
Abstract
Abstract
Objective:
The aim of this study was to evaluate the feasibility and efficacy of choledochoscopic holmium laser lithotripsy as a means of removing resistant extrahepatic and intrahepatic bile duct stones.
Methods:
Clinical data on 28 patients who had undergone choledochoscopic holmium laser lithotripsy were analyzed.
Results:
Complete stone clearance was obtained in 24 patients; small numbers of residual stones in the left or right hepatic duct were found in 4 patients. No severe complications such as hemobilia and bile duct injuries occurred.
Conclusion:
Choledochoscopic holmium laser lithotripsy is a simple, safe, and effective treatment method for patients with resistant bile duct stones.
Introduction
C
Clinical data
A total of 28 patients—17 males and 11 females of 31–86 years of age (mean age 58 ± 9.55)—were included in the study. All had lengthy histories of chronic abdominal pain; some presented with acute exacerbations accompanied by fever and jaundice. Of all patients, 3 were diagnosed with stones in the left bile duct, 6 with stone in the right bile duct, 4 with stones in the common bile duct, 6 with stones in both the left and right bile ducts, and 9 with stones in both the left and right bile ducts, as well as in the common bile duct. Twelve patients also had stones in the gallbladder. All diagnoses were confirmed by ultrasound, computed tomography (CT), and magnetic resonance cholangiopancreatography before surgery.
Treatment
Twenty-one patients underwent open surgical exploration of the common bile duct; of these, 4 also underwent left hepatectomy; 6 had laparoscopic exploration of the common bile duct; and 3 were operated through a T-tube sinus tract (2 of these patients underwent a second operation). All patients received choledochoscopic holmium laser lithotripsy.
Equipment
1. The Olympus electronic choledochoscope
2. Chinese Mast Family Keruida holmium laser equipment (Mast Family Keruida Laser) or Lumenis PowerSuite 100 W (wavelength 2.1 μm, maximum pulse frequency 20 Hz).
3. Optical fiber (diameter 200 μm).
Procedure
The common bile duct was opened and explored with a laparoscope, and stones were removed using conventional methods such as forceps or flushing. Then the choledochoscope was inserted and the biliary tree explored to determine the location, size, and number of stones, as well as variations of the intrahepatic bile duct anatomy such as abnormal branching and stenosis. In simple cases, stones were removed with a retrieval basket under choledochoscopic view. Where intrahepatic and extrahepatic stones were difficult to remove, holmium laser lithotripsy was used. A laser guidewire was introduced through the working channel of the choledochoscope and extended beyond the end of the scope for 15 mm. Under direct visualization with the endoscope, the guidewire was placed in contact with the stone to fragment it. Laser output power was set to 15 W, and the stones were fragmented repeatedly until they could safely be removed with the basket (generally such stones were ≤5 mm in diameter). Smaller stones of 2–3 mm could generally be flushed out or passed spontaneously.
Results
All 28 patients were treated successfully. The operative time ranged from 45 to 180 minutes (mean 75 ± 28.6 minutes). There were no serious complications such as bile duct injury or bleeding. Postoperative abdominal CT review showed that 24 patients achieved complete clearance and 4 patients had small numbers of residual stones in the left or right hepatic bile duct. Two patients underwent a second holmium laser lithotripsy through a T-tube tract, achieving complete clearance. All patients were followed for 1–28 months (mean 14 ± 3.2 months), reporting no abdominal pain, fever, or jaundice. Postoperative ultrasound and CT follow-up found a recurrence of bile duct stones in 2 patients (Fig. 1).
