
Abstract
Abstract
Objective:
To describe a newly developed transperitoneal intravesical technique for laparoscopic ureteral reimplantation in patients with terminal ureteral stenosis.
Methods:
Between July 2009 and May 2015, laparoscopic transperitoneal intravesical ureteral reimplantation was performed in 16 patients with terminal ureteral stenosis without vesicoureteral reflux (VUR). An incision was made in the superior bladder wall of the affected side with an electric hook. The bladder mucosa was then circumferentially cut away from the ureteral orifice to a distance of 0.5 cm, and the intramural portion of the ureter was freed from the bladder wall and dissected until 4 to 5 cm of terminal ureter was mobilized. The stenotic segment was resected, and a longitudinal cut was made in the mobilized ureter. The terminal ureter was then evaginated and sutured to the bladder wall to form a papilla. All patients underwent standard postoperative examinations.
Results:
All of the 16 operations were successful, and none required conversion to an extravesical approach or open surgery. The operation time ranged from 85 to 135 minutes (mean 98 minutes), and the estimated blood loss was ∼30–60 mL (mean 42 mL). There were no obvious intraoperative or postoperative complications. Resolution of hydronephrosis was achieved in all 16 patients, and VUR of the operated ureter was not detected at postoperative follow-up.
Conclusions:
The transperitoneal intravesical technique of laparoscopic ureteral reimplantation that we describe was safe and feasible in our 16 patients and may be an alternative surgical treatment for terminal ureteral stenosis in patients without VUR.
Introduction
D
Laparoscopic extravesical ureteral reimplantation was the earliest reported and most commonly used minimally invasive approach to the treatment of distal ureteral stenosis.5–13 However, there is a risk of voiding dysfunction after this procedure, especially in cases requiring bilateral ureteral reimplantation.7,10 In addition, in female patients, because the ureters enter the bladder proximal to the trigone and the stenotic segment is situated between the broad ligament and the base of the bladder, extravesical reimplantation inevitably disturbs structures within the pelvis.
Laparascopic methods had not been used for intravesical ureteral reimplantation until Yeung et al. reported a novel technique using pneumovesicum. 14 These transvesicoscopic techniques have since been widely developed and used,14–26 especially for the treatment of vesicoureteral reflux (VUR) in children and also for the treatment of distal ureteral stenosis. Other transvesicoscopic techniques have also been described; these also appear to be reliable and minimally invasive, but have the drawback of being complicated and time consuming.14–26
In the present study, we describe a transperitoneal technique for intravesical laparoscopic ureteral reimplantation and report the outcome of its use in 16 patients. To our knowledge, this is the first report of a laparoscopic transperitoneal intravesical reimplantation technique that does not require pneumovesicum and concomitant cystoscopy.
Materials and Methods
Patients
A total of 16 patients (16 ureters; 11 females and 5 males) with distal ureteral stenosis who underwent laparoscopic transperitoneal intravesical ureteral reimplantation between July 2009 and May 2015 were included in this study. All of the 16 patients had been diagnosed with stenosis of the terminal ureter and dilation of the ureter and renal pelvis. As shown in Table 1, the stenosis occurred on the right side in 9 patients, on the left side in 6 patients, and 1 patient had bilateral lesions. The mean patient age was 38.3 years (17–58 years).
Data in parentheses are percentages.
Nine of the patients, including the patient with bilateral lesions, were considered to have idiopathic ureteral stenosis, 5 patients had previously undergone ureteroscopic holmium laser lithotripsy for distal ureteral calculi on the stenotic side, and two developed hydronephrosis secondary to urinary tuberculosis. In the cases with urinary tuberculosis, the contralateral kidney with tuberculous pyelitis had been resected, and full-time antituberculosis treatment was adopted before and after resection. Thirteen of the patients complained of flank pain, and five had histories of fever.
