
Abstract
Abstract
Background:
Robotic surgery was introduced to overcome laparoscopic drawbacks. This study aimed to compare the learning curve of robotic-assisted right colectomy (RRC) versus laparoscopic-assisted right colectomy (LRC) for colon cancer with respect to operative times and perioperative outcomes. In addition, the health-related costs associated with both procedures were analyzed and compared.
Methods:
Between 2012 and 2015, 30 consecutive patients underwent RRC and 50 patients LRC for colon cancer. All procedures were performed by a surgical fellow novice in minimally invasive colorectal surgery. The operative time and the cumulative sum method were used to evaluate the learning curve of RRC versus LRC.
Results:
The mean operative times were 200.5 minutes for RRC and 204.1 minutes for LRC (P = .408) and showed a significant decrease over consecutive procedures (P < .0001). The number of cases necessary to identify a drop in the operative time was 16 for RRC and 25 for LRC. RRC procedures were associated with significantly reduced blood loss (P = .012). Two patients (4%) in the LRC group were converted to laparotomy, whereas no conversion was required in the RRC group. Surgery-related costs were significantly more expensive for RRC, but when combined with the hospitalization-related costs, LRC and RRC did not differ (P = .632).
Conclusions:
Both robotic and laparoscopic operative times decrease rapidly with practice. However, RRC is associated with a faster learning curve than LRC. The simultaneous development of these two minimally invasive approaches appears to be safe and feasible with acceptable health-related costs.
Introduction
H
Among MIS techniques in colorectal surgery, laparoscopy is the most commonly applied. Initially, the implementation of laparoscopy was rather slow, especially for malignant diseases; the lack of formalized training in laparoscopy and the relatively long learning curve4–6 likely represented the main barriers to its adoption, together with general concerns about technical feasibility and oncologic adequacy in certain procedures. 7 More recently, the results of randomized clinical trials, such as the COST, COLOR, and CLASICC trials, have demonstrated that laparoscopic colectomy for cancer is safe and feasible, with long-term oncologic outcomes comparable to those of conventional open surgery.2,8,9 However, laparoscopic surgery still requires a high degree of spatial resolution, dexterity, and technical skill, necessitating a long training period to ensure proficiency and reach a plateau on the learning curve.5,10–14 This may partially explain why, despite the evidence of improved short-term outcomes and equivalent oncologic results, the application of laparoscopic colorectal surgery is still limited.15–18 A French survey estimated that laparoscopy accounted for up to 29% of colorectal cancer surgeries in 2011. 19 These data suggest that after more than 20 years from its introduction, laparoscopy is still reserved for a limited number (less than one third) of surgical cases.
The advent of robotics in colorectal surgery has aimed to overcome the drawbacks of laparoscopy.20,21 The robotic approach appears to offer all of the advantages of MIS, along with greater ease and comfort for the surgeon. 22 The oncologic outcomes of robotic surgery are comparable to those of laparoscopy, but several studies suggest that the former is associated with longer operating times and greater costs.20,23,24 Although the real benefits of robotics remain under investigation, an increasing number of surgical units are equipping themselves with a robotic platform and starting to use it for colorectal procedures. Thus, it seems appropriate to ask whether it is reasonable to adopt this new technique and incorporate it into colorectal surgery training programs. To positively answer this question, robotic colorectal surgery must be proven to be safe, to be associated with results that are comparable to, if not better than, laparoscopy, to have a reasonable learning curve, and to be cost-effective. Moreover, to support its widespread application, the skills that surgeons would gain during training for robotics would be ideally transferable to other possible developments in minimally invasive colorectal surgery.
This study aimed to compare the learning curve for a single surgical fellow in robotic-assisted right colectomy (RRC) versus laparoscopic-assisted right colectomy (LRC) for colon cancer and assess the health-related costs of robotic surgery compared to laparoscopy.
Materials and Methods
Study design
Between November 2012 and December 2015, 50 consecutive patients underwent LRC and 30 consecutive patients underwent RRC for colon cancer at Henri Mondor Hospital of Créteil (France). All procedures were performed by a surgical fellow (NdeA), who, at the time of the study, was autonomous in general MIS training (>75 hands-on laparoscopic cholecystectomies/appendectomies) and had assisted in >50 laparoscopic colectomies. He had also attended training courses and simulations in robotic surgery. However, the fellow was at the beginning of his learning curve for the LRC and RRC procedures.
In the surgical unit of the Henri Mondor Hospital of Créteil, there is a senior surgeon (F.B.) who is highly experienced in laparoscopic and robotic colorectal surgery (>10 years of experience). He works with fellows and provides a team approach in MIS colorectal surgery. For this study, the senior surgeon supervised the surgical fellow in all procedures. The study was conducted in accordance with the ethical principles ascertained in the Declaration of Helsinki.
Study population
All consecutive patients with right colon cancer requiring surgical resection were eligible for inclusion in the study. The decision on which approach, laparoscopic or robotic, to use was based on the patient's choice and the availability of the robotic platform, in the absence of any clinical contraindications. Both laparoscopic and robotic surgeries were not associated with extra costs for the patient, for whom both procedures were completely covered by the national insurance system.
