
Abstract
Abstract
Background & Aim:
Gastric cancer is a leading cause of cancer-related mortality worldwide. We have invented a novel hand-assist device that allows the placement of surgical instruments and the maneuvering of the surgeon's hand, and we have established a new hand-assisted laparoscopic technique called Three United Laparoscopic Surgery (TULS) for laparoscopic dissection of advanced gastric cancer. The present study aimed at exploring the usefulness of TULS in the treatment of advanced gastric cardia cancer.
Method:
A retrospective study on 100 patients with advanced gastric cardia cancer admitted from January 2014 to June 2015 was done. There were 38 cases of TULS, 30 cases of laparotomy, and 32 cases of laparoscopy-assisted surgery. Statistical comparisons between three treatment groups in operative time, incision length, amount of bleeding, number of lymph nodes dissected, time to flatus after surgery, rate of postoperative complications, hospital stay, and expense were done.
Results:
For lymph node dissection, there were no significant differences between TULS, laparotomy, and laparoscopy-assisted surgery. However, compared with conventional laparotomy, TULS and laparoscopy-assisted surgery were found to be able to minimize incision length, reduce blood loss during surgery, lower postoperative complication rate, and shorten time to flatus and hospital stay. The differences were statistically significant (P < .05). The operative time of TULS was significantly shorter than that of the laparoscopy-assisted surgery (P < .05), and it was comparable to that of laparotomy.
Conclusion:
TULS is as efficient as laparotomy in lymph node dissection, and it shows the advantages of minimally invasive surgery. It can be considered a novel and promising surgical intervention for treatment of advanced gastric cancer.
Introduction
G
In 1994, Kitano et al. reported the treatment of early gastric cancer by laparoscopy-assisted surgery, 4 and in 1997, Goh et al. showed that laparoscopic radical gastrectomy could achieve survival benefits, although short term, in patients with advanced gastric cancer. 5 Compared with laparotomy, laparoscopy-assisted gastrectomy is less traumatic to patients, offering advantages of a lower risk of postoperative complications and, in turn, quicker recovery. Laparoscopy has gradually gained acceptance as a safe and feasible approach for not only tumor staging but also radical gastrectomy for early gastric cancer and palliative surgery for patients with advanced gastric cancer.
Despite the encouraging outcomes achieved in patients with early gastric cancer, the treatment of advanced gastric cancer with laparoscopy-assisted gastrectomy has remained controversial. Whether or not the laparoscopic approach would be equivalent to open abdominal surgery in lymph node dissection is debatable. In addition, for patients with advanced gastric cancer, the survival benefit of laparoscopic gastrectomy has yet to be established. 6 In view of these, and given the fact that laparoscopy is technically challenging due to the complex anatomy of the cavity, hand-assisted laparoscopy has emerged as a surgical approach that allows the insertion of the surgeon's hand into the abdomen via a hand-assist device for easy exposure, complete exploration, and meticulous dissection.
Laparotomy, laparoscopy, and hand-assisted laparoscopy have their own advantages, and a well-coordinated combined use of these surgical approaches is believed to benefit the treatment of advanced gastric cancer. As such, we have designed a novel hand-assist device that facilitates the placement of surgical instruments and the insertion of the left hand of the surgeon into the patient's cavity (Chinese patent no. 201220661287.9). The improved surgical procedure using our novel device was called Three United Laparoscope Surgery (TULS). TULS affords the interchange between laparotomy, laparoscopy, and hand-assisted laparoscopy whenever necessary. Besides, it provides surgeons with a better vision, and it preserves the advantages of minimally invasive surgery without compromising its ability to resect tumors and to dissect lymph nodes. In the present study, we evaluated the usefulness of TULS in the radical D2 gastrectomy for treatment of advanced gastric cardia cancer.
Methods
Patient enrollment criteria
A total of 100 patients with advanced gastric cardia cancer admitted to our medical center from January 2014 to June 2015 were enrolled in the study. All patients were first encouraged to receive either TULS or laparoscopy-assisted surgery, and if they refused, laparotomy was administered. There were 38 cases of TULS, 30 cases of laparotomy, and 32 cases of laparoscopy-assisted surgery (Table 1). Between the three treatment groups, there were no significant differences in gender, age, and clinicopathological characteristics. For all of the cases, the malignancies were confirmed by endoscopy before surgery, pathological examination of tumor biopsies, and postoperative TNM staging as stages II and III. The study excluded any patients during pregnancy and those who manifested multiple organ failure and other surgical complications. The study also did not recruit patients with unmatched pre- and postoperative pathological findings, distinct metastasis at the liver or other organs, cancer invasion into pancreas and colon, tumor recurrence, preoperative abdominal edema, or tumors with a diameter >5 cm.
