
Abstract
Abstract
Background:
Omega loop gastric bypass is a successful bariatric surgery with numerous favorable circumstances as being basic, effective on weight reduction and treatment of obesity associated metabolic disorder, the short expectation to learn and adapt, and the simplicity of correction and inversion. However, there are arguments about the possibility of biliary reflux and/or the potential danger of gastroesophageal malignancy after the procedure.
Methods:
Fifty patients experiencing morbid obesity with body mass index >40 or >35 kg/m2 with two related comorbidities, for example, diabetes type II, hypertension, or dyslipidemia, underwent omega loop gastric bypass with a follow-up period up to 18 months, investigating for any symptom of reflux infection by upper gastrointestinal tract endoscopy and pH metry.
Results:
Reflux esophagitis (a gastroesophageal reflux disease) was detected in 3 patients (6%); 2 cases (4%) showed (Grade A) acidic reflux esophagitis at 6 and 12 months postoperatively. Just 1 case (2%) had experienced gastroesophageal biliary reflux esophagitis (Grade A) at 12 months. No metaplasia or dysplasia was detected in the endoscopic biopsies.
Conclusion:
Omega loop gastric bypass is a safe and effective bariatric procedure with low incidence of postoperative biliary reflux, metaplasia, or dysplasia at the esophagogastric junction, confirmed 18 months after the operation.
Introduction
O
The current treatments of morbid obesity are not limited to eating, routine regimens, and exercises, but rather bariatric surgery has turned into a significant and successful approach for weight reduction and the treatment of obesity-related complications and the improvement of patients' quality of life. 3
Omega loop gastric bypass was developed in 1997 by Robert Rutledge as an alternative to standard Roux-en-Y gastric bypass procedure, which has the benefit of being simple and easy to perform with minimum risk of leakage and internal herniation.4,5 The omega loop gastric bypass has both a restrictive function by reducing food intake, as well as a malabsorptive function. 6
Despite that, there is a debate around possible complications associated with omega loop gastric bypass, such as metaplasia, dysplasia, and even a carcinogenic effect of biliary reflux on the gastric pouch and the esophagus.7,8 That said, some studies concluded that the long gastric pouch is believed to reduce the risk of the biliary reflux on the esophagus.9,10
This study is, therefore, aiming to evaluate the incidence of biliary reflux after laparoscopic omega loop gastric bypass and its effects on the esophagus and the gastric pouch by both upper gastrointestinal tract (GIT) endoscopy and pH metry.
Patients and Methods
This is a prospective study that was performed on 50 patients (32 females and 18 males) with an age ranging from 19 to 50 years and having morbid obesity with body mass index (BMI) >40 or >35 kg/m2 with two related comorbidities, for instance, diabetes sort II, hypertension (HTN), or dyslipidemia. Between May 2013 and January 2016, a laparoscopic omega loop gastric bypass was performed for all patients in the Bariatric unit at the Surgery Department of El Demerdash hospital, Ain Shams University in Cairo, Egypt. An approval from Ethics Committee of the faculty of Medicine at Ain Shams University was acquired, and an educated composed assent was obtained from each patient preceding the operation.
Patients included in our study had a BMI > 40 or >35 kg/m2 with comorbidities, such as diabetes type II, HTN, or dyslipidemia, in addition, had previously experienced two failed trials of weight reduction amid the year before the operation. Patients who were unfit for general anesthesia or had a history of personality disorder and drug or alcohol addiction, had a recent cardiac attack or advanced malignancy, or underwent a previous Bariatric surgery were excluded from our study. Furthermore, patients who had any upper gastrointestinal endoscopic abnormalities such as reflux esophagitis, gastritis, peptic ulcer, duodenitis, or uncooperative patient during follow-up period were also excluded.