Demographic data, intraoperative findings, operative variables, postoperative parameters, and morbidities were prospectively entered into the colorectal database of the surgical unit. To ensure patient safety and oncological clearance, bulky tumors (e.g., AJCC, cT4a, or cT4b) were not resected by the surgical fellow and were thus excluded from the study analysis.
Surgical techniques
The preoperative preparations, operative steps, instrumentation, and postoperative care were standardized. All patients underwent a preoperative evaluation, including a physical examination, colonoscopy with tumor biopsy, and total body computed tomography (CT) scan with contrast enhancement. In cases of suspected lymphatic packets, positron emission tomography with lymphatic biomarkers was performed for preoperative staging. Preoperative laboratory data included complete blood cell count, biochemical profile, and tumor markers (carcinoembryonic antigen, CEA). Intravenous antibiotic prophylaxis was administered according to the guidelines of the infection control committee of the hospital.
Laparoscopic-assisted right colectomy was performed as previously reported.25–28 In brief, four laparoscopic ports were placed as follows: a 12-mm umbilical port with a camera and 30 degree telescope, a 12-mm left lumbar port with pararectal port (right hand working), a 5-mm right lumbar port with pararectal port (assistant hand working), and a 5-mm suprapubic port (left hand working). LCR was approached from medial to lateral. First, the resectability of the mass was assessed. Then, the transverse colon was lifted up, and the C of the duodenum was identified. On the inferior side of the duodenum, an incision over the peritoneum was made with a Harmonic Ace (Ethicon Endosurgery, Cincinnati, US). A gauze piece was passed, and CO2 was insufflated to dissect the duodenum and prevent operative injury. For cancer of the cecum, the ileocolic and right branches of the middle colic vessels were clipped proximally and on the specimen side and divided with the Harmonic Ace. All fibrofatty tissue and lymph nodes were dissected toward the specimen. Usually, only the right branch of the middle colic vessels was clipped. The entire middle colic vessel was divided for right colon cancer near the hepatic flexure or in the transverse colon. The mesentery was divided completely from colon to cecum with the Harmonic Ace (Ethicon). Then, along the white line of Toldt, the entire right colon was mobilized up to the mid-transverse level. The resection and anastomoses were performed extracorporeally by delivering the colon and enlarging the umbilical trocar incision (up to 5 cm). Extracorporeal side-to-side anastomoses were carried out using Linear Staplers (Ethicon). On either side of the tumor, the resectional margin of the colon should have been at least 5 cm. All ports and incisions were closed with Vicryl and Ethilon sutures.
Robotic-assisted right colectomy was performed with the robot docked on the right side of the patient, whereas the bedside assistant and the scrub nurse were situated to the patient's left side. Port placement for the robotic procedure closely resembled the port configuration for laparoscopic right hemicolectomy. Three robotic working arms were used, along with a camera (Fig. 1). One assistant laparoscopic port was added for additional retraction, as well as an endostapler. The main surgical steps were the same as those of the laparoscopic-assisted right colectomy, always using a medial to lateral approach. In some cases, energy devices (EndoWrist® Vessel Sealer) were used.
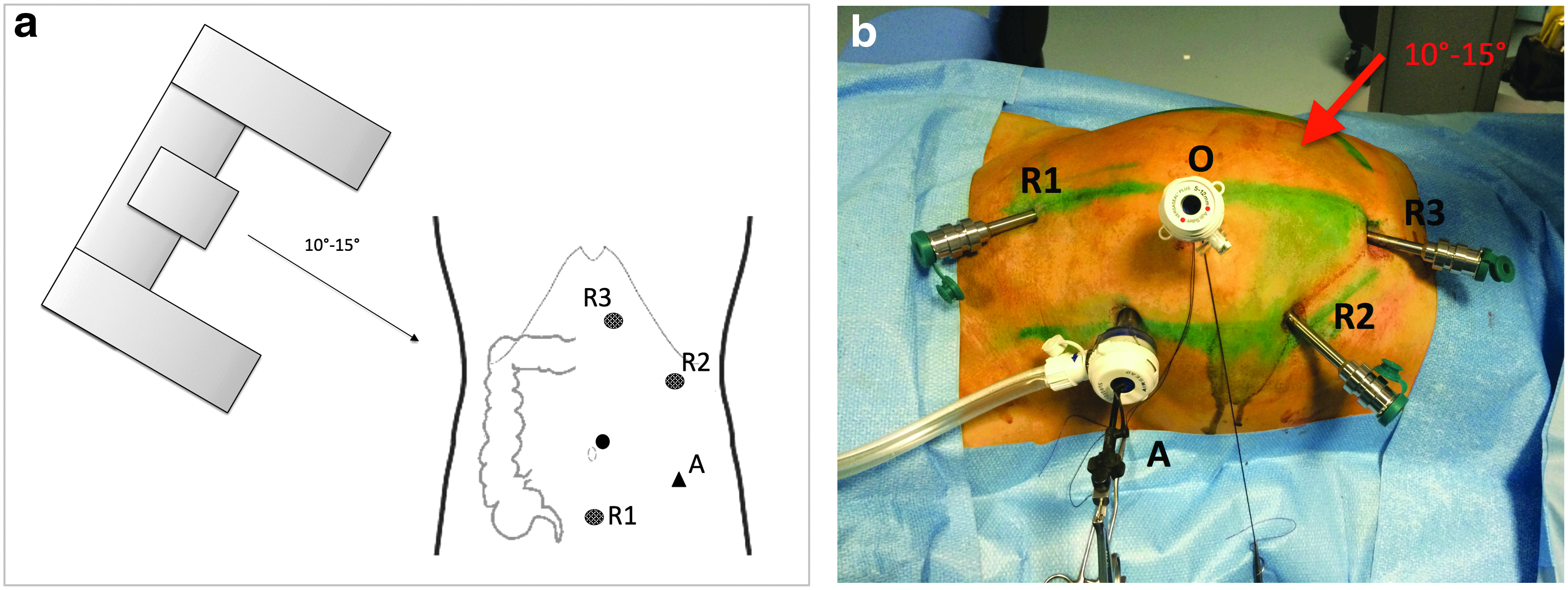
Robotic port placement and docking.
