
Abstract
Abstract
Background:
Sciatic hernia is a very rare pelvic floor hernia, but apparently its incidence has been growing in the past few years. The symptomatology is usually aspecific or absent, but in some cases complications such as intestinal obstruction, intractable pain, or urinary sepsis can occur. The usual treatment is the surgical correction of the defect, mainly with an open approach.
Case Summary:
We describe a case of sciatic hernia causing intermittent abdominal pain and subocclusive symptoms. The hernia has been treated with a laparoscopic technique using a polypropylene extraperitoneal mesh fixed with biological glue. The postoperative course of our patient was uneventful and at 3 months follow-up, no relapse or symptoms occurred.
Conclusion:
The laparoscopic treatment of this rare type of hernia appears to be a feasible and safe surgical option with all the advantages of the mini-invasive technique.
Introduction
S
It is prevalent in females, and the presence of a sudden body mass index (BMI) decrease, a concomitant neoplasia, other hernias, multiparity, or pregnancy are reported as predisposing factors.1,2 The notch of sciatic hernia is the sciatic foramen. The herniation could occur above (suprapiriformis hernia) or below the piriformis muscle (infrapiriformis hernia) or below the sacrospinous ligament (subspinous hernia). 1
Sciatic hernias are unusual findings and often present the physician with diagnostic dilemma.
The clinical presentation is various and in some cases it is absent. The patient could have chronic pelvic pain or intermitting abdominal pain. 3 Commonly the hernia sac can contain ovary and adnexa, small bowel loop, bladder, or colon. If the bowel is compressed or strangulated, the clinical onset can be characterized by intestinal occlusion. In the same way if the ureter is herniated, urinary symptoms can appear. 4 The clinical examination is frequently without any relevant sign but sometimes a lump in the gluteal region can be found. 1 The diagnosis is usually made using a computed tomography (CT) or a magnetic resonance imaging (MRI) or during explorative laparoscopy especially performed in patients who have chronic pelvic pain.3,4
Herein, we present a case of sciatic hernia, occasionally diagnosed on a CT performed for chronic abdominal discomfort, and successfully treated with a laparoscopic preperitoneal approach.
Case Report
A 65-year-old woman came to our attention complaining of chronic intermittent abdominal pain. The pain was increasing in the last months and was often associated with meteorism and nausea. She had a recent change in her bowel habit toward constipation with frequent abdominal distension.
For a certain period, abdominal symptoms were attributed to her concomitant known condition of sigmoid diverticular disease. Another confusing factor was a recent discovery of cholelitiasis that could have probably caused part of her discomfort.
Her medical history was characterized by a mild degree of chronic obstructive pulmonary disease (COPD), arterial hypertension, a previous transient ischemic attack, hypothyroidism, and hemorrhoids. She underwent appendectomy and left inguinal hernia treatment several years before. Her alimentary regimen was normal. Her BMI was 21.
On physical examination, she had moderate pain in the lower abdominal quadrants and active peristalsis, but no palpable hernia in her abdominal wall.
A CT scan of the abdomen confirmed both small gallbladder stones and a mild colon diverticulitis, but also showed an occasional right sciatic hernia (Fig. 1). An MRI was also performed to better investigate the hernia, and it confirmed the presence of a subpiriformis herniation of the right ovary and adnexa with attraction of a small bowel loop. No other pelvic hernias were detected.
