
Abstract
Abstract
Objective:
To explore the feasibility, safety, and advantages of transareola single-site endoscopic thyroidectomy.
Methods:
From January 2014 to December 2015, 40 patients were randomly divided into an observation group who received single-site endoscopic thyroidectomy by the areola approach and a control group who underwent three-port endoscopic thyroidectomy by the areola approach with 20 patients in each group. The feasibility and safety of the operation and postoperative clinical outcomes were compared between these two groups.
Results:
There was no significant difference in operation time, intraoperative blood loss, and hospitalization time (P > .05) between the two groups. The subcutaneous dissection area in the observation group (130 [120–130] cm2) was significantly smaller than that in the control group (180 [170–190] cm2) (P < .01). In addition, there is much less postoperative drainage in the observation group (70 [50–80] mL) than in the control group (80 [60–100] mL) (P = .036). Furthermore, 24-hour postoperative pain score in the observation group (4.0 [3.0–5.5]) was significantly lower compared with that in the control group (5.0 [4.0–7.0]) (P = .047). Moreover, patients in the observation group present with significantly higher 7-day postoperative cosmetic satisfaction scores (9.0 [8.0–9.0]) than those in the control group (7.0 [7.0–8.0]) (P < .001).
Conclusion:
Transareola single-site endoscopic thyroidectomy exhibits superior advantages in clinical outcomes such as causing less pain and achieving better cosmetic satisfaction, compared with three-port endoscopic thyroidectomy.
Introduction
T
Transareola endoscopic thyroidectomy can be performed by the single-site or three-port approach.9,11 However, the advantages and limitations of these two surgical approaches still have not been well understood. In this study, we conducted a comparative study on the feasibility, safety, and advantages of transareola single-site versus three-port endoscopic thyroidectomy. A total of 40 patients with thyroid nodules admitted to our hospital between January 2014 and December 2015 were randomly divided into observation and control groups with 20 patients in each group. The observation group received transareola single-site endoscopic thyroidectomy, whereas transareola three-port endoscopic thyroidectomy was performed on the control group. We then compared the safety and surgical outcomes between the two groups. Our findings may provide important guidelines for transareola endoscopic thyroidectomy in the future.
Subjects and Methods
Patients
This study was carried out in accordance with the approved guidelines by the Ethics Committee of Shanghai Tongren Hospital and patients have signed an informed consent. From January 2014 to December 2015, 40 patients were recruited for this prospective study. The inclusion criteria for this study were as follows: (1) patients were pathologically confirmed to have benign thyroid nodules; (2) the nodule is limited to one side of the thyroid; (3) the size of the nodule is less than 3 cm in diameter; (4) patients exhibit a strong cosmetic desire; and (5) patients were worried that the tumors may continue to grow or become malignant and actively requested surgical removal of the tumors. The patients with the following conditions were excluded: (1) patients who were highly suspected of malignant thyroid cancer; (2) patients with a history of thyroiditis; (3) patients with a history of neck surgery or radiation therapy; (4) patients with a certain degree of failure in their hearts, livers, or kidneys; and (5) patients who could not tolerate anesthesia and general surgery. Before the surgery, the patients were informed that they would receive the transareola single-site or three-port endoscopic thyroidectomy and the scars would be left on the chest instead of the neck. The enrolled patients who met the above criteria were then randomly assigned at a 1:1 ratio to undergo either transareola single-site (Observation group) or three-port (Control group) endoscopic thyroidectomy. All participants of this study provided their written informed consent and this study was approved by the Ethics Committee of the Institutional Review Board.