Comparison between three treatment groups.
TULS, three united laparoscopic surgery.
Hand-assist device
The design of our patented hand-assist device is depicted as in Figure 1. Simply, the device consists of an outer elastic ring, a sealed connector, an inner elastic ring, and a sac-like sealed sleeve. The sleeve connects with the inner elastic ring on one end and has two inlets: one for the placement of the surgical instrument and one for the insertion of the surgeon's left hand.
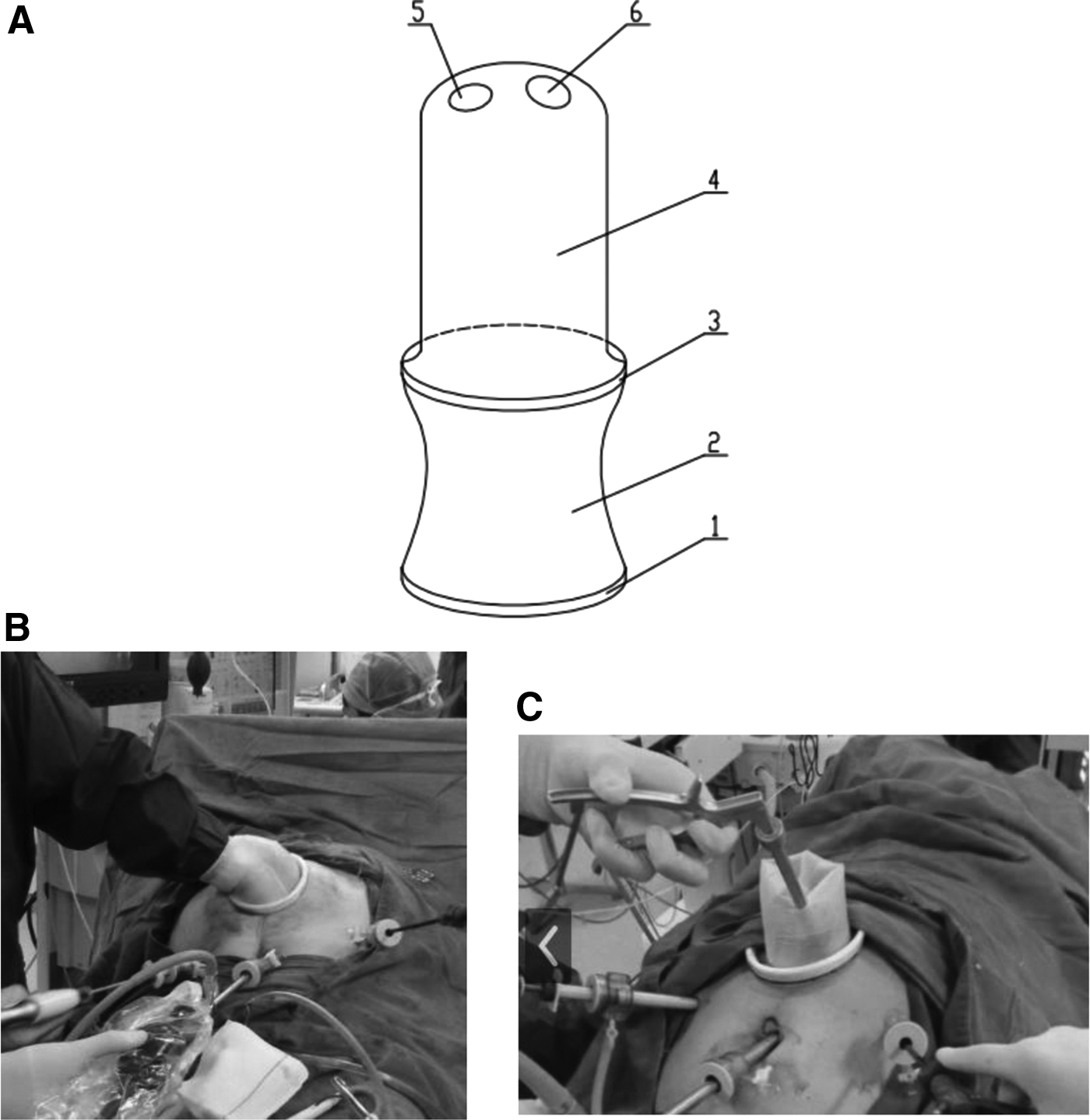
Diagram depicting the design of the hand-assist device and its use in TULS.