Four patients had previously undergone placement of percutaneous nephrostomy tubes; these were placed due to high fever in 2 patients with histories of holmium laser lithotripsy and to preserve the solitary remaining kidney in the 2 patients with urinary tuberculosis. In 7 patients, double J (DJ) stents had been placed previously but turn out to be ineffective after being removed. The patient with bilateral lesions had a DJ stent in the right ureter, but a DJ stent had not been successfully placed on the left side with visible intraluminal stenosis during previous ureteroscopy. None of the patients had been treated by operations, except stent placement for the obstructed ureters.
The diagnoses were confirmed by B ultrasound, computed tomography, intravenous pyelography (IVP), and/or magnetic resonance urography. Voiding cystourethrography (VCUG) helped to rule out VUR. Ten of the patients had grade III hydronephrosis and six had grade IV hydronephrosis as assessed according to the guidelines of the Society for Fetal Urology. 27 Inclusion criteria were as follows: mild ureteral dilation that did not necessitate ureteral tailoring and a distance of less than 2.5 cm between the most proximal part of the stenotic region and the ureteral meatus (assessed by IVP). Patients with VUR were excluded.
The study protocol and procedures were approved by the Ethics Committee of Xiangya Hospital, Central South University, Changsha, Hunan Province, China. Patients gave their written informed consent along with their consent for surgery.
Surgical method
Each patient was placed in a 30° lateral decubitus position with their head down and hips elevated while under general endotracheal anesthesia. A small incision was made in the inferior umbilical fold. Pneumoperitoneum was achieved by carbon dioxide (CO2) insufflation through a Veress needle until the intraabdominal pressure reached 12–14 mmHg. A 30° laparoscope was inserted into the 10-mm infraumbilically placed port. Under direct visualization, a 10-mm port and a 5-mm port were then placed at the midpoints between the umbilicus, and the right and left anterior superior iliac spines to serve as surgical ports. An additional 5-mm assistant port was sometimes added at a point two-thirds of the distance from the umbilicus to the anterior superior iliac spine of the affected side (Fig. 1).

A 10-mm infraumbilical port was placed for laparoscope. A 10-mm port and a 5-mm port were placed at the midpoints between the umbilicus, and the right and left anterior superior iliac spines as surgical ports. An additional 5-mm assistant port was sometimes added at a point two-thirds of the distance from the umbilicus to the anterior superior iliac spine of the affected side.
The bladder was distended with 200–300 mL of saline through a urethral catheter. A transverse incision was made on the superior aspect of the bladder wall on the affected side using an electric hook, and the length of incision was kept to the minimum necessary to meet the demands of the intravesical procedure, normally about 4 to 5 cm. The bladder mucosa was circumferentially removed from around the ureteral orifice to a distance of 0.5 cm, and the intramural ureter was freed from the bladder wall using an electric hook. A clamp was then used to pull the ureter into the bladder, and the ureteral was dissected free of the bladder wall until 4 to 5 cm of terminal ureter was mobilized (Fig. 2). The ureter was then pulled as far into the bladder as possible, and the stenotic segment was resected.
