
Abstract
Abstract
Background:
To investigate the effects and technical points of several individualized laparoscopic therapies for patients suffering from cirrhotic portal hypertension.
Methods:
In total, 385 cirrhotic patients who underwent the treatment of individualized laparoscopic therapy from February 2012 to December 2015 at the Clinical Medical College of Yangzhou University were enrolled in this study. We retrospectively analyzed the clinical data and the key technical points.
Results:
Individualized laparoscopic therapies were successfully performed on 379 of 385 cases. Six cases were converted to a laparotomy (the rate of conversion to laparotomy was 1.6%). Modified laparoscopic splenectomy (MLS) for cirrhotic patients with hypersplenism was successfully performed on 103 of 105 cases. Laparoscopic azygoportal disconnection for cirrhotic patients with esophagogastric variceal bleeding (EGVB) or F3 varices was successfully performed on 61 of 62 cases, and modified laparoscopic splenectomy and azygoportal disconnection (MLSD) for cirrhotic patients with hypersplenism and EGVB or F3 varices was successfully performed on 196 of 201 cases. Synchronous MLS and laparoscopic partial hepatectomy (SLSH) for cirrhotic patients with hypersplenism and hepatocellular carcinoma (HCC) and synchronous MLSD and laparoscopic partial hepatectomy (SLSDH) for cirrhotic patients with hypersplenism, EGVB or F3 varices and HCC were all successfully implemented on 12 and 5 patients, respectively. From May 2013, we used the intraoperative autologous cell salvage during each individualized laparoscopic procedure.
Conclusions:
An individualized laparoscopic therapy was beneficial for different state of selected cirrhotic patients with portal hypertension with or without HCC.
Introduction
I
Different cirrhotic patients present different states of PH. Some patients only suffer from hypersplenism, some suffer from oesophagogastric variceal bleeding (EGVB) with hypersplenism, some suffer from concurrent hypersplenism and hepatocellular carcinoma (HCC), and others suffers from concurrent hypersplenism, EGVB, and HCC. In our center, cirrhotic patients with different states of PH were subject to an individualized laparoscopic therapy scheme, including modified laparoscopic splenectomy (MLS), laparoscopic azygoportal disconnection (LD), modified laparoscopic splenectomy and azygoportal disconnection (MLSD), 2 synchronous MLS and laparoscopic partial hepatectomy (SLSH), 3 and synchronous MLSD and laparoscopic partial hepatectomy (SLSDH). 4 This scheme will extend the advantages of laparoscopic surgery to a number of patients who are likely to benefit the most, namely cirrhotic patients with PH with or without HCC.
Materials and Methods
Clinical data
From February 2012 to December 2015, an individualized therapy scheme was performed on 385 cirrhotic patients with PH with or without HCC (233 men and 152 women) ranging in age from 23 to 76 years (mean 52.8 ± 10.1 years). In total, 105 patients received MLS, 62 patients received LD, 201 patients received MLSD, 12 patients received SLSH, and 5 patients received SLSDH. The Ethics Committee of the Clinical Medical College of Yangzhou University approved the study.
Retrospectively collected perioperative and follow-up data included age, sex, Child-Pugh classification, model for end-stage liver disease (MELD) score, platelet (PLT) count, operation time, estimated intraoperative blood loss, allogeneic transfusions, autologous transfusions, conversion to laparotomy, postoperative hospital stay, emergency operation for bleeding, portal vein system thrombosis (PVST) on postoperative day (POD) 7, main trunk thrombosis on POD 7, gastric leakage, temporary pancreatic fistula, encephalopathy, pulmonary infection, abdominal infection, EGVB, incisional infection, encephalopathy, secondary liver cancer, and death (Table 1).
LD, laparoscopic azygoportal disconnection; MLS, modified laparoscopic splenectomy; MELD, end-stage liver disease scores; MLSD, modified laparoscopic splenectomy and azygoportal disconnection; POD, postoperative day; PVST, portal vein system thrombosis; SLSDH, synchronous MLSD and laparoscopic partial hepatectomy; SLSH, synchronous MLS and laparoscopic partial hepatectomy.