Surgical procedures
All subjects underwent general anesthesia with endotracheal intubation and were placed in the supine position with the head higher than the feet. The neck was slightly extended by placing a soft pillow under the shoulders. The two legs of the patients were separated and the operator stood between them with two assistants on both sides of the patient. A monitor screen was placed at the head of the patient. As a control procedure, the transareola three-port endoscopic thyroidectomy was performed as follows: a 10-mm incision that penetrates through the deep fascia was made along the left side of the sternum. 500 mL of saline solution containing 1 mg of epinephrine was then injected into the subcutaneous layer of the anterior chest to reduce bleeding events. A dissection stick was used to separate the subcutaneous space to form a catheter reserve space. Ten millimeter trocar and 30° 10-mm endoscope were then placed into the space and CO2 was injected to maintain the pressure at 6–8 mm Hg. After 5-mm incisions were made along the upper edge of the areolas of the left and right breasts, a 5-mm trocar was placed into the subcutaneous loose connective tissue in the direction of the thyroid. An electrical hook was then employed to separate the subcutaneous loose connective tissue and moved sequentially along the deep surface of platysma and the lower side of the thyroid cartilage to the sternocleidomastoid. The linea alba cervicalis and the outer membrane of the thyroid were then excised vertically to expose the thyroid. An ultrasonic scalpel was used to free up the thyroid isthmus and ipsilateral thyroid lobe to sequentially expose the ipsilateral inferior thyroid artery and the middle thyroid vein so that the thyroid lesions can be removed. To perform the transareola single-site endoscopic thyroidectomy, following the sterilization process, a 15-mm curved skin incision was made along the interior and upper edge of the ipsilateral areola to sequentially cut through the skin, subcutaneous tissue, and superficial fascia. Similarly, to reduce bleeding during the surgery, ∼100 mL of “inflation fluid” saline solution containing 1 mg of epinephrine in 500 mL normal saline was injected into the subcutaneous layer of the anterior chest through the incision up to the neck using a Veress needle. A narrow subcutaneous tunnel was then dissected in the anterior surface of the pectoralis major muscle and clavicle with a dissection stick. A 10-mm trocar was inserted to inject CO2 into the tunnel to maintain the pressure at 6–8 mm Hg. A 10-mm rigid laparoscope (Stryker Endoscopy, San Jose, CA) was implanted and a 5-mm trocar was inserted medially next to the laparoscope to place surgical instruments. Under the guidance of the laparoscope, an ultrasonic scalpel (model GEN300; Ethicon, a Johnson & Johnson Company, Somerville, NJ) was employed to cut the remaining tissue intervals along the subcutaneous tunnel extending from the incision through the clavicular head into between the paired sternocleidomastoid fascia. It continued to go up to separate the dense tissue anterior to the body of the sternum and reached the thyroid cartilage. The linea alba cervicalis was incised using an electric coagulation hook. The strap muscles were subsequently separated, suspended with one or two sutures, and pulled outward the neck to expose the ipsilateral thyroid gland. The middle and lower parts were also suspended with sutures and pulled inward and upward to completely expose the ipsilateral thyroid. An ultrasonic scalpel was then used to sequentially cut the middle thyroid vein and the thyroid isthmus. The ipsilateral inferior thyroid artery and vein were bluntly dissected and the Berry ligament was transected to expose the superior thyroid artery and vein. After the superior pole of the gland was coagulated and dissected with an ultrasonic scalpel, the recurrent laryngeal nerve and parathyroid gland were then exposed and identified. After being placed in a retrieval endobag, the specimen was pulled out through the laparoscopic port and a frozen section of the specimen was examined for pathologic confirmation. After no bleeding and oozing were found at the wound site, a suction drainage tube was placed to remove fluids that may build up in the areas of surgery and absorbable sutures were used to close the trocar ports.
Assessment of clinical outcomes
The two groups of patients were compared in such areas as operating time, the volume of intraoperative blood loss, subcutaneous dissection area in the anterior thoracic wall and the neck, the volume of postoperative drainage, length of hospital stay, and postoperative complications, including recurrent laryngeal nerve injury and hypoparathyroidism. Pain scores and cosmetic outcome of the incisions were evaluated 24 hours or 7 days after the surgery, respectively, using the visual analogue scale (VAS).12,13 The patients were given postoperative pain medications as needed, only after they reported the pain scores. In this study, we assessed the cosmetic outcomes 7 days after the surgery, since it is most convenient to follow up the patients at this time point.
Statistical analysis
Statistical analysis was conducted using SAS 9.2. Attributes data measuring the frequency (%) between the two groups were compared using corrected chi-square test. Variable data were expressed as median (interquartile range [IQR]). t-Test was performed to compare variable data with normal distribution. When the variable data are not normally distributed, Wilcoxon two-sample test was used. The results were considered statistically significant, when P value is <.05.