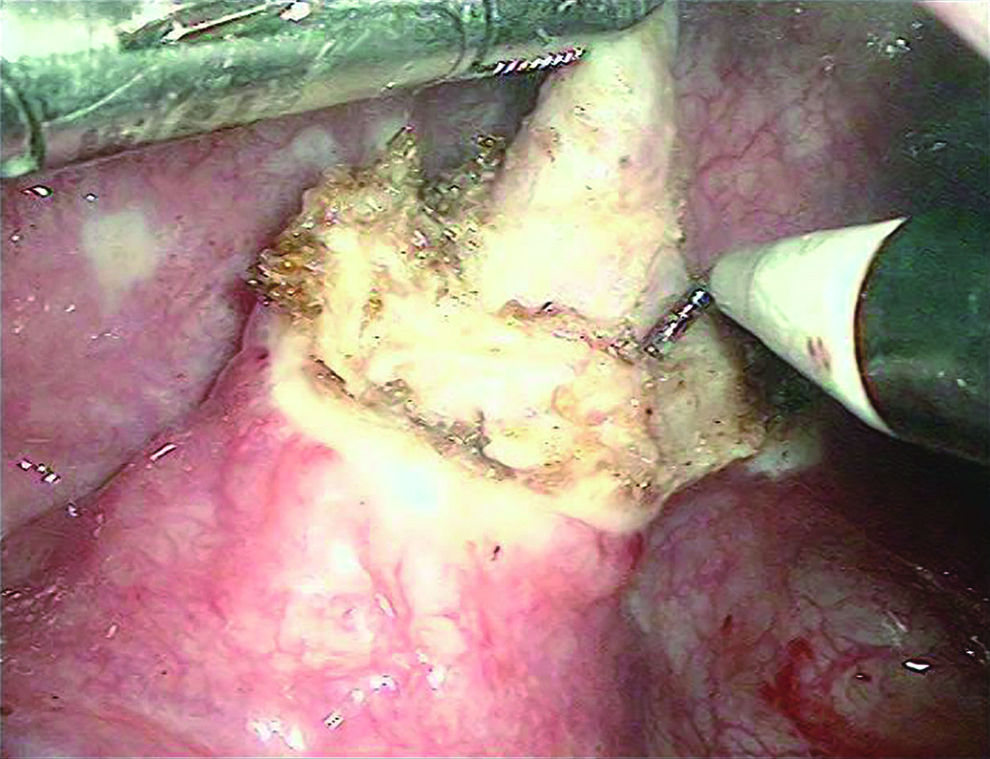
The ureter was dissected free of the bladder wall until 4 to 5 cm of terminal ureter was mobilized.
Four sutures were placed between the seromuscular layers of the bladder and the ureter, at 3, 6, 9, and 12 O'Clock, using 4–0 absorbable suture. The sutures were placed as proximally as possible on the ureter, with the aim of leaving 2 cm of mobilized ureter. Next, a longitudinal cut was made in the mobilized ureter using laparoscopic scissors (Fig. 3) and the terminal ureter was evaginated and sutured