Postoperative assessment
Postoperatively, diets were resumed as soon as bowel function returned clinically. Patients were discharged when they tolerated a normal diet and regained ambulation. Patients were regarded to be suffering from prolonged ileus if they were unable to resume a normal diet after postoperative day 4 and required parenteral nutrition supplementation. Once discharged, all patients were followed every 3 months for the first 3 years and every 6 months thereafter (French Guidelines from the Thesaurus National de Cancerologie Digestive, 2011). At the follow-up visits, a physical examination, CT, and serum chemistry analysis were performed. Colonoscopy was carried out if abnormalities were detected during any follow-up visit.
Outcome measures
Operative time was measured from skin incision to completion of wound closure. For robotic-assisted procedures, docking time (i.e., the time required to position the robot and secure the robotic arms to the corresponding postsites) was calculated separately from operative time. Surgeon console time was the actual time that the surgeon spent at the robotic console during the procedure, and it was also calculated for RRC. Mean operative time was used as the main outcome variable to plot the learning curve.
Conversion was defined as the shift from the laparoscopic to the open approach or from the robotic to the laparoscopic or open approach to complete the procedure. Postoperative morbidity and mortality were defined as events occurring during the hospital stay or within 90 days after resection. Postoperative complications were categorized by the Dindo-Clavien classification. 29 All complications were assessed by a clinician and prospectively registered in the databases at discharge or during the first outpatient visit. Morbidities included postoperative medical and surgical complications such as cardiopulmonary disease, urinary infections, intra-abdominal abscess, anastomotic leakage, prolonged ileus, anastomotic hemorrhage, and reoperation. Oncological outcomes included the quality of surgical resection (i.e., R0, R1) and the number of lymph nodes harvested. R0 resection was defined as macroscopic complete removal of the tumor with microscopic-free resection margins and no peritoneal spread.
Statistical analyses
To evaluate the surgeon's learning curve in laparoscopic and robotic-assisted right colectomy, all consecutive cases were ordered chronologically from the earliest to the latest date of surgery. The RRC and LRC groups were divided into three subgroups of patients in chronological order without the presence of any other obvious grouping criteria. Cases 1 to 10 were grouped, cases 11 to 20 were grouped, and cases 21 and above were grouped.
The cumulative sum (CUSUM) technique was used for quantitative assessment of the learning curve.22,30 The CUSUM is the running total of the differences between individual data points and the mean of all data points. The CUSUM technique used for the 30 RRC cases and the 50 LRC cases was based on the operative time.
Cost analysis was carried out by calculating the total cost per patient, which included the surgery-related costs (e.g., costs of anesthesia, consumables, and instruments) and those of the hospitalization (e.g., days of hospital stay).
Demographic data, operative outcomes, complications, and costs were compared between the RRC and LRC groups by Pearson's chi-squared test, Fisher's exact test, and the Mann-Whitney U-test. Within-group differences (by comparing the three subgroups of patients) were assessed by analysis of variance (ANOVA) calculations. Significant differences were defined as P < .05. Statistics were calculated with SPSS (Statistical Package for Social Science, IBM SPSS Statistics, Version 23 for Macintosh; IBM Corp., Armonk, NY).
Results
Data summarizing the demographic and preoperative variables are shown in Table 1. LRC and RRC did not differ significantly in any of the considered variables. The absence of between-group differences was observed when comparing the LRC and RRC groups, as well as when comparing the LRC and RRC subgroups by cases 1–10, cases 11–20, and cases 21 and above.
No statistically significant differences were noted between the LRC and RRC groups in this subset of consecutive cases.
AJCC, American Joint Committee on Cancer; ASA, American Society of Anesthesiology; BMI, body mass index; LRC, laparoscopic-assisted right colectomy; RRC, robotic-assisted right colectomy; TNM, tumor node and metastasis score.
Data summarizing the operative and postoperative outcomes of the LRC and RRC groups are displayed in Table 2. For the entire sample, the RRC procedure was associated with significantly reduced blood loss (P = .012). The mean operative time was 204.1 (26.7) minutes for the LRC procedure and 200.5 (29.5) minutes for the RRC procedures (P = .408). By subgroup analysis, the LRC and RRC groups showed a trend toward a significant difference in only the 11–20 case series, in favor of RRC (P = .07). No differences were observed between the other two series of procedures.
