
Abstract
Abstract
Introduction:
As an advanced minimally invasive surgical procedure, the repair of the diaphragmatic hernia may sometimes be very challenging especially when the anatomy is unclear.
Materials and Methods:
We are presenting a rare case of a parahiatal hernia defect repair where the understanding of the anatomy was complicated by the presence of an unusual large sized left inferior phrenic artery. The Da Vinci surgical platform was used to perform the entire procedure. Hernia sac dissection, identification of the crura, primary closure of the defect, and use of biologic mesh reinforcement were the main steps performed in the usual manner for hernia repair. In addition, the use of intraoperative ultrasound was of great utility to clarify the vascular anatomy.
Results:
The additional time required for the intraoperative ultrasound and identification of the vascular anatomy has increased the duration of the procedure that otherwise was uneventful. The accurate identification of the anatomy allowed for a safe surgical outcome. The postoperative course was favorable and patient was free of symptoms at 1-month follow-up.
Conclusion:
The challenge of the repair of this rare, parahiatal type of diaphragmatic hernia where a large sized left inferior phrenic artery was also encountered was successfully mitigated by the use of the intraoperative Doppler ultrasound and by compliance with the basic steps of the procedure.
Introduction
T
Case Report
A moderate sized left diaphragmatic hernia was incidentally found on imaging studies performed for a 45-year-old female with upper abdominal pain. She had a medical history consistent with focal nodular hyperplasia of the liver and a surgical history relevant for laparoscopic cholecystectomy. The ongoing chronic upper abdominal and back pain along with discomfort during deep inspiration, which were persisting after cholecystectomy and without other identifiable cause over 6 months of workup, has urged the decision for surgical repair. She underwent elective robotic repair of the diaphragmatic hernia with reduction of the herniated contents, resection of the hernia sac, primary closure of the diaphragmatic defect, and reinforcement with Bio A mesh. The Da Vinci Si surgical platform was used to perform the entirety of the operation. The pneumoperitoneum was created and the patient was placed in reverse Trendelenburg position with the left side up 30°. The robotic cart was docked from the head and the arms 1, 2, and 3 were placed as shown in Figure 1. Assistant port was placed initially between the camera and arm 1, this was initially an 8 mm port, and was changed later to a 12 mm port to accommodate the ultrasound probe. The following instruments were used for the procedure: monopolar curved scissors, fenestrated bipolar forceps, Cadiere forceps, small graptor, vessel sealer, hook cautery, and large SutureCut needle driver.
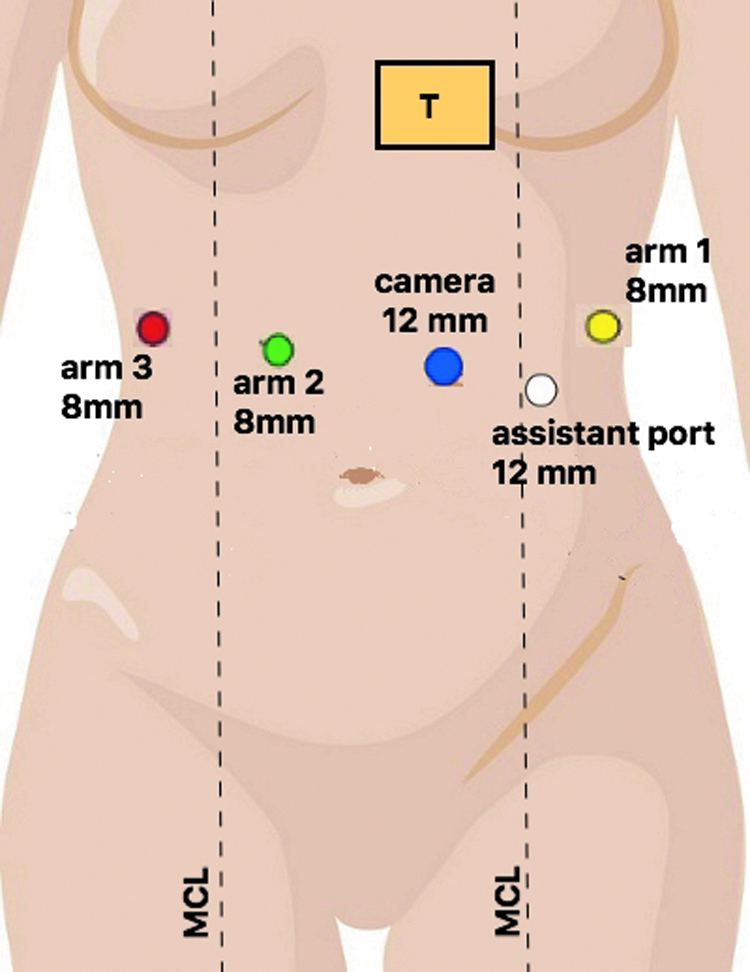
The trocar disposition for the procedure. MCL, midclavicular line; T, target area (the diaphragmatic defect); the robotic cart was docked from the head.
