
Abstract
Abstract
Background:
Total extraperitoneal (TEP) inguinal hernia repair gained popularity in the past two decades for its advantage, especially single incision laparoscopic surgery (SILS) for TEP inguinal hernia repair (SILS TEP), however, which is a technically demanding procedure.
Methods:
The study retrospectively analyzed 6 cases of the superior of inguinal ligament approach of S-SILS TEP repair from August 2015 to July 2016. A detailed review of medical records and the perioperative data including patient characteristics, operative details, and postoperative hospital stay was conducted.
Results:
S-SILS TEP repair for inguinal hernia was successfully completed for 6 patients, and the mean operation time was 59.2 minutes (range 55–70 minutes), and the mean blood loss was 7.5 mL (range 5–15 mL) and the postoperative recovery was uneventful about 3 days after operation with a single wound over inguinal ligament.
Conclusions:
S-SILS TEP repair provides a new operative view, which combines the advantage of laparoscopic and open surgery, especially in surgical technique and minimal invasiveness. Our experience suggests that the S-SILS TEP repair may be a safe and feasible alternative in inguinal hernias repair.
Instruction
T
Materials and Methods
Patients
From August 2015 to July 2016, 6 Chinese men with inguinal hernia underwent S-SILS TEP repair in our unit. All patients were coded according to the operation order, and a detailed review of medical records and the perioperative data including patient characteristics, operative details, and postoperative hospital stay was conducted. The characteristics of the patients are shown in Table 1.
BMI, body mass index.
S-SILS TEP technique
All patients underwent preoperative ultrasound examination to confirm sac size and hernia type. Under general anesthesia, the patients were placed supine with both arms adducted. A single 3-cm slant incision was made above the inguinal mass (Fig. 1). After slicing through the skin, subcutaneous tissue was separated by electrotome until obliquus externus abdominal muscle was exposed. Abdominal wall muscle was blunt dissection with vessel clamp, and we could find extraperitoneal space. Finger was put into the space and the blunt finger technique was used to expand extraperitoneal space as large as possible. A flexible port device (SILS™ Port; Covidien, Mansfield, MA) was inserted through the incision, and three 5-mm trocars were used (Fig. 2) and the extraperitoneal pressure was maintained at about 7 mmHg with carbon dioxide (CO2) gas. Under the guidance of a 5-mm laparoscopic camera, we further dissected the extraperitoneal space by detaching the surrounding soft and adipose tissue (Fig. 3). A polypropylene mesh (3D Max Light®; C. R. BARD, Murray Hill, NJ) was placed in the preperitoneal space (Fig. 4) covering the inguinal floor, and the blunt finger technique and laparoscopic technique were combined to flatten the mesh (Fig. 5). The external oblique muscle sheaths were closed with 3-0 absorbable suture, and the skin was closed with a 3-0 PDS suture (Fig. 6). Pain medicines were routinely used within 48 hours postprocedure.
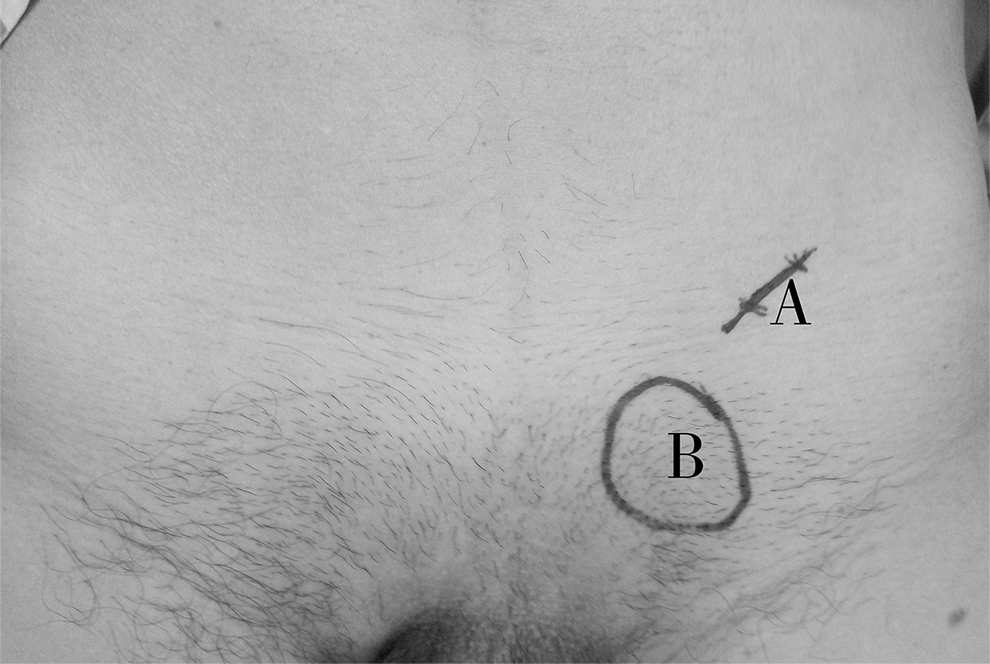

A flexible port inserted through the 3-cm incision.