Before the operation, all patients were assessed by a medical team consisting of a GIT physician, Bariatric surgeon, psychiatrist, endocrinologist, and a dietician to evaluate the general condition, mental status, and obesity-associated comorbidities such as diabetes, hypertension, or cardiovascular diseases of each patient. An upper gastrointestinal endoscopy was performed for all our patients to exclude asymptomatic gastroesophageal reflux and to take biopsies from any suspicious lesion either in the esophagus or the stomach.
One week before the operation, patients were advised to take a high protein diet, and the day preceding the operation they were just permitted to take clear liquids.
During the operation, patients were placed in a 30° reverse trendelenburg position. A Veress needle was inserted 2 cm below the left subcostal region on the midclavicular line to induce pneumoperitoneum. The first 10-mm trocar for the camera was placed at the point between the upper 2/3 and the lower 1/3 of the line drawn from the xiphoid and the umbilicus. The second and the third trocars (12 mm) were placed on the midclavicular line to the right and left 5 cm away and above the port of the cam. The fourth trocars (5 mm) were placed in the right hypochondrium at the anterior axillary line, the fifth trocar (5 mm) was inserted in the left hypochondrium symmetrical to the previous one just below the costal margin, and finally the last trocar (5 mm) was placed underneath the xiphoid process at midline for liver retractor.
An opening was created along the lesser curvature at the level of incisura angularis to enter the retrogastric space. Through the created opening, a 45 mm linear stapler was applied along the right port (12 mm), and the stomach was stapled transversely at the level of incisura, then a 36F bougie was inserted along the lesser curvature. Sixty millimeter linear staplers (4–5 staplers) were applied along the bougie axis toward the gastroesophageal junction. After the creation of the long tube gastric pouch, the patient's position was changed to trendelenburg position. The transverse mesocolon was retracted toward the head of the patient and then 200 cm of the jejunum was measured from the ligament of Treitz and an antecolic side to side gastrojejunostomy was performed with 45 mm linear stapler. The stapler enterotomy was closed with a Vicryl 2/0 continuous stitch. A nasogastric tube was placed in the gastric pouch, and the leak test was performed by injecting 50–100 cc of methylene blue. The nasogastric tube was removed at the end of the operation.
Early ambulation was highly advised 4–6 hours after the operation, and a prophylactic dose of an anticoagulant was started 12 hours after the operation. Intravenous (I.V.) fluids, broad-spectrum antibiotics, and analgesics were given after 2 days of the operation. Gastrografin meal was performed for early detection of any leakage. All patients were not allowed to take any fluid orally for 48 hours, followed by low-calorie clear liquids for 1 week, and low-calorie semisolid food for 2–4 weeks after the operation. Full diet was subsequently introduced.
Before discharge, a proton pump inhibitor was prescribed for at least the first 3 months after operation, and daily multivitamins and supplemental minerals were recommended for life.
Patients were followed up for a year and 6 months in the outpatient clinic through weekly visits for 1 month after clinic discharge, monthly visits till the end of the third month, and one visit at regular intervals till the end of the subsequent period. At every visit, patients were assessed through full clinical appraisals, weight reduction estimations, and full evaluations of any reflux manifestations or protestations, for example, heartburn, dysphagia, and/or disgorging.
Upper GIT endoscopy was performed for all patients after 6, 12, and 18 months of the operation to identify any inflammation or ulcers and to take biopsies from any suspicious lesion. Twenty-four hour esophageal pH metry was done if any abnormalities were detected by the endoscopy, to measure the level of stomach acidity and to detect the presence of bile in stomach and the esophagus and the rate of its clearance downward into the stomach. During the assessment of distal esophageal pH, the sensor was placed at 5 cm above the upper border of the lower esophageal sphincter guided by esophageal manometry, while during the assessment of proximal esophageal pH, the second sensor was placed at 15 cm above the lower esophageal sphincter.