Results
As described in the section of Subject and Materials, patients recruited for this study were divided into observation and control groups who received transareola endoscopic thyroidectomy by single-site or three-port approach, respectively. The observation group includes 2 males (10%) and 18 females (90%), ranging in age from 28 to 56 years with a median age of 45.0 (IQR, 34.5–48.0) years. There are 3 males (15%) and 17 females (85%) in the control group between 23 and 59 years with a median age of 45.5 (IQR, 37.0–49.5) years. There is no statistical difference in sex, age, and the size of the nodules between the two groups (P > .05), excluding the confounding effects of these factors on the results of our comparative study (Table 1).
The observation group: patients who received transareola single-site laparoscopic thyroidectomy; the Control group: patients who received transareola three-port laparoscopic thyroidectomy; n, number; IQR, interquartile range; P, P value.
To assess the advantages and limitations of transareola single-site or three-port endoscopic thyroidectomy, we first compared operating time, intraoperative blood loss, and length of hospital stay between the observation and control groups. As shown in Table 2, there is no significant difference in these areas between the two groups (P > .05).
The observation group: patients who received transareola single-site laparoscopic thyroidectomy; the Control group: patients who received transareola three-port laparoscopic thyroidectomy; n, number; IQR, interquartile range; P, P value.
Next, we compared the risks of potential complications between the two surgery procedures. As expected, no recurrent laryngeal nerve injury and hypoparathyroidism were identified in both control and observation groups. In contrast, transareola single-site endoscopic thyroidectomy causes a smaller subcutaneous dissection area (130 [120–130] cm2) than the three-port endoscopic thyroidectomy (180 [170–190] cm2) (P < .001). In addition, there is much less postoperative drainage observed in the observation group (70 [50–80] mL) than in the control group (80 [60–100] mL) (P = .036) (Table 2). These data suggest that transareola single-site laparoscopic thyroidectomy is a highly feasible and safe surgical option and causes minimum tissue damage, compared with three-port endoscopic thyroidectomy.
To evaluate the clinical outcomes of the two types of endoscopic thyroidectomy, we then assessed the pain scores 24 hours after surgery and the cosmetic satisfaction 7 days after thyroidectomy. We employed VAS to determine the pain score and cosmetic satisfaction.12,13 On a rating scale of 0–10, 0 indicates no pain and 10 reflects the worst pain. As for cosmetic satisfaction, 0 indicates no satisfaction, whereas 10 means “very satisfied.” As illustrated in Table 3, patients who received transareola single-site endoscopic thyroidectomy experience significantly less pain (4.0 [3.0–5.5]) than those with three-port endoscopic thyroidectomy (5.0 [4.0–7.0]) (P = .047). Similarly, patients are also significantly more satisfied with the cosmetic outcomes resulting from the transareola single-site endoscopic thyroidectomy (9.0 [8.0–9.0]) than those from three-port endoscopic thyroidectomy (7.0 [7.0–8.0]) (P < .001) (Fig. 1). These findings indicate that transareola single-site laparoscopic thyroidectomy exhibits better clinical outcomes than the three-port laparoscopic thyroidectomy.