No statistically significant differences were noted between the LRC and RRC groups in this subset of consecutive cases, if not otherwise specified.
Trend toward statistically significant difference between LRC and RRC (P = .07).
Statistically significant values are shown in italics.
LRC, laparoscopic-assisted right colectomy; NA, not applicable; RRC, robotic-assisted right colectomy.
Two patients (4%) in the LRC group were converted to laparotomy due to technical difficulties related to bleeding during right colic artery dissection and inadequate views. No conversion was required in the RRC group. The LRC and RRC groups did not differ in the other considered variables, either in the whole-group analysis or by subgroup. Overall, 10 (20%) patients in the LRC group and 4 (13.2%) patients in the RRC group developed postoperative complications, including ileus (1), anastomotic leakage (2), intra-abdominal abscess (1), cardiopulmonary disease (10), and urinary tract infection (3). Two of the patients (4%) in the LRC group were classified as Dindo-Clavien grade IV and underwent reoperation (one by laparoscopy, one by laparotomy) for anastomotic leakage. Both patients underwent stoma diversion and peritoneal lavage.
In the RRC group, one patient who was recovering well died suddenly on postoperative day 3 (suicide). The 90-day mortality was zero. The mean length of hospital stay was 8.2 (4.4) days for LRC and 7.1 (3.1) days for RRC (P = .133).
Data summarizing the histological findings are shown in Table 3. No group difference was observed for any variable considered in either the entire sample or the subgroup analyses.
No statistically significant differences were noted between the LRC and RRC groups in this subset of consecutive cases, if not otherwise specified.
LRC, laparoscopic-assisted right colectomy; RRC, robotic-assisted right colectomy.
In the evaluation of the learning curve and progression of the operating surgeon over chronological cases, the operative time showed a significant reduction over consecutive LRC and RRC procedures (ANOVA, for LRC P < .0001; for RRC P < .0001) (Fig. 2). More specifically, in the LRC group, a significant difference was observed between the 1–10 case series and the 11–20 case series (P = .002), between the 1–10 case series and the 21+ case series (P < .0001), and between the 11–20 case series and the 21+ case series (P < .0001). In the RRC group, a significant difference was observed between the 1–10 case series and the 11–20 case series (P = .002) and between the 1–10 case series and the 21+ case series (P < .0001), whereas no difference was observed between the 11–20 case series and the 21+ case series (P = .174). The curves plotted in Figure 2 show a drop in the operative time (≤ 170 minutes) after 31 cases of LRC and 16 cases of RRC.
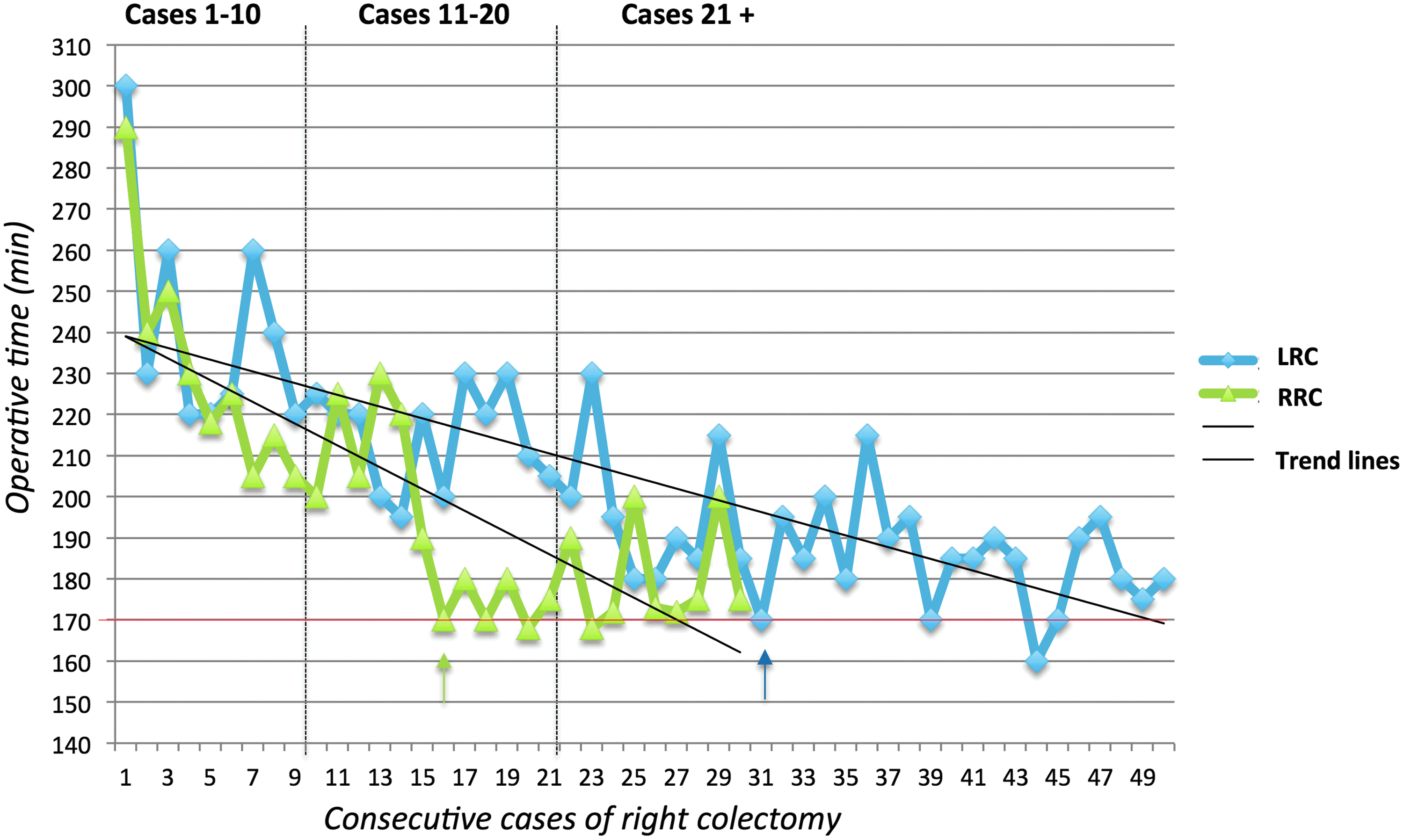
Plots of operative time for LRC (blue line) and RRC (green line) by consecutive patients, with the respective trend lines. A decrease in the operative time (≤ 170 minutes, red line) was observed after 31 cases of LRC (blue arrow) and 16 cases of RRC (green arrow).