At a primary inspection, the patient did have a hernia lateral to the left crus containing stomach (Fig. 2). The stomach was easily reduced and the hernia sac was completely excised. A vessel sealer was used to divide the short gastric vessels so that the fundus of the stomach was fully mobilized and separated from the spleen. The pancreatic tail and splenic artery were noted to be fairly close to the hernia defect. The right and left diaphragmatic crura were identified and they appeared to be in the right anatomical position and no hiatal defect could be found. The esophagus was coursing normal between the crura. A penrose drain was placed around the gastroesophageal junction to include the esophagus and the vagus nerves. This was retracted toward the right to expose the defect. No hiatal hernia could be found.
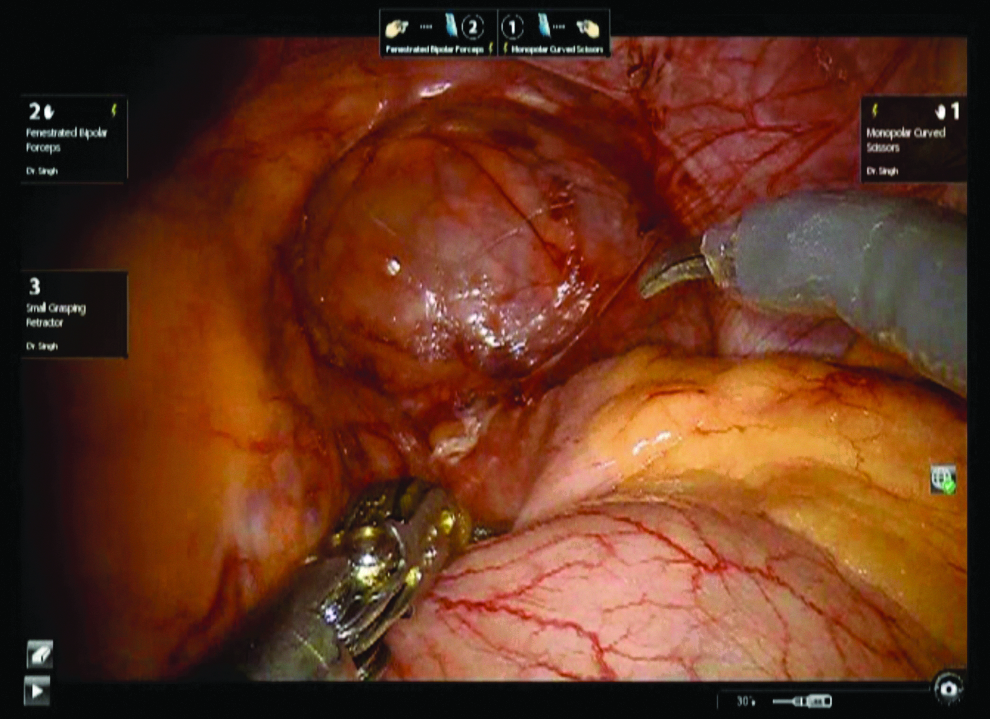
The diaphragmatic (parahiatal) defect after the stomach was reduced in the peritoneal cavity.
The defect was parahiatal, located entirely left lateral from the left crus, and once the sac was removed, we could identify a flimsy, thin, layer of tissue that was lacking musculature, in an area where we would have expected to find diaphragm structure. Further dissection of this structure led to a small opening in the pleura. We concluded that this tissue was either a poor developed diaphragmatic tissue or a redundant pleura or a combination of these two with a firm coalescence between the layers (Fig. 3). The confusion was further stressed when during the dissection of this tissue, we have found a vascular structure fairly significant in size, of almost 8 mm diameter, that was pulsating and had an arterial appearance, almost looking like the celiac artery. However, it did not seem to course over toward the stomach as it was coursing cranially toward the mediastinum parallel to the esophagus and was situated lateral to the left crus (Fig. 4a–c).