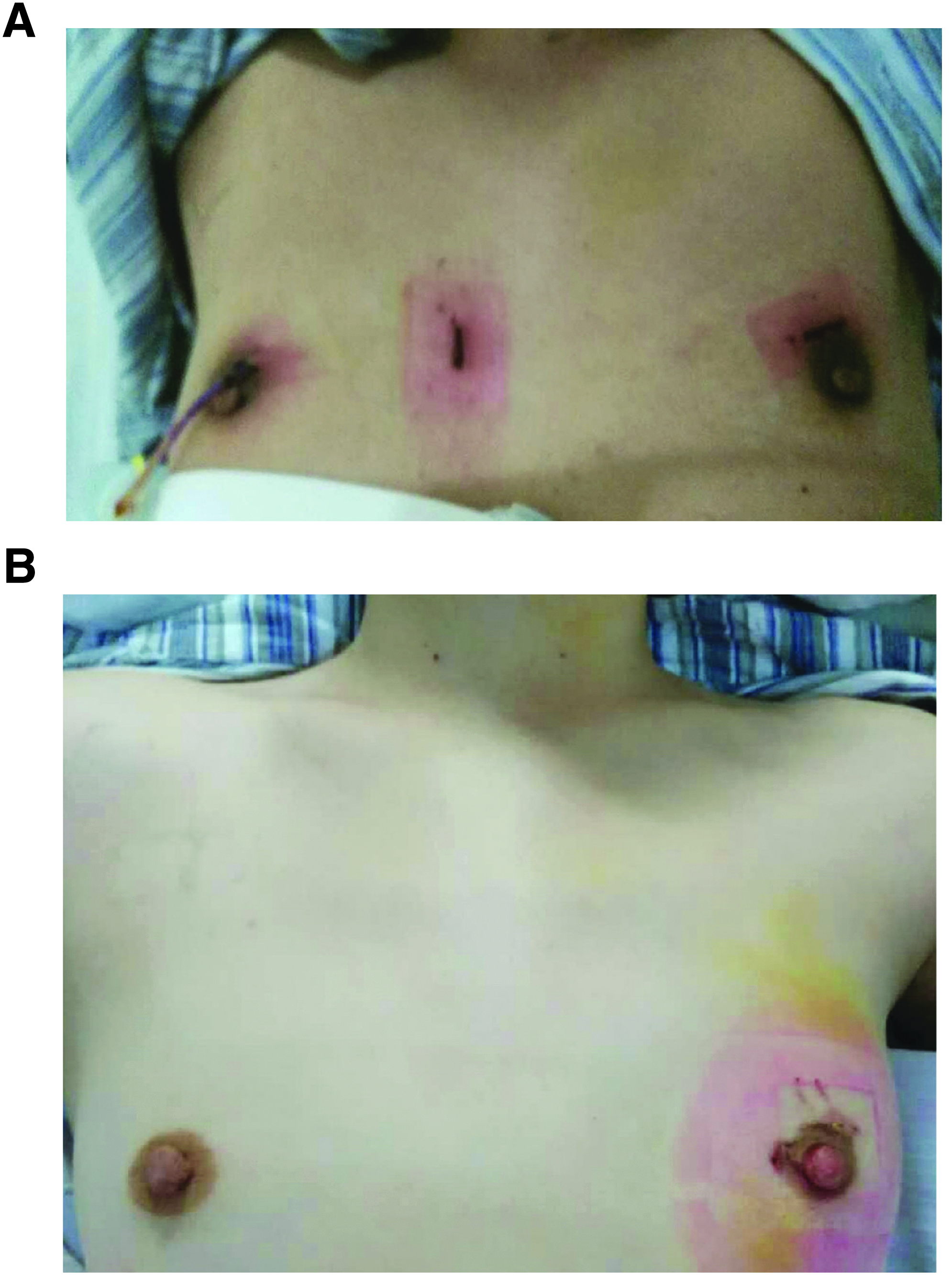
Representative photographs showing the cosmetic results 7 days after the surgery. The transareola three-port
On a rating scale of 0–10, 0 indicates no pain with 10 being the worst pain. As for cosmetic satisfaction, 0 indicates no satisfaction, whereas 10 means “very satisfied.”
The observation group: patients who received transareola single-site laparoscopic thyroidectomy; the Control group: patients who received transareola three-port laparoscopic thyroidectomy; n, number; IQR, interquartile range; P, P value.
Discussion
Traditional open thyroid surgery in the cervical area usually leaves a 6–10 cm surgical scar, seriously affecting the cosmetic appearance of the neck. 1 Intriguingly, transareola endoscopic thyroidectomy has been widely recognized as an ideal approach for thyroid surgery.2,3,14 However, the surgery was generally performed through a three-hole approach and needs dissection of a large area of subcutaneous tissues.2,3 In addition, the surgical incisions on the anterior chest wall used to result in hypertrophic scarring. 2 Therefore, the advantages and benefits of endoscopic thyroid surgery have been controversial.15–17 Intriguingly, these controversies catalyzed the emergence of transareola single-site endoscopic thyroidectomy, which displays minimum invasiveness and remarkable cosmetic outcomes.16,17 However, the advantages and limitations of transareola single-site or three-port endoscopic thyroidectomy have not been well explored. In this study, we, for the first time, compared the advantages and limitations between transareola single-site laparoscopic thyroidectomy and three-port endoscopic thyroidectomy. Our data showed that patients in the observation group exhibited significantly smaller subcutaneous dissection areas than patients in the control group. In addition, postoperative wound drainage was considerably reduced in the observation group, compared with the control group. Furthermore, transareola single-site laparoscopic thyroidectomy exhibits remarkably better clinical outcomes, including lower pain scores and more desirable cosmetic satisfactions, compared with three-port endoscopic thyroidectomy. These data indicate that transareola single-site laparoscopic thyroidectomy is a highly feasible and safe surgical procedure with superior clinical outcomes.