In our department, anticoagulation regimen was administrated from POD 3 to prevent postoperative PSVT. Patients received anticoagulant regimen with warfarin or aspirin according to individual preference. Patients in the warfarin group received 2.5 mg of oral warfarin (Harvest) once daily, with the dose titrated to maintain a target international normalized ratio (INR) of 2.0 to 2.5, whereas patients in the aspirin group received 100 mg enteric-coated aspirin tablets (Bayer) once daily.
Inclusion criteria and exclusion criteria
The general inclusion criteria were as follows: a clinical, radiological, or histologic diagnosis of cirrhosis of any etiology; age of 18–75 years; Child-Pugh liver function grade of A or B; and no evidence of PVST by ultrasound evaluation and angio-CT.
The general exclusion criteria were as follows: a hypercoagulable state other than that related to liver disease, baseline INR of >2.0, recent peptic ulcer disease, history of hemorrhagic stroke, pregnancy, uncontrolled hypertension, and human immunodeficiency virus infection.
The particular inclusion criteria for MLS included splenomegaly with secondary hypersplenism (a blood PLT count of < 50 × 109/L).
The particular exclusion criteria for MLS included hepatocellular carcinoma or any other malignancy, EGVB or F3 varices.
The particular inclusion criteria for LD included EGVB or F3 varices (large, coil-shaped).
The particular exclusion criteria for LD included hepatocellular carcinoma or any other malignancy and secondary hypersplenism with a blood PLT count of < 50 × 109/L.
The particular inclusion criteria for MLSD included splenomegaly with secondary hypersplenism (a blood PLT count of < 50 × 109/L), EGVB or F3 varices.
The particular exclusion criteria for MLSD included hepatocellular carcinoma or any other malignancy.
The particular inclusion criteria for SLSH included hepatocellular carcinoma or splenomegaly with secondary hypersplenism (a blood PLT count of < 50 × 109/L).
The particular exclusion criteria for SLSH included EGVB or F3 varices.
The particular inclusion criteria for SLSDH included hepatocellular carcinoma, splenomegaly with secondary hypersplenism (a blood PLT count of < 50 × 109/L), EGVB or F3 varices.
No particular exclusion criteria were utilized for SLSDH.
The contraindication of cell salvage and autologous blood transfusion
The exophytic or ruptured HCC should not been applied with cell salvage and autologous blood transfusion. The technique should be used before the laparoscopic hepatectomy during SLSH and SLSDH procedures.
Surgical Technique
MLS, LD, or MLSD procedures
The MLS procedure was described in our previous article on MLSD. 2 A five port method similar to the previous report was used (Fig. 1). A 10-mm trocar (port A) was placed through the umbilicus for a 10-mm, 30° angled laparoscope. Port B was placed in the right midclavicular line halfway between the costal margin and the umbilicus. Port C was placed in the right midclavicular line immediately below the costal margin. Port D was placed in the left midclavicular line halfway between the costal margin and the umbilicus. Port E was placed in the left anterior axillary line below the border of the spleen. After the spleen was dissected, a laparoscopic spleen extraction was performed through Port D. Cylindrical spleen tissue (Fig. 2) was removed using a 12-mm trocar by an electromechanical morcellator without enlarging any port incision. A drainage tube was placed under the left diaphragm.

Trocar positions for modified laparoscopic splenectomy, laparoscopic azygoportal disconnection, and modified laparoscopic splenectomy and azygoportal disconnection.

Cylindrical spleen tissue.
The LD procedure was similar to that described in our previous article on MLSD 2 ; however, the laparoscopic splenectomy (LS) procedure and laparoscopic spleen extraction were deleted. A drainage tube was placed beneath the stomach body.
The MLSD procedure was the same as described in our previous article. 2 A drainage tube was placed at the spleen fossa.
