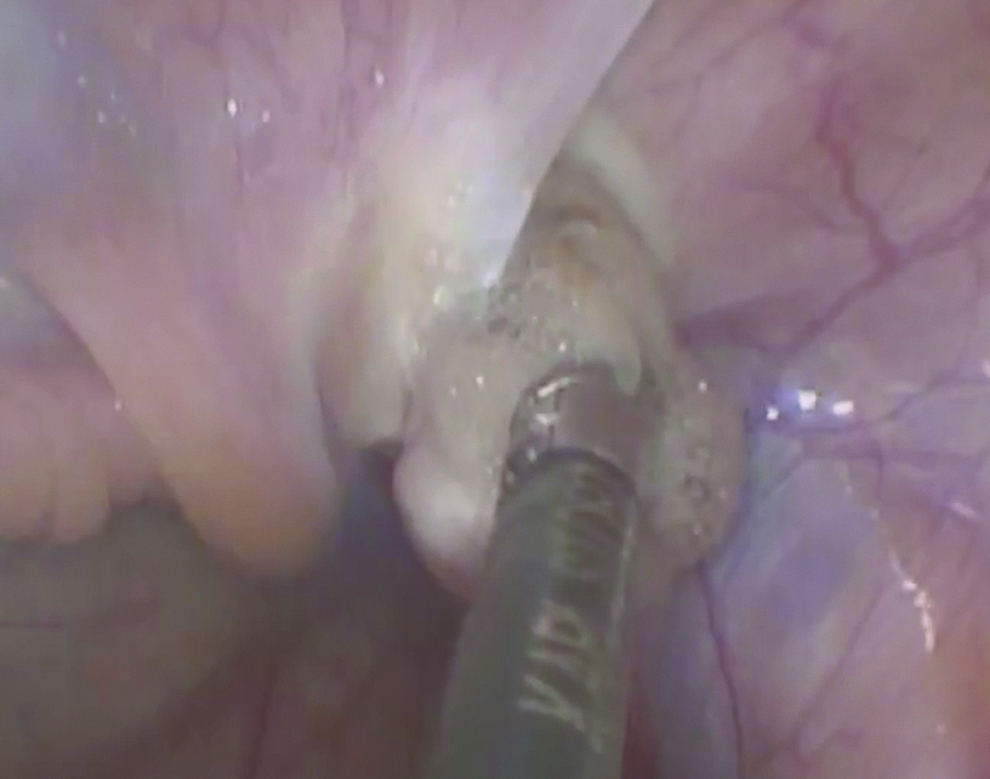
Cautery being applied to the inverted sac.
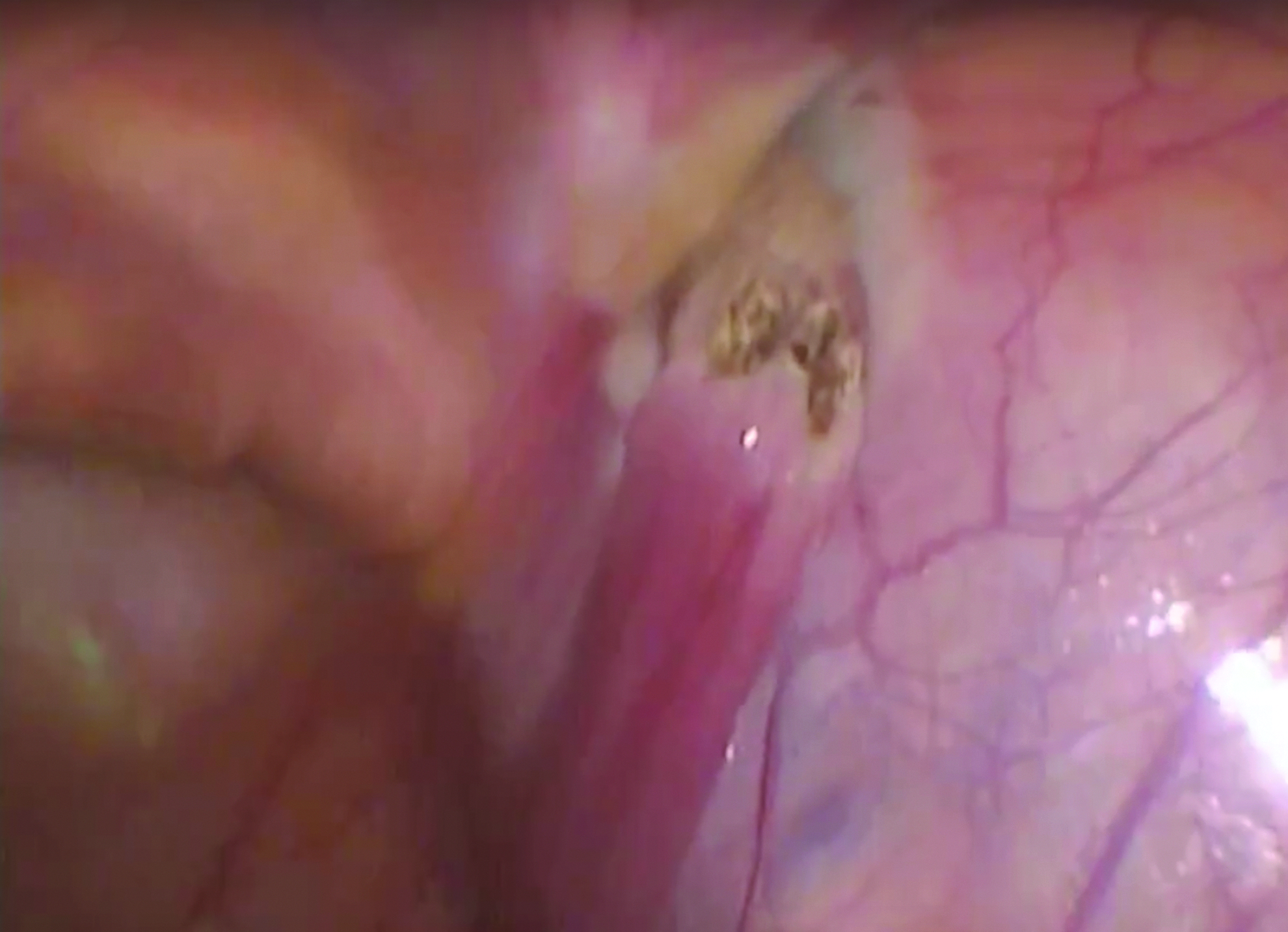
Closed internal ring.
Results
Sixty-seven girls underwent 90 sutureless laparoscopic inguinal hernia repairs between July 2009 and September 2015. Preoperative demographics are listed in Table 1. With one exception, all others were completed laparoscopically without conversion to open. The single conversion was a girl with an incarcerated ovary that after reduction was too close enough to the inguinal ring to have concern of injury. All patients undergoing only hernia repair were discharged on the same day. The group had a mean follow-up of 28 months (1.6–75 months). There were no recurrences.
The average age was 4.4 years old (1 month–16 years). The average weight at the time of surgery was 17 kg (2–69 kg). Four girls weighed 40 kg or more. Seven babies weighed 5 kg or less at the time of surgery. Of the 90 inguinal hernias, 52 were right-sided hernias and 38 were left-sided hernias. including 22 that were bilateral. Comorbidities were rare, though 4 babies were born prematurely, 1 of whom was born at 24 weeks. There was one 13-year-old with heart disease. The rest were healthy.
The average length of surgery was 22 minutes for unilateral (5–38 minutes) and 30 minutes for bilateral hernias (11–68 minutes). A contralateral hernia was found in 30% of girls with a preoperative diagnosis of unilateral hernia. One patient had a preoperative diagnosis of bilateral hernia and only a left inguinal hernia was found. Eleven out of 67 patients (16%) had a documented preexisting umbilical hernia.