Surgical procedures
Three united laparoscopic surgery
The patients received anesthesia and were placed supine. The operator stood at the right side of the patient (typically near the patient's head). The first assistant stood at the left side of the patient, whereas the second assistant (endoscope holder) stood at the right side of the patient (typically near the patient's foot). A 10 mm incision was made left to the umbilicus to establish pneumoperitoneum at 12 mm Hg, and to place a 10 mm trocar. The laparoscope was inserted through the trocar to observe the presence of hepatic metastasis, intraabdominal metastasis, and omental nodules in the abdominal or pelvic region. A 5 mm trocar was inserted 2 cm below the ribs at the left anterior axillary line by the first assistant. A longitudinal incision at a hand's width was made at the upper mid abdomen below the xiphoid process, and the size, position, and metastatic status of the tumors were further examined by hand. The mid-transverse colon and the greater omentum were retracted out of the incision. Then, the greater omentum and the transverse mesocolon were dissociated along the transverse colon in both directions until the hepatic flexure and the splenic flexure were reached. Lymph nodes at station 4d and 6 were first removed, followed by lymph nodes at 4sb. The greater omentum was folded over and returned to the peritoneal cavity. A patented connector, with a sealed sleeve, was then inserted at the incision to facilitate the entry of surgical instruments. A 12-mm trocar was inserted at the right midclavicular line 2 cm superior to the umbilicus that the operator used to maneuver instruments. Through the patented connector, a device was placed to retract the left lobe of the liver. The hepatogastric ligament was excised along the inferior border of the liver to the right of the cardia, and lymph nodes at stations 1 and 3 were removed. The laparoscopic instrument was then removed from the connector, and the left hand of the surgeon was entered through the connector. The gastrosplenic ligament was transected, and the greater curvature of the stomach was dissociated to the left of the cardia. The remaining lymph nodes at station 4sb and 4sa were removed; then, the hepatic artery, the celiac trunk, the proximal splenic artery, and the left gastery were dissociated and exposed. The left gastric vein and coronary vein were clamped at the root and transected. Lymph nodes at stations 7, 8, 9, and 10 were removed. The retrogastric tissues were dissected until the posterior part of the esophagus was reached and the crura of the diaphragm were exposed. The lymph nodes at station 12a were then dissected under direct vision through the longitudinal incision at the upper mid abdomen. The lymph nodes at station 5 were removed along the right gastric artery. The esophagus was transected with a purse string clamp at about 4 cm above the tumor at the cardia. The stomach was retracted outside of the incision. An endolinear strapler was used to excise the antrum along the predefined cutting line. A 3 cm incision was made in the anterior wall of the remnant stomach, and a 26 mm circular anastomosis stapler was inserted into the stomach through the incision. The esophagus and the remnant stomach were anastomosed with the stapler. The incision in the remnant stomach was sutured with an absorbable 3-0 suture. Total gastrectomy was done, and gastrointestinal continuity was rebuilt in a Roux-en-Y fashion. The abdomen was finally closed once the drainage tube was placed.
Laparoscopy-assisted surgery
The patients received anesthesia and were place supine with legs apart. The operator stood at the right side. The first assistant stood at the left side of the patient, whereas the second assistant (endoscope holder) stood between the patient's two legs. Briefly, a 10 mm incision was made left to the umbilicus to establish pneumoperitoneum at 12 mm Hg, and to place a 10-mm trocar for laparoscopy. A 10-mm trocar was inserted 2 cm below the costal margin at the left preaxillary line. Then, a 5-mm trocar was placed at the left midclavicular line parallel to the umbilicus, and another 10-mm trocar was inserted at the contralateral site. The last 5-mm trocar was placed at the right preaxillary line 2 cm below the costal margin. The presence of hepatic metastasis, intraabdominal metastasis, and omental nodules in the abdominal or pelvic region was observed. After the removal of lymph nodes sequentially at stations 4d, 6, 2, 4sb, 2, 4sa, 7–11, 1, 3, 12a, and 5, an upper midline incision with a length of about 8 cm was made. The gastrectomy was done, and gastrointestinal continuity was restored as in TULS.