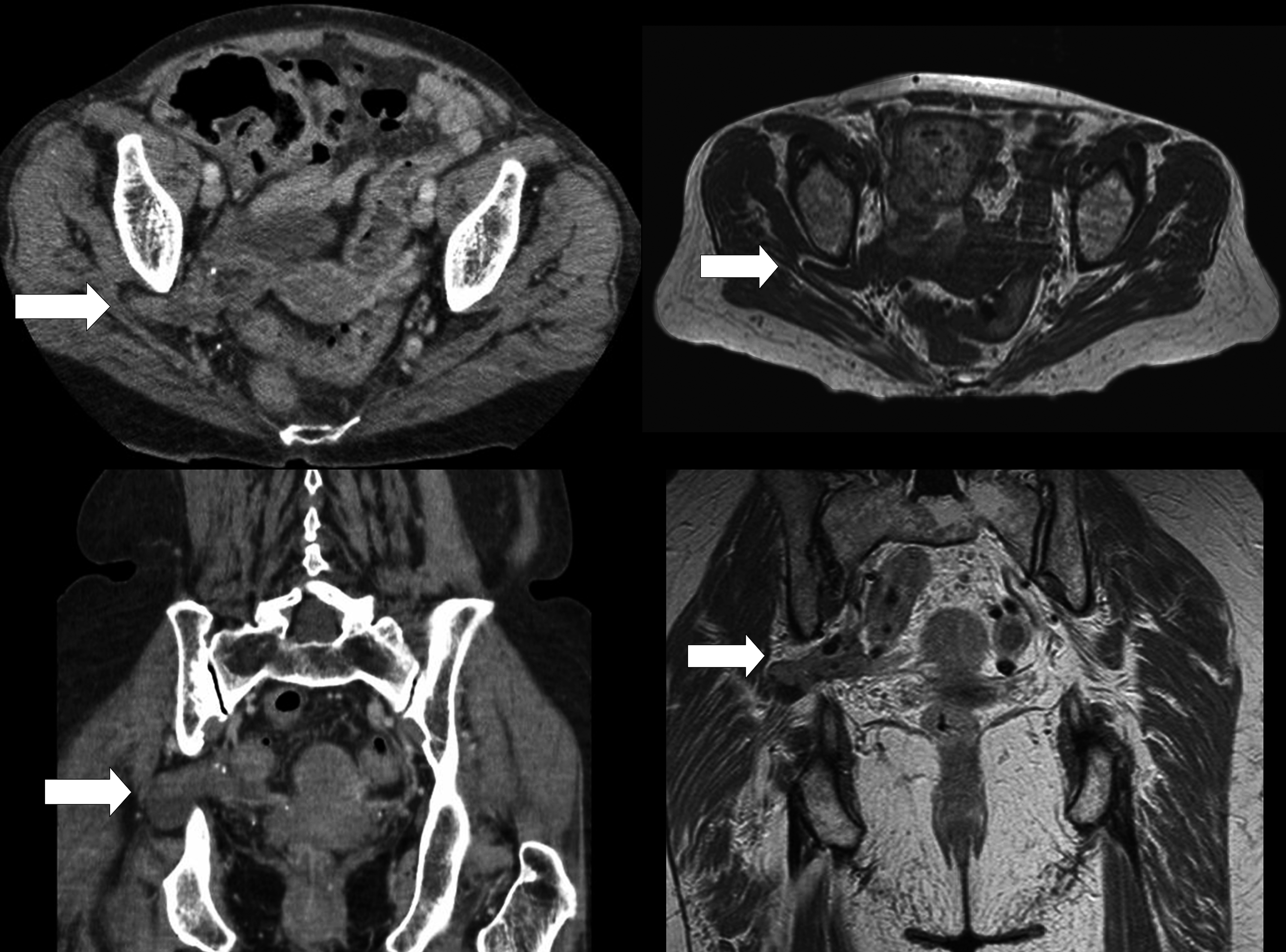
Axial and coronal view of right sciatic hernia at computed tomography scan (left) and magnetic resonance imaging (right). Arrows indicate the herniation of the peritoneum through the right sciatic foramen.
Treatment
A single dose of cefalosporin was administered preoperatively, a Foley catheter was inserted, and the pneumoperitoneum was induced with a Hasson trocar in the periumbilical region. The abdomen was explored using three more trocars (5 mm in epigastrium and right flank; 10 mm in left flank).
A cholecystectomy was performed and one more trocar (5 mm) was placed in the sovrapubic region.