to the bladder wall with 4–0 absorbable suture to form a papilla (Fig. 4). The hiatus was reduced using 4–0 absorbable suture (Fig. 5) and a DJ stent was inserted into the ureter through a 5 mm surgical trocar and the bladder wall was closed with 3–0 absorbable suture.
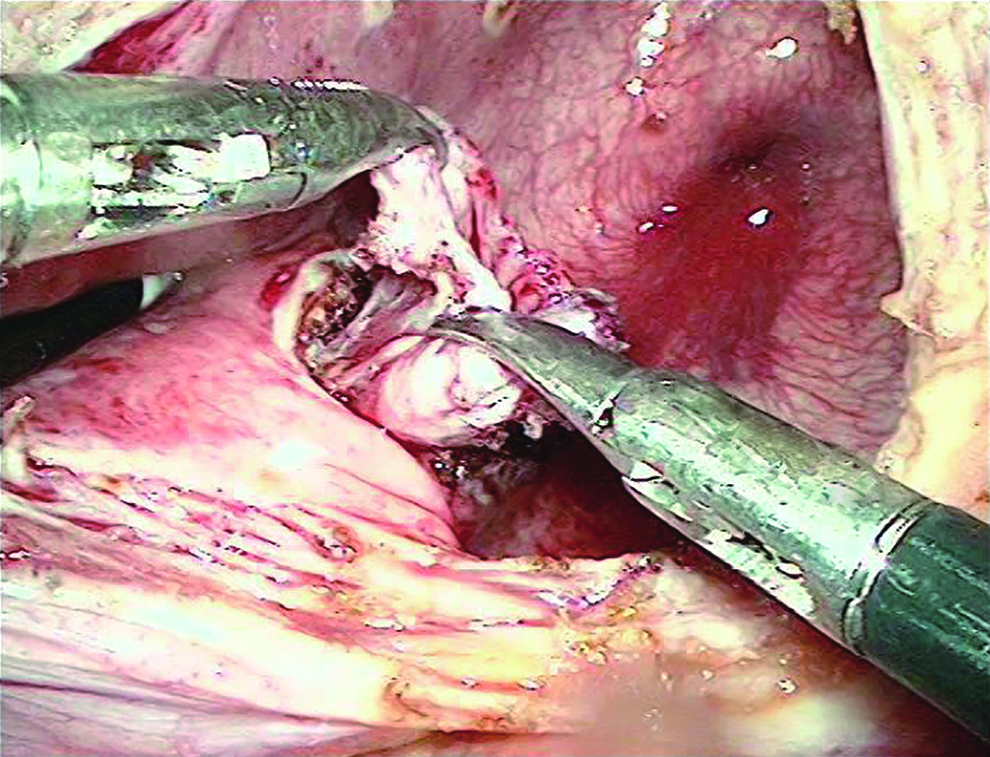
A longitudinal cut was made in the mobilized ureter using laparoscopic scissors.
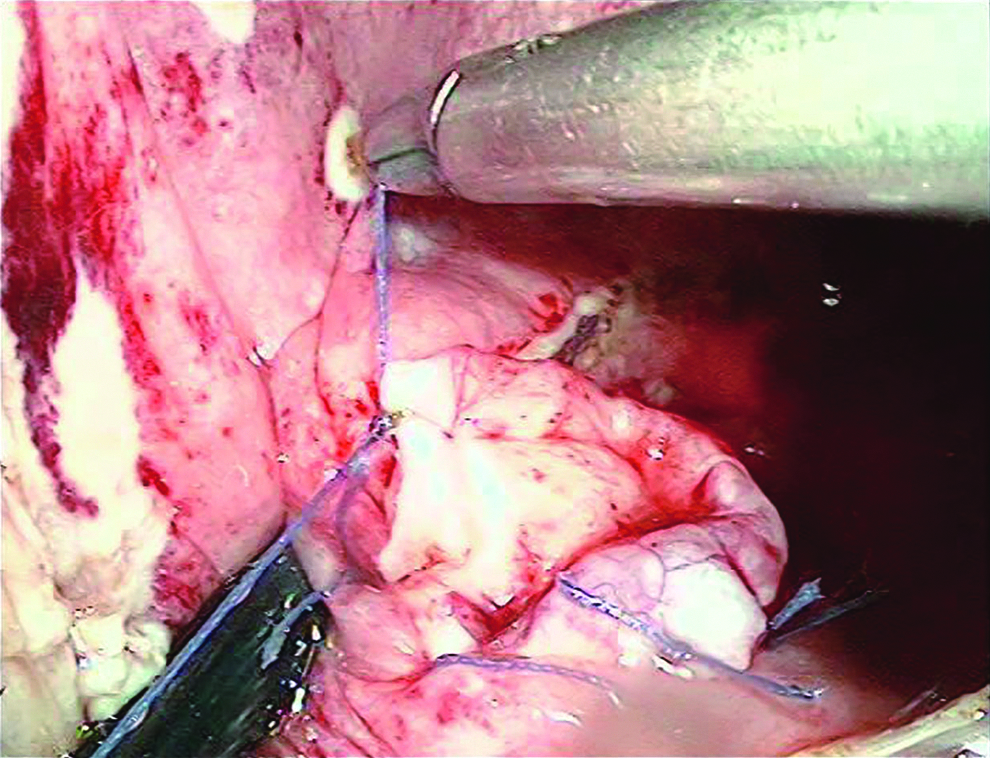
The terminal ureter was evaginated and sutured to the bladder wall with 4–0 absorbable suture, to form a papilla.