Esophageal pH estimations near 7 were viewed as ordinary, while a reflux episode was diagnosed when esophageal pH drops beneath 4. The esophageal pH checking was recorded in 24 hours, and toward the end of recording, patients tracing was analyzed and the outcomes were communicated with six standard segments, including percent total time pH, percent upright time pH, percent supine time pH, number of reflux episodes, number of reflux episodes that lasted for 5 minutes or longer, and the longest reflux episode in minutes. Of these six parameters, a pH score called DeMeester Score has been figured, which represents the global measure of esophageal acid exposure. A DeMeester score below 14 is viewed as typical, while a score >14.72 shows a reflux.
Results
Fifty recipients were selected for this study, consisting of 18 male patients (36.0%) and 32 female patients (64.0%). The mean age of the participants was 35.5 years that ranged between 19 and 50 years (Table 1).
The mean operative time was 90 ± 12.6 minutes (ranged between 80 and 120 minutes), and the mean period of hospitalization was 2 ± 2 days (ranged between 2 and 4 days). Only 1 patient required an overnight ICU admission. There were no surgical or procedure-related mortalities within the entire study group during the follow-up period.
At the time of follow-up upper GIT endoscopy, 2 patients indicated lower end esophagitis (Grade A) following 6 and 12 months of the operation and 1 patient demonstrated perianastomotic gastritis and diffuse pouchitis with no esophageal abnormality following 12 months of the operation. The 3 cases were investigated for gastric and esophageal pH by 24-hour esophageal pH metry. Acidic gastritis was affirmed in the patient that demonstrated lower end esophagitis (Grade A) following 6 months of the operation and in the patient with perianastomotic gastritis and diffuse pouchitis (Figs. 1 and 2), while gastroesophageal biliary reflux (soluble gastritis) was affirmed in the third patient that indicated lower end esophagitis (Grade A) following 12 months of the operation (Fig. 3). Different biopsies were taken from the 3 cases and were sent for histopathologic examination. The outcomes indicated nonspecific esophagitis with no dysplasia and metaplasia, and proton pump inhibitor was given for 3 months. Follow-up endoscopy was performed, and normal gastric mucosa was seen for each of the 3 cases (Table 2).
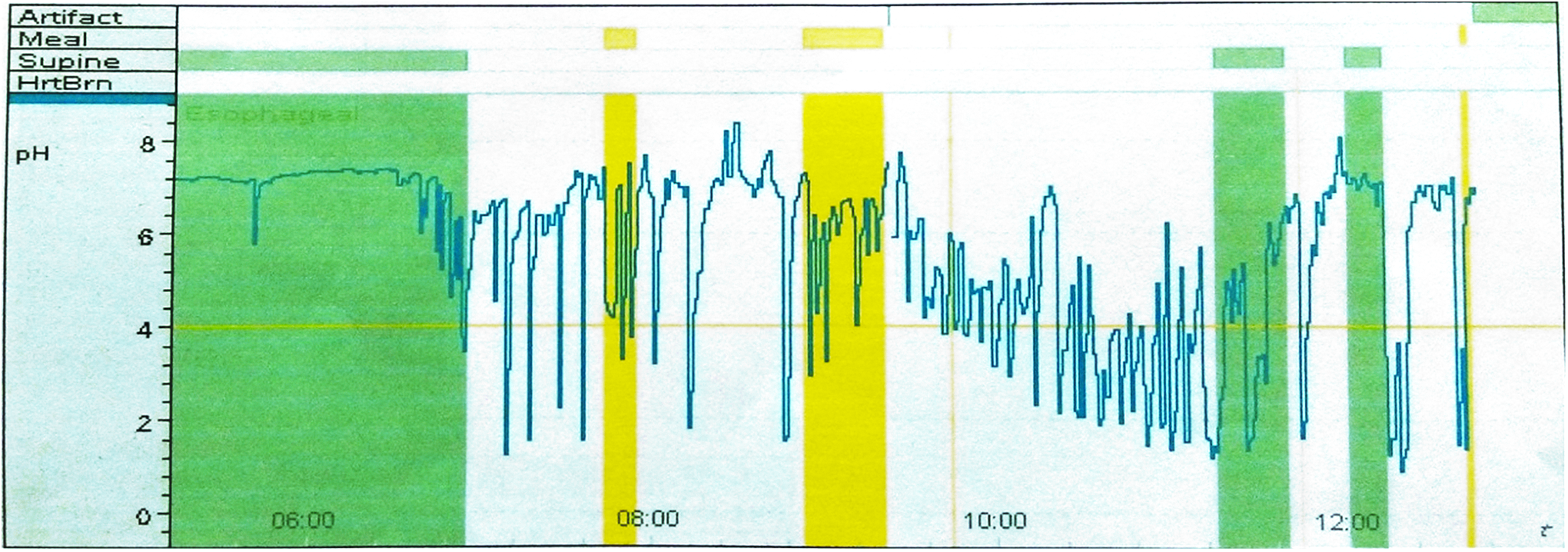
Patient with positive pH metry.