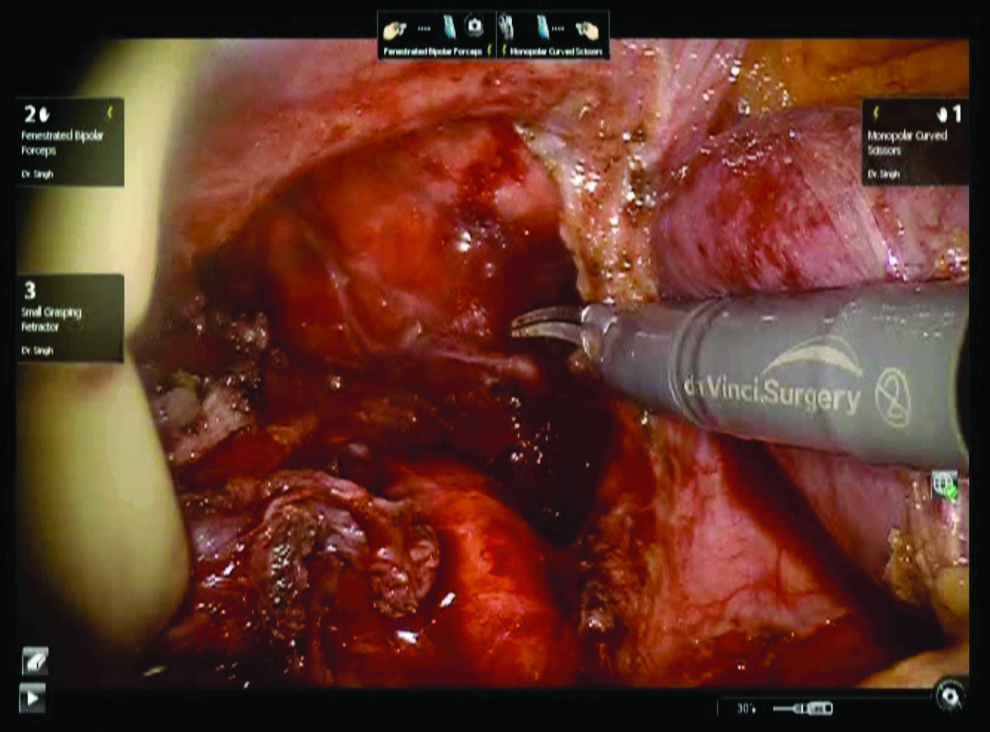
The hernia defect after the hernia sac was excised exposing the pleura. The diaphragmatic tissue was basically absent at this level and the pleura was fused with the hernia sac consisting of the diaphragmatic peritoneum. On the right side, the penrose drain can be seen retracting the esophagus toward the right to expose the defect.

At this point, intraoperative Doppler ultrasound was performed. The superior mesenteric artery was identified, as well as the celiac artery along with its branches, which were located below the area of the hiatus. This large vascular structure was arising laterally off the aorta and it was coursing toward the phrenic vein and it was, therefore, a large sized left inferior phrenic artery (Fig. 5a–e). Once the vascular anatomy was identified, we have proceeded to close the diaphragmatic defect. Ethibond 0 suture was used to approximate the diaphragm to itself and then diaphragm to the left crus (Fig. 6a, b). There was absolutely no tension on this area. As we sutured the defect of the diaphragm to the left crus, this did widen the hiatus a little bit. The angle of His was left intact. The hiatus was then reinforced with GORE® BIO-A® Tissue Reinforcement biosynthetic mesh that was affixed to the diaphragm with Ethibond 0 suture. The option was not to perform fundoplication at all as the patient did not have any reflux symptoms and the geometry of the angle of His was not modified during the surgery. At 1 month follow-up visit, the patient was free of symptoms.

Intraoperative ultrasound with precise identification of all the vascular arterial structures from the area:

Closure of the defect:
Discussion
Congenital diaphragmatic hernias include retrosternal-anterior, Morgagni (in the right side), Larrey (in the left side), posterolateral (Bochdalek), hiatal hernia subclassified to types 1 to 4, and parahiatal hernia. Parahiatal hernia is an exceedingly rare congenital abnormality, estimated at 0.2%, which results from muscular diaphragmatic defects separate from the esophageal hiatus. 1 It occurs as a result of incomplete closure of a normal pleural–peritoneal canal during embryonic development. 2 Previous diaphragmatic trauma or surgical manipulation can cause acquired diaphragmatic hernia. The vast majority of acquired diaphragmatic hernias are esophageal hiatal sliding hernias, whereas the less common form is a paraesophageal hernia mimicking a parahiatal hernia. 3 Given its rarity, published articles regarding preoperative diagnosis, treatment modality, and postoperative surveillance are scarce.
Our patient had a diaphragmatic defect on the left side of the esophagus that was clearly distinct from the esophageal hiatus, from which it was separated by the left diaphragmatic crus. Hence we consider it as a pattern of incomplete closure that generated the hernia, or a very weak closure with poor representation of the diaphragm at that area. The aforementioned incomplete closure of a normal pleural–peritoneal canal during embryonic development or persistence of pleuroperitoneal communication is a natural history of parahiatal hernia. Therefore, we could classify our case as a parahiatal hernia. We postulate that the diaphragm anomaly might relate to the abnormal trajectory of the inferior phrenic artery that coursed more toward the hiatus than the diaphragm, which was poorly represented. With the difficult identification of local anatomy, the enlarged left inferior phrenic artery and abnormal route make this rare case particularly interesting.