The herniation of the right ovary and the fallopian tube was clearly evident in subpiriformis position through the greater sciatic foramen; the small bowel loop attraction was not confirmed. The hernia was rapidly reduced without any difficulty (Fig. 2). The peritoneum overlying the defect was opened longitudinally to create a peritoneal flap 3–4 cm larger than the perimeter of the defect. A big hernia sac was isolated and reduced respecting the right ureter, the lesser gluteal artery, the pudendal artery, and the branches of sciatic nerve. A polypropylene mesh was shaped (10 × 8 cm) and positioned to cover the preperitoneal space previously prepared, then it was secured with a biological glue (Tisseel®; Baxter) as shown in Figure 3. The peritoneal flap was then closed with a running absorbable suture.
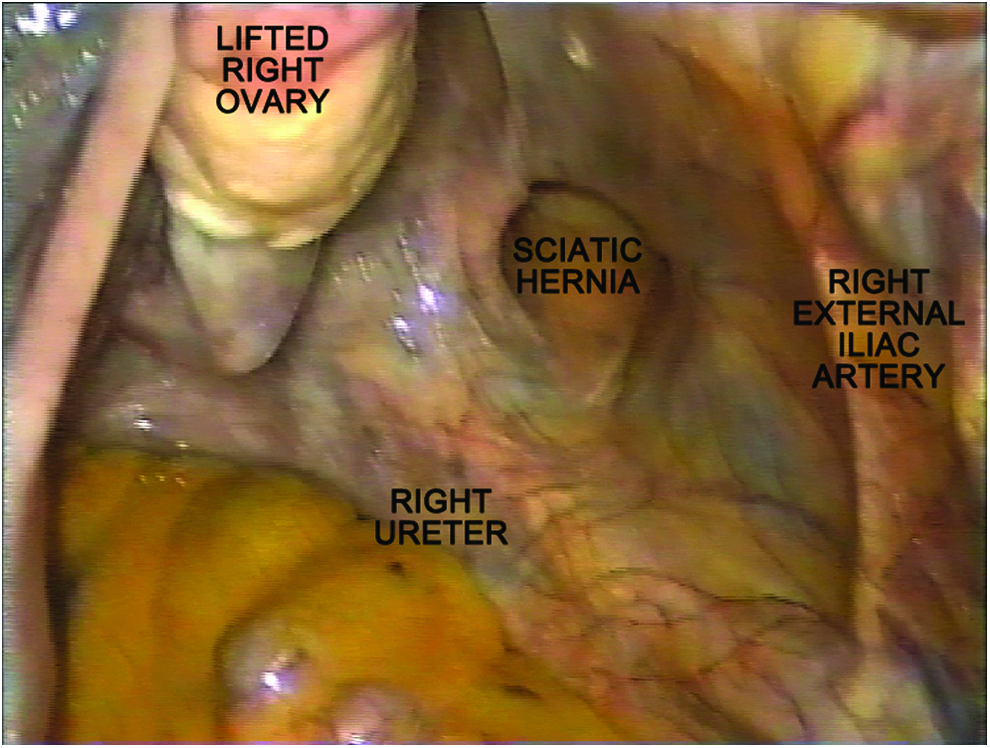
Laparoscopic view of the right sciatic hernia. The right ovary and adnexa were already retracted from the hernia defect.

Polypropylene-shaped mesh (10 × 8 cm) positioned to completely close the hernia defect. The mesh has been fixed with a fibrin sealant (Tisseel®; Baxter).
The postoperative period was uneventful. The patient was discharged from the hospital at third postoperative day in good clinical and general conditions. At 3 months follow-up she was completely asymptomatic.
Discussion
Sciatic hernia is a very rare entity, but its incidence is significantly growing in the past years due to the widespread use of radiological investigations and laparoscopic techniques.1,2
The etiology of sciatic hernia is unclear. Probably a genetic predisposition and an increased space between piriformis muscle and sacrospinous ligaments could be considered two of the most important risk factors. 2 Anyway, as Chaudhuri et al. 4 underlined, the majority of these hernias are supposed to be acquired in origin with chronic raised intraabdominal pressure implicated as a causative factor.