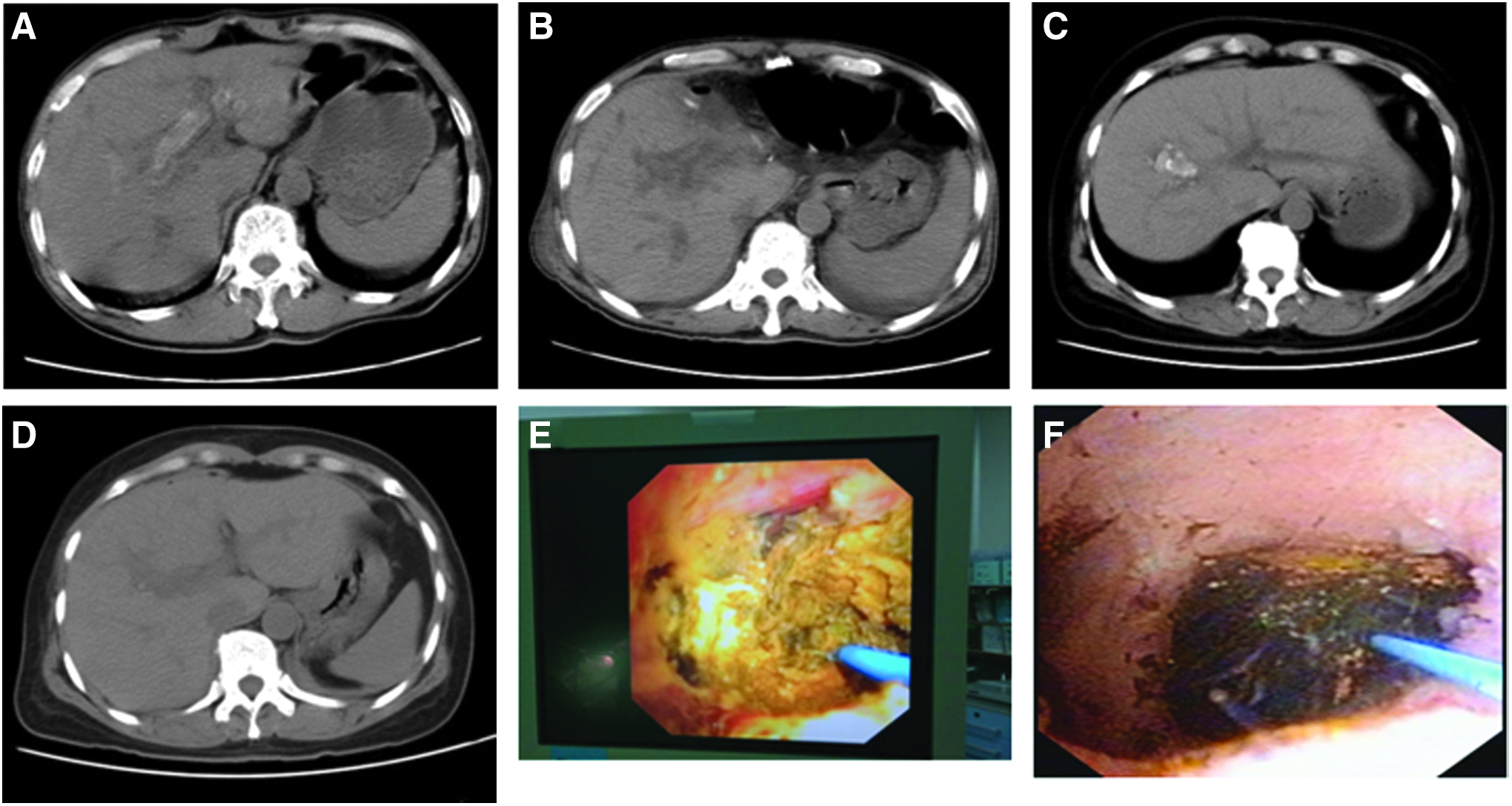
Case 1
Discussion
Gallstone disease includes cholelithiasis, common bile duct stones, and intrahepatic bile duct stones. Statistics shows that the overall incidence of gallstone disease in China is 8.2%, which breaks down as 6.6% stones of the left and/or right bile ducts and gallbladder (cholelithiasis), 0.6% stones of the common bile duct and gallbladder (choledocholithiasis), and 1% both cholelithiasis and choledocholithiasis. Currently, cholelithiasis is treated mainly with laparoscopic cholecystectomy, whereas choledocholithiasis is treated with ERCP. In China, most hospitals will perform liver resection for hepatic stones. In recent years, surgeons have realized that ERCP can cause damage to the duodenal papilla, thus leading to postoperative biliary reflux, cholangitis, the recurrence of gallstones, and so on. In addition, the use of hepatectomy has been limited because it is a highly invasive high-risk procedure that often leaves behind residual stones and may be followed by postoperative complications.