Laparotomy
Open abdominal surgery was performed as described, 7 and a 20-cm incision from the xiphoid process to the left of the umbilicus was made. Gastrectomy, lymph node dissection, and gastrointestinal reconstruction were then performed as in TULS and laparoscopy-assisted surgery.
Clinical data collection and statistical analysis
The following clinical data of each patient were collected: length of surgery, amount of bleeding recorded by anesthetists, length of incision, number of lymph nodes removed, time to flatus, complications after surgery, and hospital stay and expense. Data were analyzed by using SAS version 9.3. Measurement data were presented as mean + SD, with comparisons between groups done by Kruskal–Wallis test. Qualitative data were compared by using Chi-squared or Fisher test. P value <0.05 indicated statistical significance.
Results
Patient clinicopathological characteristics
Demographic details of the three treatment groups are as listed in Table 1. Among a total of 100 cases of advanced gastric cancer, 38 patients received TULS, 30 patients received laparotomy, and the remaining 32 received laparoscopy-assisted surgery. In each of the treatment groups, the majority of patients had a tumor located at the gastric cardia. Between the three treatment groups, there are no significant differences in gender (P = .797), age (P = .889), tumor size (P = .141), location of tumor (P = .829), presence of enlarged paraaortic lymph nodes (P = .792), and history of abdominal surgery (P = .145).
Surgical conditions of TULS, laparotomy, and laparoscopy-assisted surgery
For each of the treatment groups, >90% of the patients were administered radical tumor resection (Table 2). We compared incision length, length of surgery, amount of bleeding, and number of lymph nodes removed between the three groups. As expected, TULS and laparoscopy-assisted surgery resulted in significantly shorter incision lengths compared with laparotomy. Lengths of surgery of TULS and laparotomy were comparable, and both were significantly shorter than that of the laparoscopy-assisted surgery. TULS led to a substantial reduction in bleeding during surgery compared with laparotomy. There were no differences in the number of lymph nodes removed between the three groups.
P < .05 compared with TULS.
P < .05 compared with laparotomy.
Comparison between three treatment groups.
TULS, three united laparoscopic surgery.
Postoperative characteristics of TULS, laparotomy, and laparoscopy-assisted surgery
Postoperative characteristics of patients of different treatment groups were analyzed (Table 3). TULS led to no postoperative complications at all; whereas for laparotomy and laparoscopy-assisted surgery groups, there were 4 and 1 patients inflicted with postoperative complications, respectively. The difference was found to be statistically significant (P = .023). Patients treated with TULS stayed in hospital after surgery for 8.87 ± 1.14 days, which was significantly shorter than those treated with laparotomy (10.9 ± 1.73 days) and laparoscopy (9.53 ± 1.39 days) (P < .001). However, TULS presented a longer time to flatus compared with laparoscopy-assisted surgery (P < .05). The hospital expenses of TULS-treated patients were less than those of patients treated with laparoscopy-assisted surgery, but they were slightly higher than those of the laparotomy-treated patients.
P < .05 compared with TULS.
P < .05 compared with laparotomy.
Comparison between three treatment groups.
TULS, three united laparoscopic surgery.
Discussion
In China, nearly 95% of gastric cancer cases are diagnosed with advanced malignancy at the first presentations of patients to clinics. Over the past decade, with the advancement of surgical instruments and techniques, the use of laparoscopic D2 dissection has been extended from early to advanced gastric cancer. Indeed, there are many studies indicating that laparoscopic D2 dissection is as efficient as laparotomy in radical tumor resection.8–10 A systemic study by Pugliese et al. demonstrated that laparoscopic D2 subtotal gastrectomy would achieve acceptable long-term clinical outcomes and 5-year survival. 10 In March 2009, our team successfully performed our first laparoscopic radical gastrectomy. Since then, we have completed nearly 300 laparoscopy-assisted surgeries, evidencing that the therapeutic efficacy of the laparoscopic approach is comparable to that of conventional laparotomy. However, in spite of these encouraging findings, the wide use of laparoscopy-assisted surgery for treatment of advanced gastric cancer remains to be established. Laparoscopic D2 resection is technically challenging. To ensure a clean dissection, a closed collaboration between a well-trained operator and assistants is required, but unfortunately, many medical centers are not accessible to such intensive training. As such, we invented a novel hand-assist device and developed a modified laparoscopic approach named TULS.