Concerning the robotic procedure, a progressive decrease in the operative time over consecutive RRC cases was also observed for the docking and surgeon console times (both P < .0001) (Fig. 3). The CUSUM analyses are displayed in Figure 4 for the LRC and RRC procedures. As shown, the number of necessary cases to identify a change in the operative time (i.e., inverted yield curve) was set at 25 for LRC and 16 for RRC.
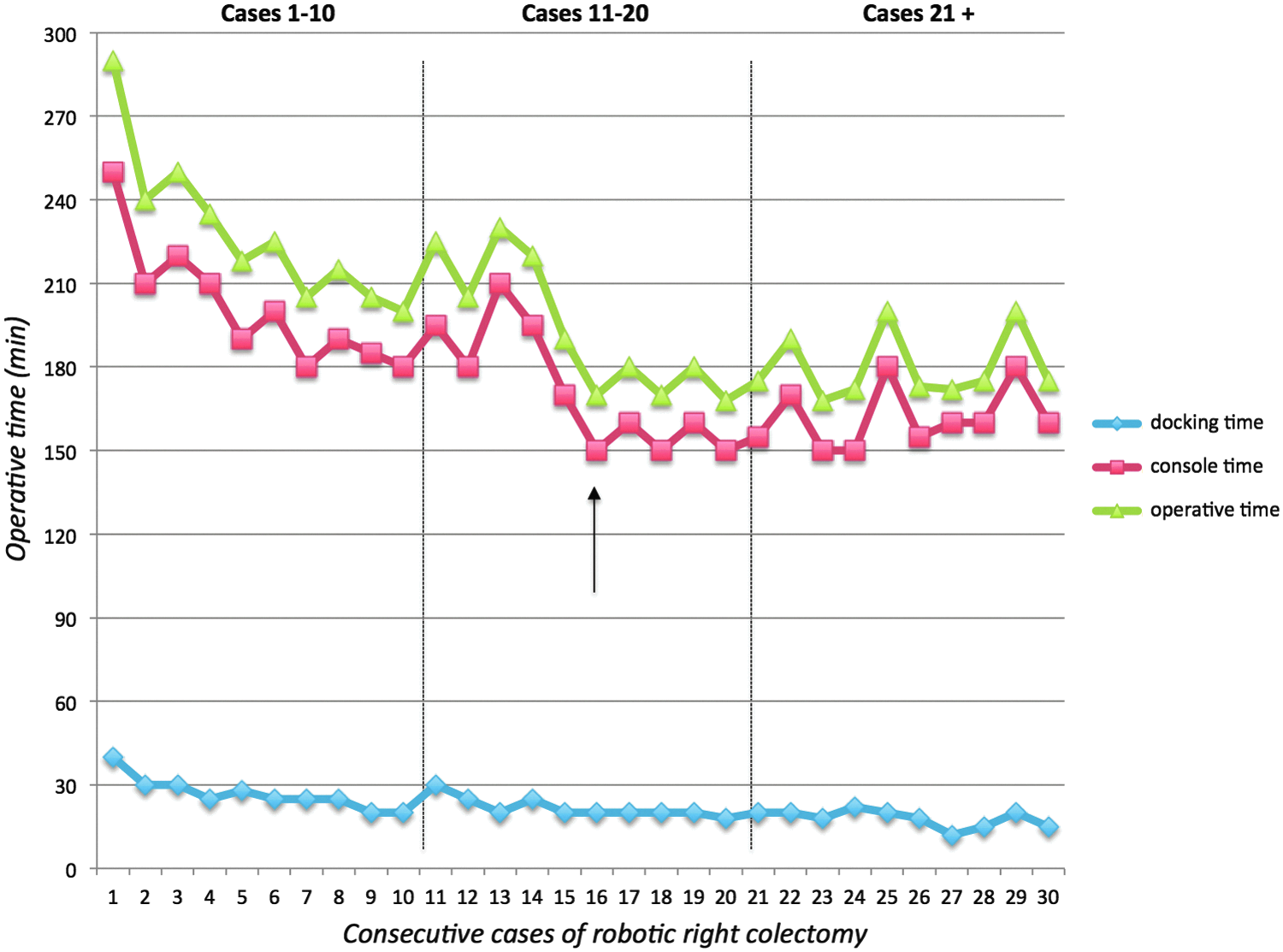
Plot of operative time (green line), surgeon console time (red line), and docking time (blue line) of RRC by consecutive patients. A decrease in the operative time and console time was observed after 16 RRC cases (black arrow).