MLSH or MLSDH procedure
During the SLSH or SLSDH procedure, laparoscopic hepatectomy was performed after the LS or laparoscopic splenectomy and azygoportal disconnection (LSD). A (5 + 1)-port or five-port method was used for LSH or LSDH (Fig. 3). The positions of A, B, C, D, and E were the same as described for MLSD. Port F was placed in the right anterior axillary line just below the costal margin. Ports B, C, D, and E were used for LS or LSD. These ports were also used for laparoscopic left partial hepatectomy, and ports B, C, D, and F were used for laparoscopic right partial hepatectomy.
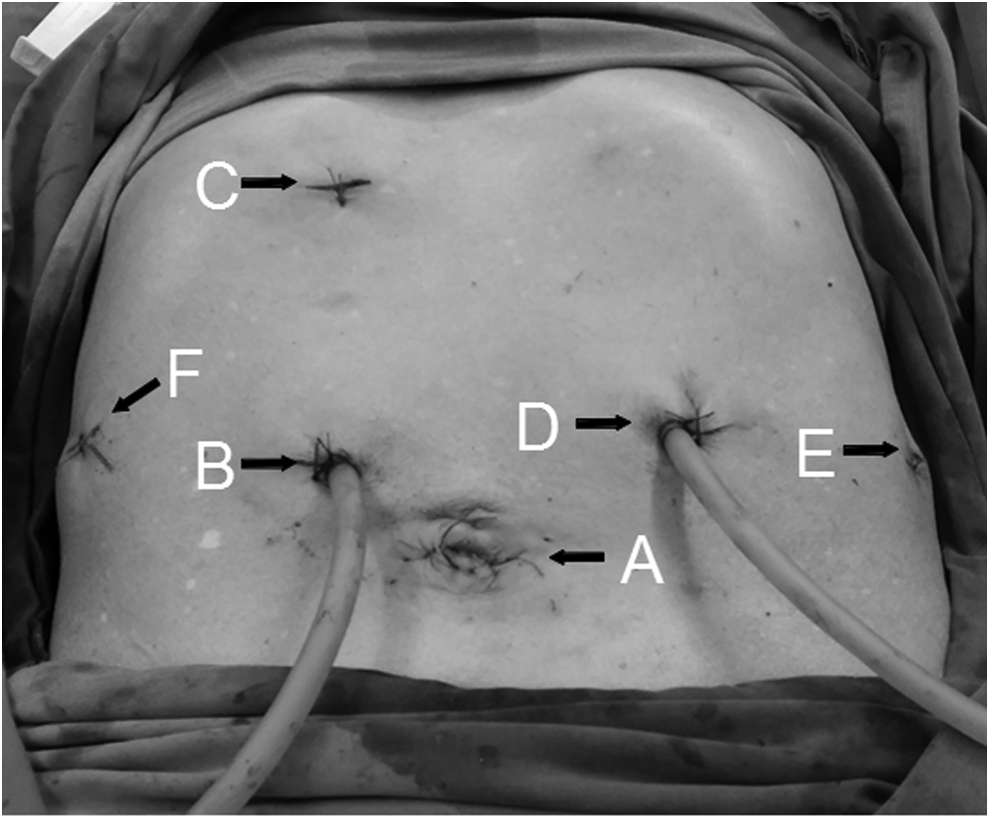
Trocar positions for synchronous laparoscopic splenectomy and laparoscopic partial hepatectomy, and synchronous laparoscopic splenectomy and azygoportal disconnection with partial hepatectomy.
The laparoscopic partial hepatectomy procedure was performed as follows. The procedure began after advanced preparation of the device used for the modified Pringle maneuver described in our previous article, 5 which could be used to occlude the inflow in the entire liver when necessary. If the neoplastic lesion was located in the right lobe, port E would typically be used for the modified Pringle maneuver. If the neoplastic lesion was located in the left lobe, port F would occasionally be prepared for the modified Pringle maneuver as needed. With increasing laparoscopic experience, port F was abandoned for utilization in the next consecutive laparoscopic left hemi-hepatectomy or laparoscopic hepatic left lateral lobectomy.