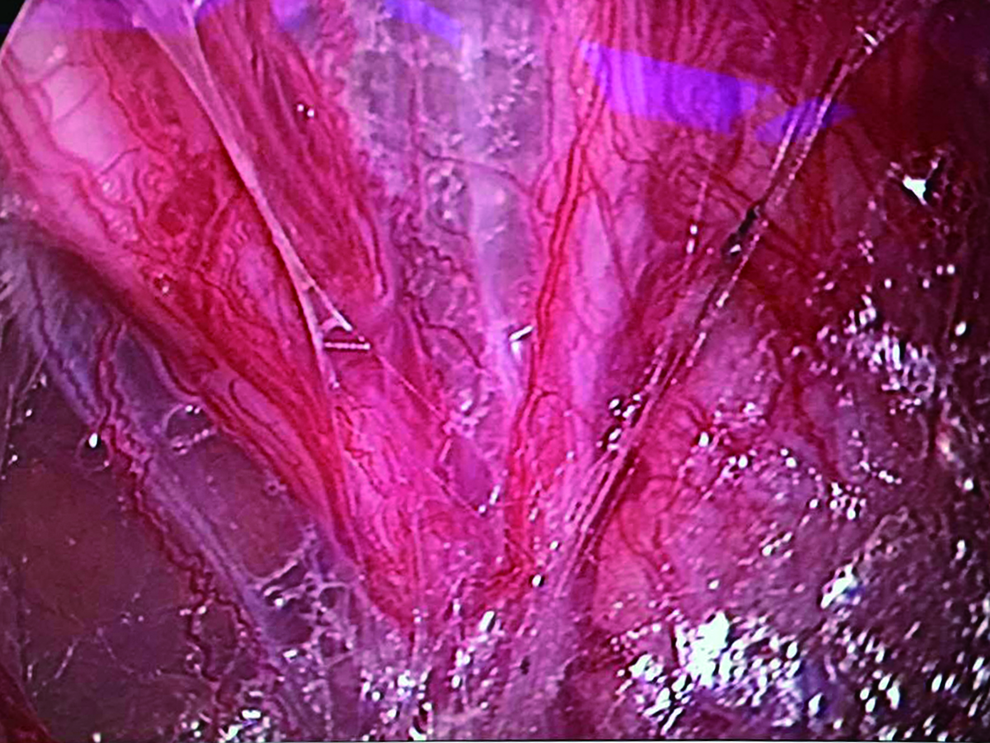
Detachment of extraperitoneal soft and adipose tissue.
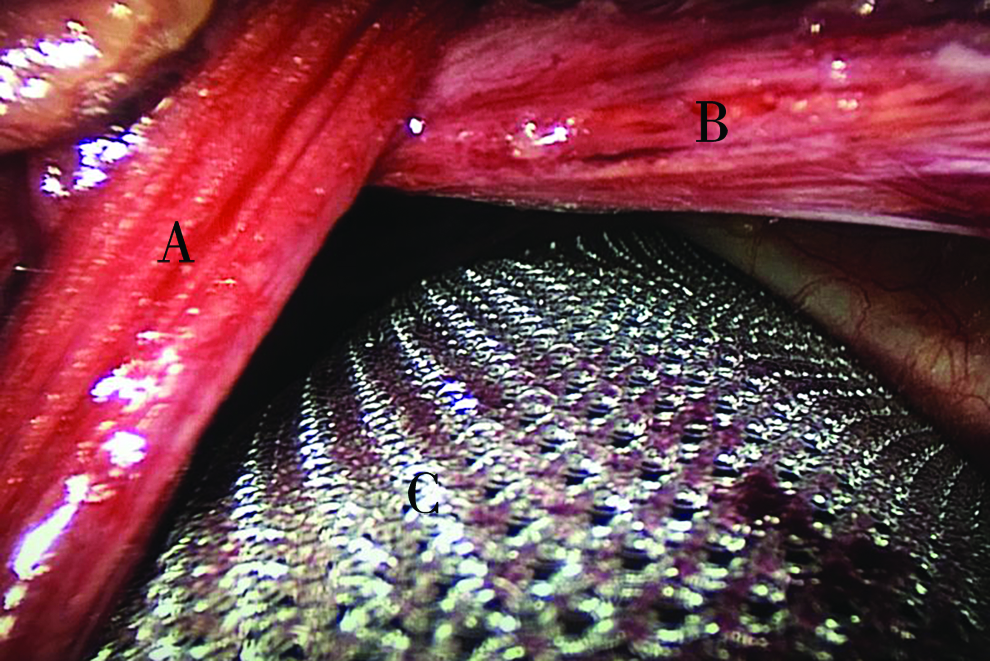
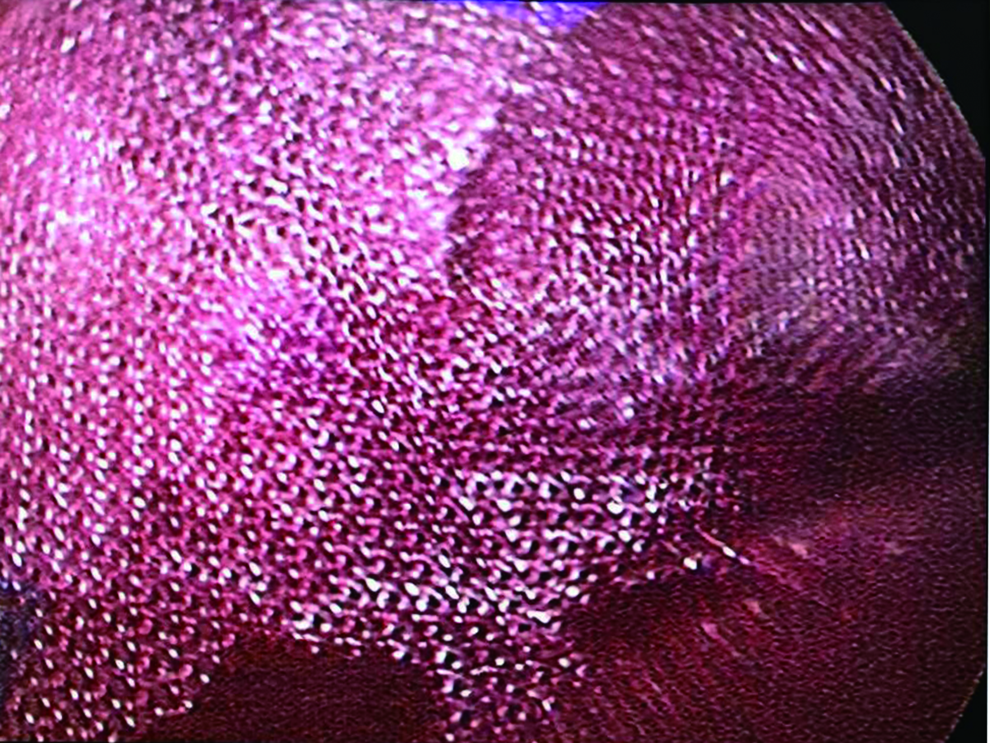
Mesh was flat after the blunt finger technique and laparoscopic technique.

Postoperative wound over the inguinal ligament after hernia repair.
Data collection
The patients' sex, age, body mass index, site and type of hernia, sac size, operating time, blood loss, postoperative hospital stay, pain medicine, incision infection, and numerical rating scale (NRS) after surgery in hospital were recorded. Pain was measured using an 11-point pain intensity NRS, where 0 = no pain and 10 = worst possible pain after surgery in hospital.
Results
All patients were successfully performed S-SILS TEP repair; intraoperative and postoperative data are shown in Table 2. The mean operation time was 59.2 minutes (range 55–70 minutes), the mean blood loss was 7.5 mL (range 5–15 mL), none of the patients experienced incision infection, and the postoperative recovery was uneventful about 3 days after operation.
NRS, numerical rating scale.
Discussion
Inguinal hernia repair is a frequently performed operation in general surgery. Compared with the tension-free repair, laparoscopic techniques have revolutionized the general surgical field. 3 The laparoscopic approach offers advantages in lower incidence of recurrence, less postoperative pain, and faster recovery. SILS TEP repair offers good cosmetic results in comparison with conventional three-port TEP repair. 4
Conventional SILS TEP is navel incision, which is a technically demanding procedure. In our experience, in S-SILS TEP an incision was made at the superior of inguinal ligament, which has advantages of clear field of vision and easy approach. To our knowledge, this is the first report of S-SILS TEP described in the literature. S-SILS TEP is safe and feasible, and this technique may provide a new operative view, but we still need to confirm whether it improves patient postoperative pain and complications and cosmetic results. Further studies are needed to evaluate this approach, especially in comparison with standard TEP and conventional SILS TEP.
S-SILS TEP may provide a new operative view, which combines the advantage of laparoscopic and open surgery, especially in surgical technique and minimal invasiveness. S-SILS TEP also offers cosmetic result. Our experience suggests that the S-SILS TEP technique may be a safe and feasible alternative in inguinal hernias repair.
Footnotes
Disclosure Statement
No competing financial interests exist.