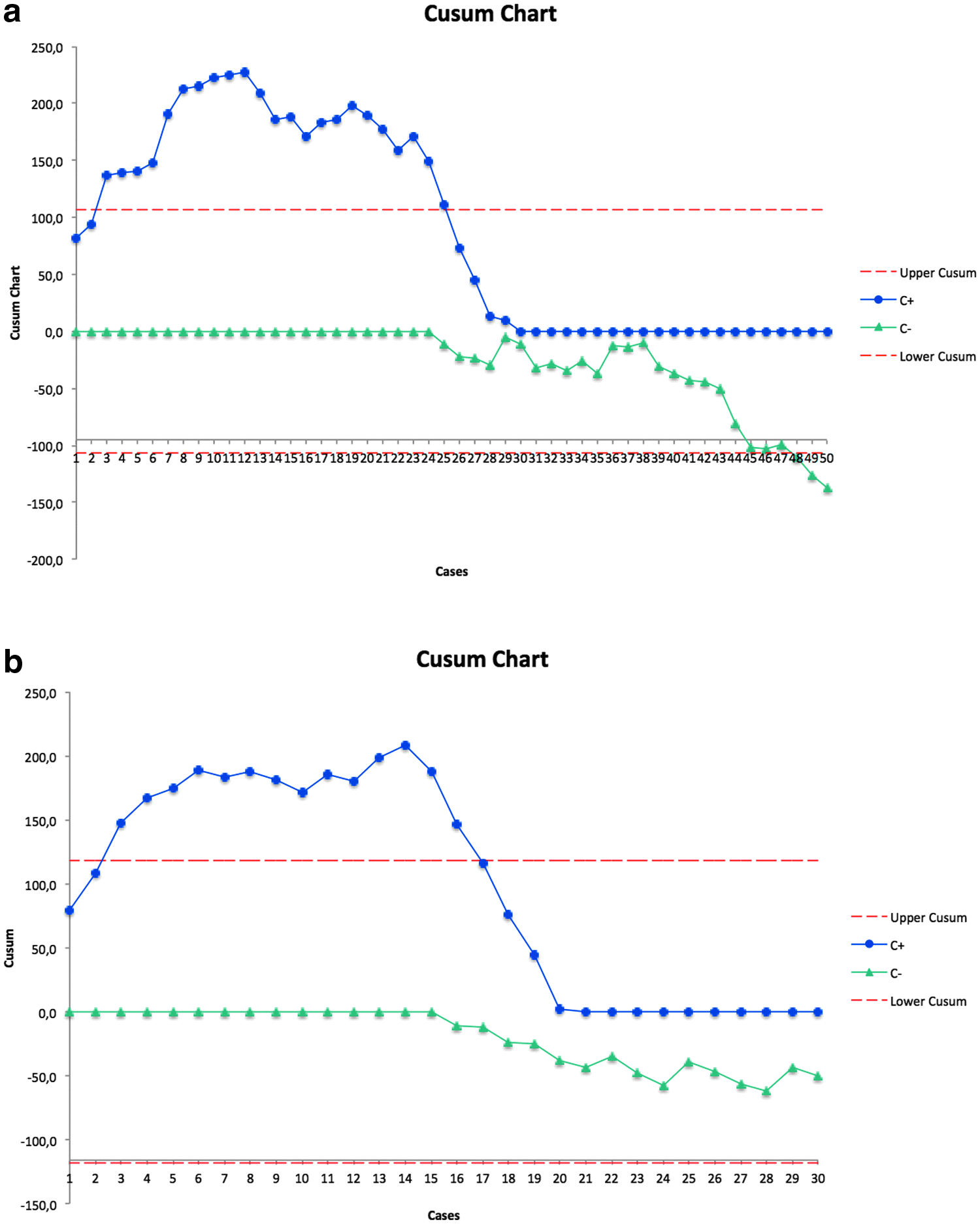
Cumulative sum analysis of LRC and RRC procedures. An inverse yield curve in the operative time is observed after 25 LRC procedures
In the healthcare cost analysis, the surgery-related costs of the LRC procedure were significantly less expensive than those of the RRC procedure, with a mean cost of 1800 (90.9) euros for the LRC compared to 2990 (298) euros for the RRC (P < .0001). However, when the surgery-related costs were combined with the hospitalization-related costs (estimated at ∼1300 euros per day), the LRC and RRC procedures did not differ significantly (P = .632). Overall, the average cost (surgery + hospitalization costs) of a right colectomy procedure was 12,400 (5180) euros (Fig. 5).