If the laparoscopic approach was a left hemi-hepatectomy, the left branch portal vein and left hepatic artery were separated and occluded with a clip, and the inflow in the remnant liver remained open. The falciform and triangular ligaments were divided to mobilize the liver. After these manipulations, the blocking zone after left liver ischemia was clearly visible. The hepatic resection line was marked along the blocking zone with a monopolar electrocautery device. A harmonic scalpel was used to dissect the parenchymal liver tissue. To locate the biliovascular structures, the assistant surgeon used the aspirator to push, suck, and scratch the tissue. Small biliovascular structures were divided using the harmonic scalpel, whereas wider biliovascular structures was clasped with the Hem-o-lok and then divided with a 5-mm LigaSure vessel-sealing device. The left hepatic vein was divided using an endoscopic stapling device with 2.5-mm staples.
If the laparoscopic approach was a wedge hepatectomy, intraoperative ultrasonography was first performed to assess the boundaries of the HCC and its relationship with major vascular structures. A 1-cm hepatic resection line beyond the margin of the HCC was scored via electrocautery. The modified Pringle maneuver was always performed after an ∼1.0-cm-deep cut was created in the liver tissue by harmonic scalpel, then the harmonic scalpel was further used to resect the liver.
The entire spleen was removed with an electromechanical morcellator as described in our previous reports. 2 The liver specimen was loaded into a specimen bag and removed though the umbilical port, which was extended to a proper length according the size of the HCC along the linea alba. At the end of the operation, one surgical drainage tube was placed at the epiploic foramen, and another surgical drainage tube was placed under the left diaphragm.
Cell salvage and autologous blood transfusion
Cell salvage was used throughout the entire MLS, LD, and MLSD procedures 6 and before laparoscopic hepatectomy during the SLSH 3 and SLSDH procedures. 4 The blood sequestered within the enlarged spleen and that from intraoperative blood lost were collected and processed with heparinized saline using a cell saver (Autologous Blood Recovery System; Beijing Jingjing Medical Equipment Co. Ltd.). Intraoperative blood was collected at three different stages. First, once the spleen was completely divided, the patient was placed in the Trendelenburg position with a left half-lateral position. Blood was drained through the splenic hilum that was cut open by scissors and suctioned from the left upper quadrant. Second, blood lost intraoperatively was collected by a cell saver at any time. Finally, a small quantity of blood was also discharged from the spleen after its morcellation.
Statistical analysis
Parametric data were expressed as the mean ± standard deviation. Nonparametric data were expressed as medians (interquartile range), and categorical data were presented as percentages. Parametric data were compared using Student's t-test.
Results
Perioperative results and follow-up data of each individualized therapy scheme involving MLS, LD, MLSD, SLSH, and SLSDH groups were described in Table 1. Conversion rates in MLS, LD, MLSD, SLSH, and SLSDH groups were 1.9% (2/105), 1.6% (1/62), 1.5% (3/201), 0% (0/12), and 0% (0/5) respectively. The overall rates of postoperative complications in MLS, LD, MLSD, SLSH, and SLSDH groups were 42.9% (45/105), 12.9% (8/62), 50.2% (101/201), 75% (9/12), and 60% (3/5) respectively. The comparisons between PLT at admission and PLT on POD 7 were showed in Table 2. PLT on POD 7 were all significantly higher than that at admission in MLS, MLSD, SLSH, and SLSDH groups respectively (all P < .001). There were no significant differences between PLT at admission and PLT on POD 7 in LD group (P > .05).
LD, laparoscopic azygoportal disconnection; MLS, modified laparoscopic splenectomy; MLSD, modified laparoscopic splenectomy and azygoportal disconnection; PLT, platelet; POD, postoperative day; SLSDH, synchronous MLSD and laparoscopic partial hepatectomy; SLSH, synchronous MLS and laparoscopic partial hepatectomy.
During a postoperative follow-up period of 2–48 months, 16 cases were lost to follow-up, and 4 patients died during this period, including acute EGVB in 2 patients who received MLSD, secondary liver cancer in 1 patient who received MLSD, and recurrent liver cancer in 1 patient who received SLSH, yielding a 2.5% mortality rate. Among them, only one patient who received MLSD suffered from acute EGVB died within 30 days, other 3 mortalities were all late mortalities.