All but seven preoperatively known hernias (not incidentally found) were completed through a single incision. Six of these were in the early experience of 1 surgeon and 1 patient was a less than 5 kg girl with bilateral hernias and was the surgeon's preference to utilize a second 3 mm stab incision. There was one port site hernia in the multisite group in a 2 kg girl who was born at 24 weeks postmenstrual age. An additional 7 patients had hernias found incidentally at the time of operation for other pathologies and were treated through the existing incisions. No complications were associated with treating these hernias at the time of appendicitis, diagnostic laparoscopy for abdominal pain, ovarian torsion, or ovarian cystectomy. One patient underwent a subsequent surgery related to her appendicitis and her internal inguinal ring was closed and reperitonealized.
Discussion
Acceptance of laparoscopic hernia repair in children is growing. The technique used is not uniform and many have offered technical enhancements. 7 Unifying themes among the methods of repair are the laparoscopic camera in the umbilical port and typically an extraperitoneal high ligation of the hernia sac at the level of the internal inguinal ring. Some advocate using cautery to encourage scarring at the internal ring after an animal study suggested a decrease in recurrence rate after limited cauterization of the internal ring. 6 Inversion and ligation (typically with an endoloop) of the hernia sac in girls is a common procedure, although it requires a camera port and two working ports.3,8,9 A group in Mexico simply cuts the peritoneum at the level of the internal ring and uses no cautery or suture. 5 The removal of the peritoneal “stent” of the internal ring allows for the natural closure of the inguinal musculature. This technique also utilizes two working ports and a camera port.
Our patients' weights ranged from 2 kg to nearly 70 kg and from 32 weeks postmenstrual age to 16 years of age. This seems to be a tremendously versatile technique that can be applied to a wide range of girls.
Critics of the laparoscopic approach for inguinal hernia repair cite unneeded violation of the peritoneum, concern for higher recurrence rate, longer operative time, and no cosmetic benefit. Proponents of the laparoscopic approach argue that there is minimal disruption of the vas and vessels with the laparoscopic approach in boys, better observation of the contralateral side than through the hernia sac as performed using an open procedure, smaller overall incision length, and the ease of the operation particularly in premature infants.
The additional benefit of the Burnia offers short operative time. A mean of 22 minutes for a unilateral inguinal hernia in teaching hospitals is respectable. If a comorbid umbilical hernia is present, the laparoscopic approach is clearly superior with respect to operative time. Once facile with the technique, the fastest unilateral hernia was accomplished in just 5 minutes and a bilateral in 11 minutes. The simplicity of the case allows for efficiency in operative times.
Moreover, concealing the incision completely in the umbilicus, we believe, does offer cosmetic benefit as there is no opportunity for skin dimpling if the skin were to become adherent to the fascia. Single-site surgery really can be a scarless surgery for a girl with bilateral inguinal hernias and an umbilical hernia.
In this series of 90 inguinal hernias at medium-term follow–up, we had no recurrences of either inguinal or umbilical hernias. This technique both removes the peritoneal stenting of the internal ring and provides cautery to encourage scarring and sealing of the hernia by reperitonealization over the internal ring. Although we will certainly continue to follow these girls, our initial results are encouraging that cautery alone can effectively repair an inguinal hernia in girls.
Our data were retrospectively analyzed and all the weaknesses inherent to that study design are applicable here. In addition, although we have done our due diligence in contacting each patient, we recognize that symptomatic report does not provide 100% sensitivity in revealing recurrence. Weaknesses of the technique include violation of the peritoneum, concern for long-term durability, and a small learning curve for single-incision laparoscopy if the surgeon has not performed single-incision laparoscopy before.
To our knowledge, this is the first published description of a single-site laparoscopic sutureless inguinal hernia repair. We have shown medium-term follow-up to prove durability of the repair and believe it to be safe and effective for girls of all ages.
Footnotes
Disclosure Statement
No competing financial interests exist.