In general, patients with symptomatic diaphragmatic hernias should undergo surgical intervention to improve patient's quality of life and to prevent potential complications such as perforation, bleeding, or volvulus that could be associated with high morbidity and mortality. 4 The main purpose of surgery is to reduce the herniated organs to their normal anatomy to reduce the associated symptoms such as heartburn and abdominal pain and to prevent recurrence by the closure of the diaphragm defect. First, both crura are identified. Dissection of hernia sac is undertaken with great care to preserve the vagal nerve, esophagus, and pleura. Complete resection of the peritoneal sac is performed routinely. In general, based on the size of defect and tissue integrity, simple cruroplasty or prosthetic hiatal herniorrhaphy is utilized. Recent meta-analysis by Stavros et al. has demonstrated the superiority of mesh hiatoplasty over primary closure in terms of hernia recurrence. Recurrence rate ranged between 22.2% and 26% for the primary closure and between 0% and 8.9% for the mesh repair. 5 However, because of lack of high-quality data on the incidence of adverse effects of mesh hiatoplasty, routine application cannot be recommended. Moreover, cases of mesh erosion and migration through the esophageal wall have been reported sporadically. 6 As they are very rare, there are no studies to evaluate the utility of mesh particularly for the parahiatal type of diaphragmatic hernias. Technically, to close the defect in the sagittal plane, it is required to approximate the left edge of the defect to the left crus, a maneuver that can cause a somewhat unwanted enlargement of the hiatus especially if the tension in the suture is considerable. We felt that our closure was free of tension, but still we could notice a tendency of the hiatus to enlarge (Fig. 6a). Therefore, we considered placing a biologic mesh for reinforcement.
Several studies have demonstrated that laparoscopic hiatal repair is both safe and effective.7,8 However, laparoscopic giant hiatal hernia is a technically demanding procedure that requires advanced laparoscopic skills, especially during the dissection of the huge sacs and mobilization of the esophagus in the mediastinum. Robotic surgery with optimized ergonomics, better three-dimensional vision, and finest endowrist instruments has allowed surgeons to overcome some of the technical limitations of the conventional laparoscopic surgery. A prospective study for robotic giant hiatal hernia in a single institution showed favorable outcomes in terms of anatomical recurrence and quality of life. 4 A recent case–control study by Gehrig et al. has demonstrated that robotic-assisted surgery appears to be an alternative to open surgery due to lower intraoperative blood loss and potentially fewer postoperative complications as well as shorter hospital stay. However, robotic-assisted surgery is not superior to conventional laparoscopic surgery. 9
The right and left inferior phrenic arteries originate as a common trunk or separately mostly from the abdominal aorta or the celiac trunk, renal artery, rarely from the left gastric artery, hepatic artery, superior mesenteric artery, or contralateral inferior phrenic artery. They give two main branches. The posterior branch traverses parallel to the lower border of the lumbar part of the diaphragm, where the ascending branch arises from the level of the vena cava and esophageal foramina on the right and left sides. 10 A previous study indicated that the normal diameter of the right inferior phrenic artery and left inferior phrenic artery is 2.2 mm (range 1.4–3.2 mm) and 2.0 mm (range 1.4–2.8 mm), respectively. 11 Apart from being the main blood supply for the diaphragm, the right and left inferior phrenic arteries are the main extrahepatic collateral arterial pathways that supply the hepatic malignancies. The inferior phrenic artery can be one of the systemic-pulmonary artery anastomosis, especially when the pulmonary abnormality involves the lung base. 11
We encountered the hypertrophic left inferior phrenic artery with abnormal trajectory, which might have been confused with other major vascular structures from the area. The usage of Doppler ultrasound intraoperatively helped in identification of the superior mesenteric artery, celiac artery with all its branches, and phrenic artery accurately (Fig. 5a–e). The size of the artery was constant all throughout its course and it did not have aneurysmal appearance. Complications are to be expected after embolization of the inferior phrenic artery. These include abdominal or referred shoulder pain, pleural effusion, atelectasis, hiccups, and ipsilateral diaphragm weakness.11,12 Furthermore, gastritis, esophagitis, and ulceration might develop if the gastric and esophageal branches of the left inferior phrenic artery are affected. 13 Therefore, we opted to preserve the artery instead of ligating it.
Conclusion
This is the first communication to report an unusually enlarged left inferior phrenic artery generating confusion during repair of a rare, parahiatal type of a diaphragmatic hernia. The difficulty was caused by an abnormal sized phrenic artery with an unusual course. The meticulous dissection and intraoperative Doppler ultrasound allowed for precise anatomical identification and the repair could be performed accordingly. Using the Da Vinci robotic platform with tridimensional view, magnification, and increased dexterity has facilitated the anatomical dissection and the repair of the defect.
Footnotes
Disclosure Statement
No competing financial interests exist.