In our department, ascites was assessed by ultrasound screening at admission. If the patients suffered from ascites, they should be administrated with diuretics until ascites disappeared. Hence, none had ascites at the time of surgery. Total 81 (77.1%) had ascites assessed by ultrasound screening on POD 7 in the MLS group with 5 (4.8%) ascites leaks, 37 (59.7%) had ascite in the LD group with 3 (4.8%) ascites leaks, 163 had ascites (81.1%) in the MLSD group 10 (5.0%) ascites leaks, 11 (91.7%) had ascites in the SLSH group with 1 (8.3%) ascites leaks, and 5 (100%) had ascites in the SLSDH group with 1 (20.0%) ascites leaks.
Discussion
In Asia, large numbers of patients suffered from PH due to liver cirrhosis given the high incidence of the chronic hepatitis B and C. These cirrhotic patients typically represent various state of PH, including with or without different degrees of hypersplenism or/and different degrees esophagogastric varices. Partial cirrhotic patients with PH suffered from concurrent HCC. Approximately 30% of HCC patients also exhibited hypersplenism.7,8
Patients with concurrent cirrhosis and PH typically have poor liver function and coagulation disorders. Surgical procedures with the least possible impairment that contribute to rapid recovery are jointly desired by both surgeons and patients. Today, given the rapid advancement of laparoscopic surgery, it is important to determine how surgeons can make good use of the laparoscopic technique to benefit these patients and offer better surgical procedures. To date, few surgical teams have reported the technique of LS for hypersplenism secondary to PH and LSD for cirrhotic patients with EGVB and hypersplenism.
In our department, our surgical team created various individualized laparoscopic therapy schemes for different states of PH. In March 2007, Hong et al. first reported 23 patients who underwent total LSD without a hand-assisted procedure. 9 LSD is associated with less pain compared with open laparoscopic splenectomy and azygoportal disconnection (OSD), but patients still complained about abdominal incision pain mainly due to the enlarged incision required for a massively enlarged spleen. Moreover, most surgeons complained and were reluctant to perform LSD or LS because placement of the spleen into an intracorporeal bag is quite challenging, the creation of an enlarged incision or hand-assisted incision is necessary for removal of the spleen, and the procedure is tedious. Thus, the advantages of laparoscopic surgery are obviated.10–12
Since 2012, our team has developed an MLSD technique, and this is the first report of the use of an electromechanical morcellator to extract the entire massive splenic tissue through the existing trocar incision. 2 This technique eliminates the need for the creation of hand-assisted or enlarged incisions to remove the spleen, reduces surgical trauma, and shortens the time required to remove the spleen given that time is not needed to enlarge the incision, place the spleen into an intracorporeal bag, and sew the enlarged incision. The technique is easy to learn and will enable and encourage surgeons to perform LSD.
Furthermore, in MLSD, we optimized the laparoscopic procedure, including LS, LD, and laparoscopic spleen extraction, as described in our previous articles. 2 Our previous study reported that MLSD is technically feasible and safe and is preferable to OSD. MLSD is associated with minimal postoperative pain and scarring and faster postoperative recovery compared with OSD.2,6,13
Similarly, in our department, pure LS also used the laparoscopic spleen extraction method with an electromechanical morcellator.
There is some controversy about whether splenectomy is necessary or even beneficial for cirrhotic patients whose hypersplenism is not severe (PLT ≥50 × 109/L). Advocates for splenectomy believe that the spleen in patients with PH is harried with serious fibrosis; therefore, minimal immune function is noted in those with splenomegaly. 14 Advocates inclined to preserve the spleen believe that a spleen with PH may still exhibit some immune function, 15 whereas a splenectomy may exacerbate immune dysfunction in the presence of PH.16,17 Voros et al. proposed that a splenectomy should be exclusively performed in patients with severe hypersplenism. 18 The spleen is also thought to be the regulating center of the immune system, which is a metabolic feature involved in endocrine function. 19 Overwhelming postsplenectomy infection may lead to mortality rates of up to 50%. 20 Furthermore, splenectomy for hypersplenism is attributed to a high incidence of PVST that may deteriorate liver function and increase portal pressure, thus contributing to the high risk of EGVB recurrence21,22; or even lead to ischemic intestinal necrosis.23–25 PVST is correlated with poor patient survival.26,27 Our surgical team supported the viewpoint of preserving the spleen. In our department, patients with PH suffering from EGVB and moderate hypersplenism (PLT count ≥50 × 109/L) only received LD. In addition, LS was not performed for PH patients with moderate hypersplenism.