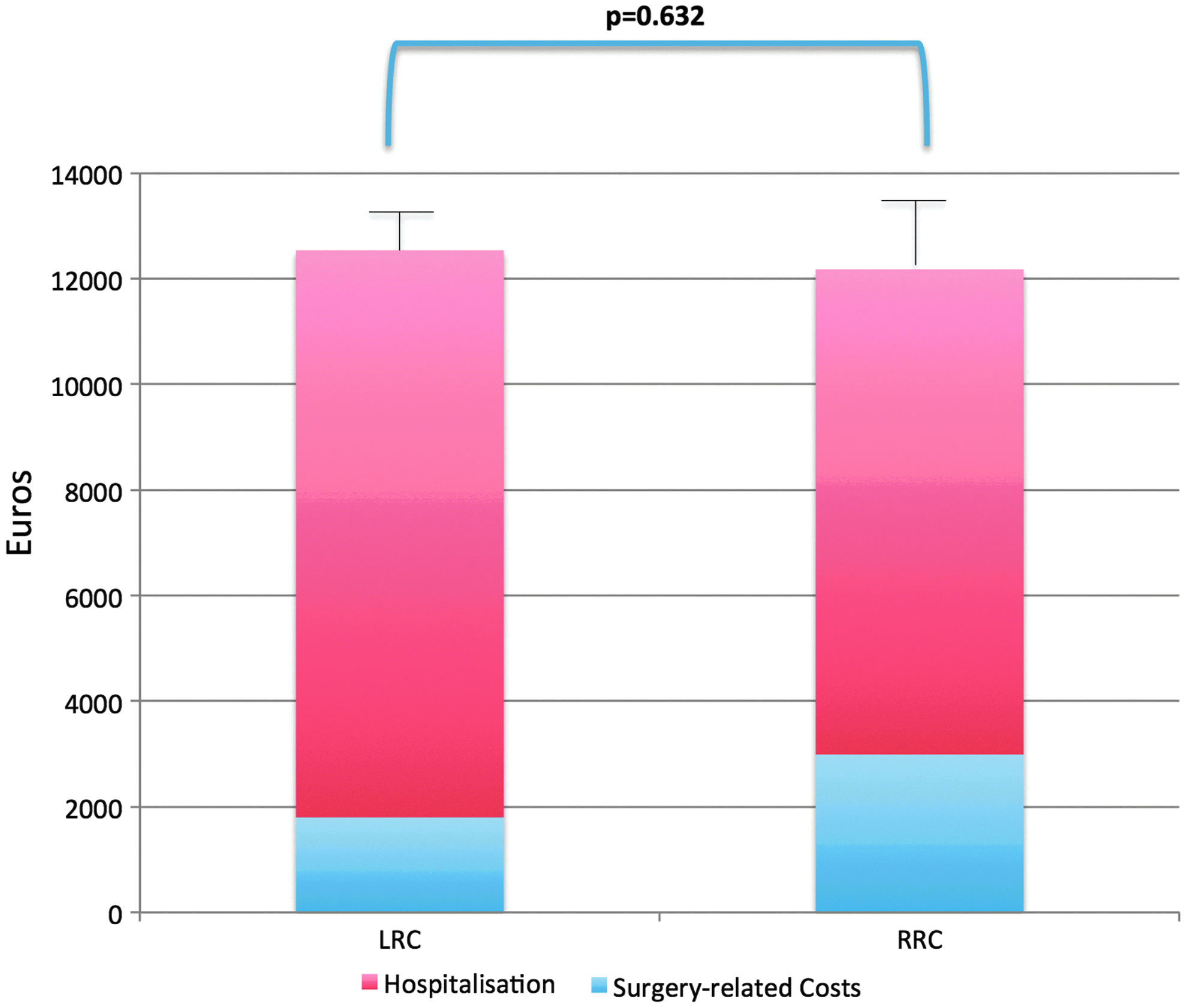
Healthcare cost analysis for LRC and RRC by taking into account the surgery-related costs and the hospitalization.
Discussion
This study shows that robotic-assisted right colectomy yields similar operative and postoperative outcomes to those of laparoscopic-assisted right colectomy when performed by a surgical fellow. The learning curve appears to be longer for LRC, whereas with only 16 robotic procedures, a significant reduction in the operative time was observable for RRC. RRC was also associated with significantly less blood loss than LRC. The postoperative complication rate and the histologic variables were not different between the two approaches. Interestingly, these results also show that the health-related costs were similar between LRC and RRC when considering the mean cost per procedure by adding the surgical costs (significantly higher in RRC) to the hospital stay.