In our case, a history of a previous inguinal hernia could be a clue of a genetic predisposition; old age, pregnancy, and previous appendectomy could lead to some anatomic alterations of the pelvic floor. As for other types of hernias, also high abdominal pressure and malnutrition are risk factors for the development of a sciatic hernia.2,3 Our patient was affected by COPD that could have influenced the abdominal pressure and systemic metabolism favoring the weakening of the osteomuscular components of the pelvis.
Patients are usually women, in many cases they present with pelvic chronic pain, 5 abdominal aspecific pain, 1 or renal colic-like discomfort. 4
In our case, there were no specific symptoms but only a diffuse abdominal pain, probably partially due to diverticular disease. Karasaki et al. 2 tried to answer the question whether it is always necessary to repair a sciatic hernia even if it is asymptomatic; in their experience they assumed that probably a sciatic hernia found incidentally should not be treated, especially in the emergency setting. However, Miklos et al. 5 postulated that it is difficult to demonstrate, but often sciatic hernia can be a cause of chronic intermittent pain and so could be reasonable to close the hernia defect to avoid potential future obstructive symptoms. We decided to repair the hernia defect because our patient had an on–off pain for a long period and it was not easy to attribute the cause of this discomfort.
Repair was historically performed with an open approach: through a midline transabdominal or a transgluteal approach with a direct suture repair1,2,4 or using a prosthetic material. Laparotomy is nowadays helpful in emergency cases (i.e., intestinal or ureteric herniations with occlusion or urinary sepsis),3,4,6 but some authors have reported the feasibility and good outcomes of a laparoscopic approach and repair with a plug or a patch.3,5 Furthermore, the open technique is a real demanding procedure with not always satisfying results. Bernard et al. 3 instead highlighted the excellent observation of this type of hernia with laparoscopy with the possibility to diagnose and repair it easily.
Also Tsuzaka 7 and Witney-Smith 8 confirmed the advantages of the mini-invasive approach to treat this rare condition also in an emergency setting. In fact when the ureter is herniated through the sciatic foramen, the magnification of the laparoscopic view could be really helpful and allow to recognize all the anatomical elements.
Similarly, Singh et al. 9 described a successfully repaired sciatic hernia with a robot-assisted technique during a radical cystectomy.
Nevertheless, until now, in the literature only 20% of the described cases of sciatic hernias are treated with a mini-invasive approach even if in the past few years the number of laparoscopic corrections is increased.1,2 In fact all the reports on laparoscopic treatment of sciatic hernias reaffirmed the benefit for the patients in terms of a faster recovery, less pain, and better cosmetic result.3,7,8
Finally, recent significant progresses in prosthesis materials and laparoscopic equipment, with the possibility to situate and secure the mesh in very deep and uncomfortable positions, have favored an easy and safe treatment also of the more demanding hernias.
In our case, we performed a laparoscopic surgery using the same settings of a total extraperitoneal (transabdominal preperitoneal) inguinal hernia correction showing the good feasibility of this approach. The surgeon has to be aware of the proximity of gluteal arteries, pudendal artery, and sciatic nerve. Also the ureter may be attracted in the notch and could be damaged during the extraperitoneal dissection or during the hernia sac reduction.
Even if some authors believe that a prophylactic surgery for an asymptomatic hernia may not be necessary, 2 we recommend a laparoscopic repair for surgeons who are experienced in laparoscopic hernia correction, in all uncomplicated cases. Indeed, the rate of complications of sciatic hernias, if untreated, is not easily measurable, but not so low and the rate of recurrence after a laparoscopic treatment is lesser than 5%. 1
Footnotes
Acknowledgments
The authors thank all the surgical and medical staff who took care of the patient. All authors report no source of funding for conducting this study.
Consent
Written informed consent was obtained from the patient for publication of this Case Report and any accompanying images.
Authors' Contributions
All the Authors have made substantial contributions to the acquisition of data, analysis, and interpretation of data. All have contributed in drafting the article or revising it critically for the approval of the final submitted version.
Disclosure Statement
No competing financial interests exist.