DeMeester graph scoring of patient with reflux gastritis.
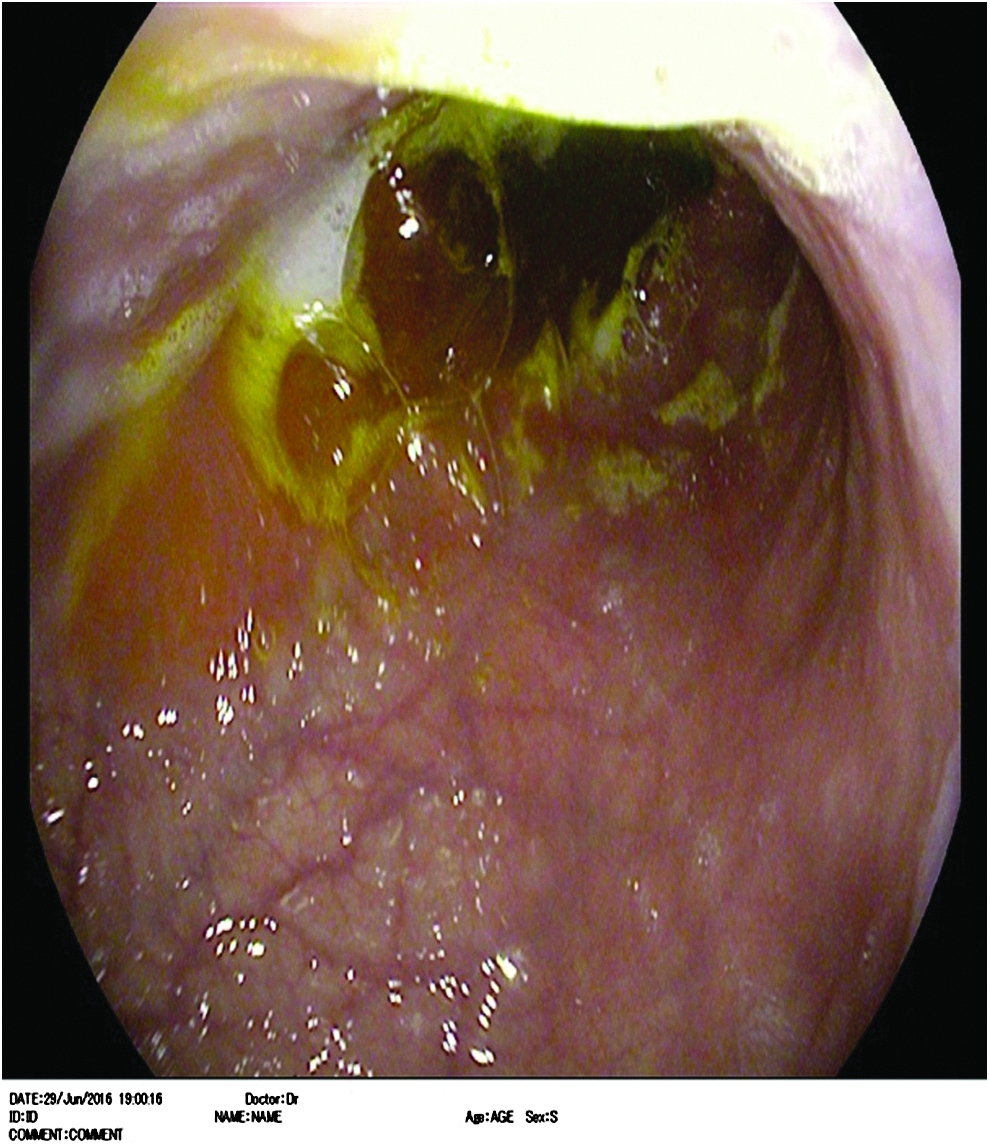
Mild biliary reflux pouchitis with Grade A esophagitis.