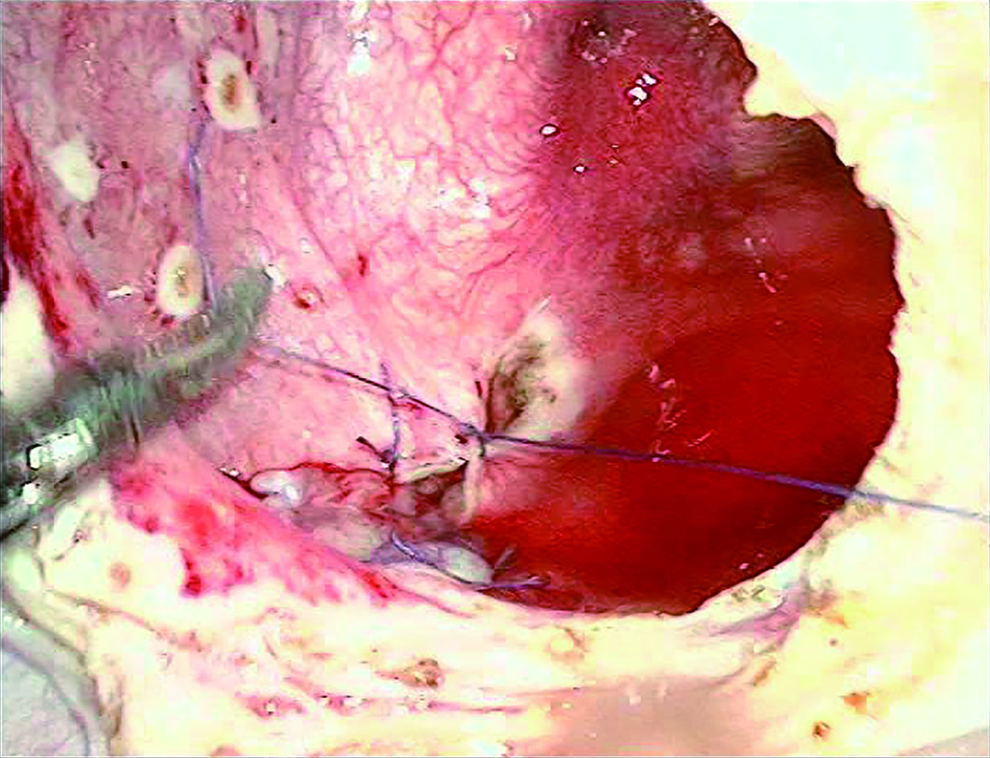
The hiatus was reduced using 4–0 absorbable suture.
In most cases, a drainage tube was placed with its end in the rectovesicular pouch (in male patients) or in Douglas' space (in female patients). The drain was removed when the drainage output was less than 10 mL in 24 hours. The Foley catheter was removed 7 days postoperatively, and the ureteral stent was removed 6–8 weeks after surgery. Patients who underwent nephrostomy before reimplantations had their nephrostomy tubes removed 2 weeks after surgery.
All patients underwent standard postoperative examinations, which at minimum consisted of IVP and B ultrasound performed at 3, 6, and 12 months after surgery, and VCUG performed at 3 or 6 months.
Results
All of the 16 operations were successful, and none required conversion to the extravesical approach or an open surgical procedure. Table 2 summarizes the intraoperative and postoperative results. The mean operating time was 98 minutes (range 85–135 minutes), and the estimated blood loss was 42 mL (range 30–60 mL). The mean hospital stay was 4.3 days (range 4–6 days).
Data in parentheses are percentages.
There were no obvious intraoperative or postoperative complications. The median follow-up period was 24 months (range 12–54 months). Follow-up VCUG showed no VUR of the operated ureter, and evaluation of B ultrasound and IVP (Figs. 6, 7) showed improvement of at least one hydronephrosis grade in 14 patients. In the remaining 2 patients, hydronephrosis improvement was evident but was not sufficient to change their grade (Table 2). There was no evidence of recurrence of the stenosis at the last follow-up examination in all patients.