A paucity of reports exists on learning curves involving robotic colonic surgery, 22 whereas more literature is available for laparoscopic procedures.4–6,11,12,14,31,32 Comparing the two techniques is also difficult in the literature because most of the time, the surgeons beginning their learning curve in robotics are already experienced in laparoscopy, and this can have a direct and indirect influence on their robotic skills. In this study, the operating surgeon was simultaneously adopting laparoscopic and robotic surgery techniques for right colectomy procedures, and he was at the beginning of his minimally invasive career. Thus, the results provide further elucidation of MIS learning curves and allow direct comparisons. To our knowledge, only one previous study used this design to compare laparoscopy versus robotic rectal surgery and concluded that the simultaneous development of laparoscopy and robotics provides acceptable perioperative outcomes and robotics had a faster learning curve. 30 These results confirmed those findings for the particular setting of right colectomy. Indeed, RRC appears to have a learning curve of 16 procedures, whereas the laparoscopic procedure requires 25. In discordance with the literature,33,34 this study also showed that the mean operative time of RRC was similar to that of LRC, which falls into the previously reported ranges for laparoscopic-assisted right colectomy (85–214 minutes35–37 ). Moreover, the operative time decreased progressively with the number of procedures and increasing surgeon experience for both the robotic and the laparoscopic approaches, but this process appeared faster for robotic surgery. Interestingly, this decrease seems to be attributable to both the decrease in docking time, which was finally assessed at 15–18 minutes, and the decrease in surgeon console time, which directly corresponds to the laparoscopic time. After 16 RRC procedures, an improvement in the operative time was observed and appeared stable for the subsequent 14 procedures analyzed in this study. For LRC, the same decrease in operative time was seen after 31 procedures, and it was more difficult to identify a plateau, even after 40 procedures. Moreover, the total operative time for robotic surgery improved rapidly, and after only 16 cases, it became faster (trend toward significance) compared with the laparoscopic surgery. This difference may disappear with time, as demonstrated by these results that showed a similar operative time between LRC and RRC in the last case series (cases 21+). This may be explained by the fact that robotic instruments offer greater dexterity and a much more stable view of the operating field than laparoscopic ones, which may be particularly useful for inexperienced surgeons. With increasing experience, the surgeon may be able to overcome the laparoscopic technical drawbacks and be equally proficient at both procedures.
In this study, no intraoperative complications occurred, and no conversions were required during the RRC procedure, whereas two LRC patients were converted to laparotomy. Although not statistically significant, this finding is in accordance with the previous literature on robotic colorectal surgery38–41 and suggests that robotics is feasible and may even facilitate some critical steps of the colectomy procedure that can be particularly challenging.
Previous studies have reported that operative time proficiency in robotic rectal surgery is reached in 15–25 cases. 22 Another study has recently estimated that 80 robotic total mesorectal excision cases are the necessary learning curve, 42 although operative times did not improve during the course of the study. Thus, data in the literature are still controversial, but it must be noted that the learning curve may be substantially different among right colectomy, colorectal resection, and total mesorectal excision, which have varying levels of difficulty and require different technical skills.10,11,22,30,43 In this regard, right colectomy appeared to be a suitable intervention to start the learning curve 35 and was chosen in this study as the sole procedure (performed with the same approach, that is, medial to lateral, in both RRC and LRC) to limit possible confounders in the evaluation of the learning curve.
Given these data, the robotic approach can be considered an alternative to laparoscopy for right colectomy because it proved to be safe, yielded comparable results to those of laparoscopy, and has a faster learning curve. The major concern will remain the costs for the public health system. These results must be interpreted with caution because they refer to a specific subset of procedures performed by a surgical fellow during the learning curve period. Despite this, this study shows that the two surgical techniques were not associated with different health-related costs when combining surgery-related costs and those of the hospitalization.44,45 Indeed, RRC procedures carry higher intraoperative costs in terms of surgical materials than laparoscopy, but the costs of laparoscopy per se may be expected to be higher than those for experienced surgeons. Thus, the gap between the two approaches may be inferior to what has been previously reported in the literature and is balanced out by the costs in the postoperative period. Another important point is the low incidence of complications, which can drastically influence the costs for the healthcare system. The investment to procure the robotic platform was not considered in the analyses. These aspects cannot be neglected, and these results cannot be generalized. However, they may suggest that the arguments for cost-effectiveness or saving resources as a means of discouraging robotic surgery training and implementation are no longer valid.20,24,46,47
One of the main limitations of this study was the relatively small number of cases, especially for the robotic procedure. Moreover, the learning curve was evaluated in a single surgeon, and the potential additive or even synergistic learning effects transferring from laparoscopy to robotic surgery and vice versa (which were developed simultaneously) cannot be excluded. On the other hand, the fact that this was a single surgeon performing both procedures at the onset of his career allows a unique head-to-head comparison where many variables and effects stay similar for both techniques. However, the external validity of these findings was not assessed, and all operative, postoperative, and health cost results should take into account the specific situation of a surgical fellow at the beginning of his MIS career in a university colorectal surgical unit. The points of strength for this study include the homogeneous sample of patients undergoing LRC and RRC during the same time period. The two groups were not balanced in numbers (due to the lower availability of the robotic platform compared to the laparoscopic instruments), but they did not differ in the most important demographic, clinical, and tumor-related variables.
In conclusion, robotic-assisted right colectomy is associated with similar operative and postoperative outcomes to laparoscopic-assisted right colectomy when performed by a surgical fellow during his learning curve. The advantages of MIS are observable in both robotic and laparoscopic procedures, but the latter procedure appears to be associated with a longer learning curve. With increasing experience, the operative time decreases progressively, and the time is not longer when operating with the robotic platform. This finding suggests that it is reasonable and important to include robotic colorectal training in surgical fellowships and this advanced MIS approach should be considered safe, feasible, and advisable in colorectal surgery.
Footnotes
Acknowledgment
The authors would like to thank Dr. Clotilde Carra for her valuable support.
Disclosure Statement
No competing financial interest exists.