Holmium laser is a relatively new surgical modality, having been invented in the 1990s. It has a wavelength of 2.1 μm, pulsed laser emission time of 0.25 seconds, and instantaneous power up to 10 kW; its energy can vaporize the water between a stone and the end of the inserted fiber, fragment the stone into ashes instantly, and “change a stone into powder with one touch.” Thus, the holmium laser can achieve a high degree of success in clearing stones. In addition, the holmium laser's depth of penetration of human tissue is very shallow, only 0.38 mm, and the pulse duration is only about 0.125 ms, which is far less than the tissue's thermal conduction time (1 ms). In addition, because water absorbs a lot of energy, the holmium laser does only minimal damage to the surrounding tissues while fragmenting the stones. Holmium laser has been commonly used in the treatment of urinary stones and biliary stones in recent years.1–2 Use of the choledochoscope to guide the holmium laser in finding the stones to crush and remove them not only utilizes the intuitive and minimally invasive characteristics of cholangioscopy but also takes advantage of the quick, safe, and effective features of holmium laser lithotripsy. In short, the combined use of holmium laser and cholangioscopy to treat resistant intra- and extrahepatic stones has the advantages of implementing accurate fragmentation, causing less injury, ensuring safety and effectiveness, and promising a quick recovery. On follow-up, we found that none of our patients had any serious complications (e.g., postoperative bile duct injury or bleeding). Postoperative abdominal CT showed complete clearance in 24 patients after a single treatment session. Four patients retained few residual stones; the residual rate overall was 14.2%, which is slightly higher than the rate of 11.2%–78% following liver resection reported in the literature.3–5 All patients were followed for 1–36 months. Only two experienced a recurrence (7.1%), which is less than the reported recurrence rate of 33% post liver resection.6–8
Taking into account a review of the literature 9–10 and our own experience, we believe that choledochoscopic holmium laser lithotripsy is effective in the following situations:
1. Where there is incarceration of hepatic or common bile duct stones, there are cast stones, there is only a small space surrounding the stones or the stones are distant, or where the retrieval basket cannot pass or open.
2. Bile duct stones <1 cm in diameter.
3. Multiple intrahepatic bile duct stones within ducts of grade II and III or above.
4. Stones that could not be removed by other methods, such as ERCP.
The advantages of choledochoscopic holmium laser lithotripsy are as follows:
1. High-efficiency pulverization for cholesterol gallstones, bile pigment stones, and mixed stones regardless of size.
2. Safety, with minimal risk of injury (mainly thermal damage due to poor saline flushing and direct mechanical damage caused by faulty maneuvering); can be used repeatedly if necessary with no additional risk.
3. Can be applied at all levels of the bile duct; is especially effective in higher-level bile ducts of grade II, III, or higher, where the procedure should be done within the field of view to avoid blind maneuvering and equipment damage.
Physicians should pay attention to the following matters:
1. The Olympus electronic choledochoscope was used. In this procedure, the stone is removed through the same channel that is used for saline flushing; this channel's large diameter permits a rapid flow of water and quick removal of both the stone and the heat generated by the laser.
2. Use of ultrasoft fiber (200 μm in diameter) is recommended. The intrahepatic bile duct forms an angle that the fiber must traverse; hence the use of a 500-μm fiber can lead to breakage.
3. The choledochoscope's mirror can be damaged during the process of stone fragmentation; therefore, the end of the fiber end should extend beyond the end of the scope for 15 mm or more. Care should also be taken to avoid placing the end of the fiber between the stones and the bile duct wall, and the angle of scope front should be kept below 30° to enable easy access to the fiber and reduce the risk of breakage.
4. For larger stones, fragmentation can begin at the stone's edges; for small or medium-sized stones, targeting of the center will yield better results. Excitation should be carried out within the field of view to enable careful observation of the stone's puncture depth and fragmentation level.
5. The holmium laser process will generate a lot of bubbles, biliary sludge, and inflammatory secretions from the bile duct wall; application of rapid saline flushing can help to maintain a clear field of view. Each stone should be fragmented to a size that can allow easy removal with the cholangioscope's basket or by flushing it out.
6. Laser output power (ranging from 8 to 10 W) and the number and frequency of pulses can be adjusted during the procedure according to a stone's shape and hardness.
7. Stones <1 cm in diameter can be removed directly using a retrieval basket. When a large residual stone (>1 cm) is suspected or dilation of the common bile duct is obvious, placement of a T-tube (size 24 or 26) is recommended to ensure easier stone removal and a shorter procedure time, both of which can reduce the patient's pain. Stones should be fragmented before removal with the basket, which should be pulled gently to avoid tearing the T-tube and bile ducts, as well as damage to the retrieval basket.
Conclusion
Holmium laser lithotripsy improves the technology of cholangioscopy, greatly reduces the difficulty of stone removal using this modality, achieves maximal stone clearance in a single treatment session, and has the advantages of minimal injury, a quick recovery, and an easy procedure. Thus, it provides an efficient and safe new option for patients with extra- and intrahepatic bile duct stones and is worthy of clinical promotion and application.
Footnotes
Acknowledgments
This study was supported by Taizhou Science and Technology Plan Project (1601KY21), Zhejiang Medical and Health Science and Technology Project of China (2017KY161), and the Zhejiang Natural Fund Project of China (LY17H160069).
Disclosure Statement
No competing financial interests exist.