Performing prophylactic LD to treat F3 grade varices without bleeding caused by PH in cirrhotic patients remains controversial. An opponent of prophylactic LD considered LD to be an additional trauma for patients. Our surgical team was an advocate of prophylactic LD based on the following reasons. Although prophylactic LD appears to be an additional trauma, the technique is safe and offers a short operation time, a small amount of blood loss, and fewer complications (Table 1). 28 F3 grade varices will likely progress to EGVB, which lead to the damage of liver function and is a major cause of death in patients with PH due to liver cirrhosis. LD can effectively reduce the EGVB rate. Of note, patients using LD with less operation trauma exchange for the safety by avoiding EGVB.
Difficult perioperative bleeding control and postoperative liver decompensation are the major complications associated with hepatectomy in patients with HCC and PH. In the past, hepatectomy was not recommended in patients with both HCC and PH.29–31 Fortunately, splenectomy has been proven as an effective method to overcome these problems.32,33 Some studies have demonstrated that synchronous open splenectomy and hepatectomy may improve disease-free survival rates without an increased perioperative risk for patients with cirrhotic HCC and hypersplenism.34,35
Surgical procedures with the least possible impairment and rapid possible recovery are always pursued by surgeons. In 2011, Ohno et al. first reported a case report of SLSH. 36 Surgical teams seldom report SLSH,36–38 which is considered to be a safe and useful minimally invasive procedure for the treatment of hepatocellular carcinoma with hypersplenic thrombocytopenia. Our surgical team has successfully performed 12 cases of SLSH since 2015. 3 Selective SLSH is a feasible, effective, and safe surgical procedure with satisfactory short-term efficacy, and the technique embodies an ideal minimally invasive procedure for liver cirrhotic patients with HCC and hypersplenism.
In 2015, our surgical team first reported the use of SLSDH for patients with concurrent HCC, EGVB, and hypersplenism due to PH. 4 SLSDH has been successfully performed for 5 patients. We are in the initial developmental stages of SLSDH, and patients with HCC and PH selected to undergo SLSDH should meet the following indications: tumor diameter ≤5 cm, tumor located in the left lobe or peripheral right lobe of the liver, and Child-Pugh class A or B liver disease. The procedure is a promising minimally invasive treatment option for cirrhotic patients with concurrent HCC, EGVB, and hypersplenism.
In 2012, Wang et al. were the first to report splenic blood salvage during LSD, 10 which significantly increases postoperative Hb. We used cell salvage and autologous blood transfusion during each laparoscopic procedure for PH performed since May 2013 if the above-mentioned contraindications were not noted. Our study found that the conservation of intraoperative blood loss using the cell saver and the use of sequestered splenic blood during MLSD resulted in a perioperative increase in Hb of 11.2 g/L. 6 One of the most serious perioperative complications during LSD is the rapid loss of large volumes of blood; timely intraoperative cell salvage and fast autologous blood transfusion can relieve the pressure placed on the surgical staff. Furthermore, the technique reduces the need for allogeneic blood transfusion by relieving pressure on transfusion services and avoids complications due to allogeneic blood transfusion.
In conclusion, an individualized laparoscopic therapy scheme including MLS, LD, MLSD, SLSH, and SLSDH is a safe, feasible, and effective surgical procedure, and the scheme allows for optimal minimally invasive treatment for different states of cirrhotic patients associated with PH with or without HCC. This study is limited by its small sample size; therefore, specifically designed prospective studies with a larger cohort that include randomized comparisons with the open operation should be performed.
Footnotes
Acknowledgments
This work was supported by the scientific research subject of Jiangsu province health department (No. H201452) and six kinds of talents of Jiangsu province (No. WSW-087).
Disclosure Statement
No competing financial interests exist.