Intravenous pyelography before reimplantation shows grade III hydronephrosis.

Intravenous pyelography 1 year after reimplantaion shows distinct resolution of hydronephrosis (from grade III to grade I).
Discussion
Terminal ureteral stenosis can be idiopathic or inflammatory, or may develop secondary to urolithiasis or other diseases. In most cases, iatrogenic injury due to abdominopelvic surgery or gynecological disease does not result in terminal ureteral stenosis, especially in the intramural segment of the ureter. Ureteral reimplantation is the standard treatment for distal or terminal ureteral stenosis.
In recent years, efforts have been made to adapt ureteral reimplantation techniques for minimally invasive surgery. Overall, the extravesical reimplantation technique described by Lich 1 and Gregoir 2 was the first to be successfully adapted to laparoscopic methods and has been commonly used for minimally invasive extravesical ureteral reimplantation. This technique effectively treats VUR and distal ureteral stenosis with overall success rates similar to those achieved with open reimplantation techniques.7–13 However, this technique also has drawbacks, which include disruption of pelvic structures and risk of transient voiding dysfunction, especially after bilateral ureteral reimplantation. 28
Extravesical reimplantation was the preferred minimally invasive method used to treat distal ureteral stenosis at our center before this study. From 2005 to 2015, 71 patients underwent laparoscopic extravesical ureteral reimplantation in our hospital; of these, restenosis was identified in 4 patients at 6–12 months follow-up. We believe that restenosis occurred due to excessive damage to the ureteral blood supply relative to the length of the stenosis. In the extravesical technique, the distal ureter is dissected anterograde, and excess dissection may be unwittingly performed if the stenotic portion of the ureter is located within the terminal segment.
In consideration of these concerns, we developed the laparoscopic intravesical ureteral reimplantation technique described here. Since July 2009 we have treated 16 patients with ureteral stenosis of the terminal segment using this technique and have achieved satisfying results without ureteral reflux or restenosis at 12–54 months follow-up.
Unlike the extravesical approach, this intravesical approach allows the ureteral orifice within the bladder to be accurately located and dissected without unnecessary injury to the surrounding connective tissues and blood supply of the ureter. In addition, this intravesical technique dissects the ureter free at the ureteral orifice and creates a new hiatus close to the original hiatus; this is very similar to anastomosis in situ and facilitates urine drainage while reducing the risk of angulation and twisting of the terminal ureter when the bladder is full. The anatomic placement of the surgically created ureteral hiatus also facilitates future ureteroscopy. In this study, all of the 16 pyeloureteral units had achieved resolution of dilation and there was no evidence of restenosis after at least 12 months follow-up.
Another advantage of this minimally invasive intravesical reimplantation technique is that the ureteral dissection method used does not disrupt the structures that cover the base of the bladder and support the pelvic organs and, hence, reduces the risk of potential injury to pelvic structures. Although there is no specific research to support this, it seems likely that less tissue disruption in the pelvic area may reduce the long-term risk of inflammatory adhesions within the pelvic cavity.
Since the development of the pneumovesicum technique, transvesicoscopy has been applied to allow transvesical reimplantation techniques. Compared with extravesical techniques, these newly developed transvesicoscopic techniques leave most of the pelvic structures intact; in addition, transvesicoscopic techniques allow reimplantation to be performed without an initial incision into the bladder wall. The creation of a submucosal tunnel for prevention of ureteral reflux is also possible using these techniques.
Yeung et al. 14 first described minimally invasive transvesicoscopic cross-trigonal ureteral reimplantation under CO2 pneumovesicum, with mean operating times of 112 and 178 minutes for unilateral and bilateral cases, respectively. Follow-up of 23 reimplanted ureters in 16 patients revealed complete resolution of VUR in 22 ureters in that case series. Transvesicoscopic ureteral reimplantation using the Politano–Leadbetter technique was first reported by Soh et al; of 19 ureters in 12 patients, reflux completely resolved in 18 ureters but persisted in one. 25 The median operating time using this technique was longer; 288 minutes for unilateral cases and 324 minutes for bilateral cases.