The data we presented here demonstrated that transareola single-site laparoscopic thyroidectomy exhibits superior advantages over three-port laparoscopic thyroid surgery. First, single-site laparoscopic thyroidectomy is less invasive and results in a substantial reduction in tissue injuries. This advantage can be well interpreted by the fact that single-site laparoscopic thyroidectomy needs only one incision, whereas three-port laparoscopic thyroid surgery needs to make three incisions. 18 Second, scars arising from the incision made along the areola in the single-site laparoscopic thyroidectomy can be concealed by the pigmentation of the areola, resulting in better cosmetic appearance. In contrast, incisions made on the anterior chest during the three-port laparoscopic thyroidectomy are prone to developing keloid scars.17,18 Third, transareola single-site laparoscopic thyroidectomy reduces the number of trocars used throughout the procedure, compared with the three-port laparoscopic thyroidectomy. This can serve to decrease the cost of the surgery and simplify the surgical procedure.
It is worth noting that there are a few limitations in the transareola single-site laparoscopic thyroidectomy, compared with the three-port endoscopic thyroid surgery.11,19 First, transareola single-site laparoscopic thyroidectomy involves a relatively narrow operating space since the surgery is carried out in a single-site and one-tunnel condition. 11 The limited working space results in collisions between the instrument and the laparoscope, increasing the difficulties in performing the surgery.11,19 To address this issue, we used cervical transcutaneous suture suspension and retraction to pull the thyroid and strap muscles inward and outward, respectively. 19 This technique better exposes the working area and allows safer operation. Second, the limited working space during the single-tunnel operation only allows for operating one instrument throughout the whole procedure, making it difficult to stop bleeding. Thus, before we created the subcutaneous tunnel for the surgery, adrenaline saline was injected in the surgical area to reduce bleeding and oozing. In addition, it also helps to reduce the likelihood of bleeding to choose the correct anatomical plane, the subcutaneous superficial fascia, to create the operation tunnel for the procedure. The connective tissue at this anatomical plane is loose and there are fewer blood vessels, which lower the chances of damaging the fascia and blood vessels. 11 Likewise, the use of ultrasonic knife to disarticulate the upper and lower blood vessels of the thyroid gland also helps to minimize bleeding. The ultrasonic scalpel was used to precoagulate the proximate end and subsequently seal the distal end of the thyroid blood vessels, which enables more precise vascular closure. 17 Third, the continuous use of energy-generating instruments such as ultrasonic knife or electrical hook throughout the surgery produces smoke. 20 Since the working space is very limited, the smoke produced by the instruments does not disperse easily and blocks the view of the surgeons. Thus, it is very important to follow the correct guidelines to use energy-generating instruments. Regularly cleaning and removing the eschar from the tip of the instruments will maximize the power of the knife and reduce smoke production. 20 In addition, shortening the duration of the electrocoagulation of the blood vessels or repeating it multiple times for a shorter period each time will serve to diminish the production of smoke. We think that the suggestions we discussed above will help to address the limitations of the transareola single-site laparoscopic thyroidectomy.
Taken together, compared with the three-port endoscopic thyroid surgery, transareola single-site laparoscopic thyroidectomy is more desirable in terms of minimum invasiveness and cosmetic outcomes. In addition, it will be very helpful to follow the guidelines we discussed above to overcome certain limitations of the transareola single-site laparoscopic thyroidectomy. We believe that with the accumulation of surgical experience and continuous improvement of endoscopic instruments, the transareola single-site laparoscopic thyroidectomy will be widely used and can be performed for the treatment of more complex thyroid diseases in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.