GIT, gastrointestinal tract; LMGB, laparoscopic mini gastric bypass.
Discussion
An omega loop gastric bypass is an effective surgical procedure for accomplishing weight reduction and can achieve results that are profoundly comparable to the results of typical Roux-en-Y gastric bypass. Likewise, it has the advantages of being straightforward and simple to perform and can effectively treat weight-related disorders, for example, hypertension, type II diabetes, and other comorbidities. 5 However, since it is a loop anastomosis system, it is connected with a few concerns in regard to possibility of biliary reflux and its impacts on remnant stomach and the esophagus. 11
There are a few fears concerning the biliary and pancreaticoduodenal reflux taking after omega loop gastric bypass (OLGB) that may lead to gastric and esophageal malignancies.6,10 In a study12,13 that was performed on creatures to explore the impacts of biliary and pancreaticoduodenal reflux on the gastric stump demonstrated that gastric stump carcinoma was detected in 10 out of the examined 14 creatures.
In our study, the frequency of postoperative gastroesophageal reflux was 6% (3/50 patients), which was similar to the results obtained by Tolone et al. 14 in which they evaluate the frequency of biliary reflux after OLGB using esophageal pH manometry and they found that there was a significant decrease in both acidic and biliary reflux in all patients. In addition, our finding was practically identical to that achieved by Rutledge et al. 5 in which they demonstrated that there were no pathological abnormalities along the esophagogastric junction and there was a decrease in the esophageal exposure time to the acidic and biliary reflux after OLGB.
In another study performed by Carbajo et al. 15 in which they investigate the gastroesophageal reflux utilizing 24-hour pH metry and through performing endoscopy after 12 and 18 months of a single laparoscopic anastomosis gastric bypass, they demonstrated that none of the examined patients had reflux symptoms after the operation.
Preceding the disclosure of Helicobacter pylori in 1984, 16 which is currently identified as the main cause for ulcers and gastric cancer, it was believed that gastric stump carcinoma after Billroth 2 gastrectomy was mainly caused by biliary reflux. However, biliary reflux can be a precipitating factor for carcinoma, but its effect alone without the activity of H. pylori is still not clearly defined. 17
In our study, the omega loop gastric bypass was performed on 50 patients with morbid obesity. The mean operative time was 115 minutes, while the mean period of hospitalization was 2 days, which were comparable to other studies.5,18,19
Although most of the concerns and fears of biliary reflux and its complications after omega loop gastric bypass were generally diminished, we still require more studies with longer follow-up period to assess the long-term impacts of reflux on both the gastric pouch and the esophagus.
Conclusion
From our results, we can conclude that omega loop gastric bypass is a safe and efficient bariatric procedure that is not associated with any significant incidence of postoperative biliary reflux, metaplasia, or dysplasia at the esophagogastric junction. However, studies with longer follow-up period and including a larger number of patients are recommended to investigate the long-term incidence of biliary reflux after omega loop gastric bypass.
Footnotes
Disclosure Statement
No competing financial interests exist.