TULS demonstrates the combined advantages of laparotomy, laparoscopy, and hand-assisted laparoscopy. The present study showed that TULS could be finished significantly faster than laparoscopy, of which the operative time was comparable to that of laparotomy. The short operative time of TULS is believed to be attributed to the better vision achieved by the use of our patented hand-assist device. This advantage of better vision of TULS would be particularly useful in surgery for obese patients. Besides, TULS was shown to substantially reduce the amount of bleeding compared with laparotomy. This was likely due to the fact that with our hand-assist device, the surgeon can better locate the blood vessel with his hand and so minimize the risk of injuring the blood vessel. No significant differences in bleeding between TULS and laparoscopy-assisted surgery were observed. Despite this fact, we believe that TULS would be superior to the laparoscopic-assisted surgery in mitigating bleeding. The use of our hand-assist device facilitates the control of bleeding by pressing with the surgeon's hand. TULS also makes the transition into laparotomy, whenever necessary, rapid and safe. In addition, the combined use of pneumoperitoneum and endoscopy of TULS provides a better vision of the gastric cardia compared with laparotomy, in turn, lowering the risk of bleeding.
The numbers of lymph nodes dissected by laparotomy and TULS were almost the same as each other, suggesting that TULS is, undoubtedly, an efficient approach for lymph node dissection. This satisfactory performance of TULS may be likely due to its good vision as mentioned earlier. The laparoscopy-assisted surgery also yielded efficient lymph node clearance. TULS involves less surgical instruments than laparoscopy-assisted surgery, making it less likely to cause cancer cell shedding from the tumor and thus minimizing the risk of tumor recurrence and distinct metastasis. 11
The use of our patented hand-assist device in TULS was shown to be able to preserve the advantages of minimally invasive surgery. Our analysis unequivocally illustrated that TULS performed as well as the laparoscopy-assisted surgery in reducing time to flatus, hospital stay, rate of postoperative complications, and incision length compared with laparotomy. Notably, most TULS-treated patients could resume physical activity 2 days after surgery, and perhaps more importantly, no postoperative complications were reported in this group of patients. TULS did not result in any postoperative complications, because it could significantly reduce blood loss during surgery, and because of its small incision that could minimize the risk of wound infection. Abdominal wall hernia is a common postoperative complication in patients receiving laparotomy. Our data anticipated that TULS would lower the risk of hernia in a significant manner. Surprisingly, patients receiving TULS paid less compared with their counterparts who were treated with the laparoscopy-assisted surgery, although TULS cost a little bit more than laparotomy. The low cost of TULS would likely be a combined result of its fast recovery and short hospital stay, with fewer amounts of antibiotics, nutritional supplements, and medications used.
In the present study, a pairwise comparison between the learning curves of TULS and laparoscopy-assisted gastrectomy was not made. However, in view of the clinical advantages gained by the use of the novel hand-assist device, we believe that the number of cases of TULS required to achieve optimum proficiency is likely smaller than that of laparoscopy-assisted surgery. On the other hand, our hand-assist device helps surgeons to build up their skills and confidence in minimally invasive surgery. The device greatly facilitates the placement of surgical instruments, rendering surgeons much ease in the transition from conventional laparotomy to laparoscopy-assisted surgery. It also demonstrates a high degree of flexibility, because it allows a rapid switching between laparoscopy and hand-assisted laparoscopy, and whenever necessary, changing to laparotomy from laparoscopy by increasing the incision length.
Taken together, TULS has been demonstrated as a safe, efficient, and cost-effective surgical approach for radical resection of tumors located in the cardia of the stomach. With the use of our novel and patented hand-assist device, TULS preserves advantages of minimally invasive surgery without compromising its efficacy of tumor resection. TULS is less traumatic than laparotomy. Compared with laparotomy, TULS causes less bleeding and lowers risk of postoperative complications, shortening hospital stay and, in turn, reducing medical expense. To promote TULS as the frontline surgery for patients with gastric cancer, the safety and feasibility of TULS will be examined in larger patient cohorts from multiple centers.
Footnotes
Disclosure Statement
No competing financial interests exist.