Single-site 20 and robot-assisted 16 laparoscopic transvesical ureteral reimplantation has also been performed in humans. Roslan reported a case in which a single-site transvesical technique was used for laparoendoscopic ureteral reimplantation. 20 The operating time was ∼250 minutes, and follow-up revealed no reflux or obstruction. Peters presented an approach to robot-assisted laparoscopic transvesical bilateral ureteral reimplantation, 1 boy out of 6 children had persistent low-grade reflux at follow-up and the operating time was not specifically mentioned.
Thus, it is evident that the mean operation times for transvesical techniques are significantly longer than for techniques that do not require pneumovesicum and concomitant cystoscopy. Nevertheless, these techniques are very useful for the treatment of patients with VUR, which are usually diagnosed and treated during infancy or childhood. Surgical methods for treating ureteral reflux are complicated, and a long operating time is expected in these cases; also, the bladder is smaller and at more risk of cicatricial contraction in children.
However, for adult patients with simple terminal ureteral stenosis without VUR that does not require tailoring, there seems to be no advantage of tranvesical versus extravesical surgical methods. The intravesical technique that we describe here has a mean operation time no longer than the extravesical techniques; thus, our newly described method can be adopted as a routine surgical technique with normal patient turnaround time.
It must be pointed out that terminal ureteral stenosis is the condition treated by the intravesical technique that we describe here, not VUR. In our experience, other than changing the location of the ureteral orifice and placing the ureter in a submucosal tunnel, intravesical direct nipple technique is adopted in our research to prevent reflux. Although VCUG showed no reflux at follow-up in our study, this technique only applies to terminal stenosis of the ureter without VUR, which may be its main limitation. In cases of VUR, more complicated techniques that allow tailoring of the ureter and formation of a submucosal tunnel for reflux prevention should be used. 29
Certain technical points are important. First, on the basis of our experience, the incision in the bladder wall should be ∼4 to 5 cm; a longer incision theoretically increases the chance of urine leakage or cicatricial contracture and also prolongs the suturing time and extends the duration of the surgery. Second, blunt dissection of the intramural portion of the ureter can be performed after placement of a 3F ureteral catheter if necessary. As much periureteral tissue should be left intact as possible when separating the ureter from the bladder wall to preserve blood supply. Third, sutures in the terminal ureter should be placed longitudinally to avoid ischemia and annular stricture.
DJ stents were routinely placed and removed 6–8 weeks after surgery. For the patients who had percutaneous nephrostomy tubes, a DJ stent was still placed in the operated ureter to allow better drainage and prevent anastomotic stricture during the early stages of healing, and their nephrostomy tubes were removed 2 weeks after the ureteral reimplantation surgery.
The surgical field with this intravesical technique is limited, which may complicate dealing with unexpected bleeding; this is also a problem with transvesicoscopic techniques. In some rare cases, changing the surgical approach (e.g., to an extravesical reimplantation) might be necessary to stop bleeding. In such a case, the intravesical technique may be more easily switched to an extravesical approach than the transvesicoscopic techniques.
Conclusions
The intravesical ureteral reimplantation technique that we report here is safe and feasible. It may be an alternative method for treatment of terminal ureteral stenosis without VUR when the distance between the most proximal part of the stenosis and the ureteral orifice is <2.5 cm. However, this technique should be further refined; more patients, especially those with bilateral ureteral stenosis, are needed to reliably evaluate its efficacy and safety.
Footnotes
Acknowledgments
This study was financially supported by 2015 Subsidy Funds for Industrial R&D Project by the Development and Reform Commission of Hunan Province.
Disclosure Statement
No competing financial interests exist.