
Abstract
Abstract
Background:
The aim of this prospective trial was to evaluate the clinical outcomes of nonabsorbable polymeric clips in laparoscopic appendix stump closure in children by comparing the endoloop ligature.
Patients and Methods:
From June 2011 to June 2016, 277 children who underwent laparoscopic appendectomy were included in the study. The patients were divided into two groups based on the technique used for appendiceal stump closure: there were 101 patients in the polymeric clips group and 176 in the endoloop group. The risk of intraoperative and postoperative complications was investigated for two different techniques to close the appendiceal stump.
Results:
Among the 277 patients who underwent laparoscopic appendectomy, no intraoperative complications and 17 (6.1%) postoperative complications were recorded. There were no significant differences between the groups with respect to the postoperative complications (P = .546). The median length of the operation was 10 minutes shorter when the polymeric clips were used (P < .001). The median hospital stay was also shorter in the polymeric clips group (P = .008). Costs of polymeric clip were significantly lower (€ 17.64) compared to endoloop (€ 34.16).
Conclusions:
Closure of the appendix stump with polymeric nonabsorbable clips in laparoscopic appendectomy reduces operative time and may be a cost-effective and simpler alternative to widely used endoloops.
Introduction
L
Materials and Methods
Patients
From total number of 281 patients who underwent laparoscopic appendectomy because of suspected appendicitis, between June 2011 and June 2016, in the Department of Pediatric Surgery, Split University Hospital, 277 patients (147 males and 130 females) were enrolled in the study. The study was carried out as a cross-sectional single-center trial. Informed consent was obtained from the parents of all of the patients and the Ethics Committee of Split University Hospital approved the study protocol.
All patients with suspected appendicitis younger than 18 years of age were enrolled in the study. The exclusion criteria were patients older than 17 years of age, the patients converted to open appendectomy, pregnant patients, the patients who needed stapler application for stump closure, and patients who refused laparoscopic appendectomy.
The technique used for closure of the appendiceal stump (endoloop or polymeric clips) was chosen based on the operating surgeon's personal preference. The data were grouped according to the stump closure technique; a polymeric clips group (101 patients; 36.5%) and an endoloop group (176 patients; 63.5%).
In each group, the patients were divided in three subgroups based on the intraoperative and histopathological findings (acute appendicitis, perforated appendicitis and other/no pathology). Preoperatively, all patients underwent a clinical examination and laboratory analysis. In most of the patients, abdominal ultrasonography was performed. The patient data are summarized in Table 1.
Mann–Whitney U test.
Chi-square test.
BMI, body mass index; IQR, interquartile range.
Hypothesis and outcome measures
The primary endpoint of this study was to test the hypothesis that there would be an equal frequency of postoperative complications in patients in whom the appendiceal stump was secured using polymeric clips compared to the patients in whom an endoscopic loop was used for securing the appendiceal stump in laparoscopic appendectomy. The primary outcome measure was the rate of intra-abdominal surgical site infections, defined as a postoperative intra-abdominal abscess and peritonitis. The secondary outcome variables were the intraoperative and postoperative complications, duration of operation and hospital stay, and the rate of reoperations. The intraoperative complications included access-related complications, such as organ lesions, thermal damage of intra-abdominal organs, and intraperitoneal bleeding. Postoperative complications included bleeding into the abdominal wall, wound infection, postoperative ileus, small bowel obstruction, and formation of an intra-abdominal abscess.
Operative technique
The patient was placed in a supine position, combined with the Trendelenburg position and left lateral position. The surgical procedure was performed under general anesthesia. A Veress needle was introduced below the umbilicus and CO2 insufflated at a pressure of 8–12 mmHg depending on patient's age and body weight. Laparoscopic appendectomy was performed using a three-trocar technique with a combination of 5- and 10-mm trocars. The mesoappendix was dissected, depending on the surgeons' preferences, with a harmonic scalpel (Ultracision™; Ethicon Endo-surgery, Cincinnati, OH), a bipolar tissue sealing system (Ligasure™; Valleylab, Boulder, CO), or using thermal fusion technology (MiSeal™; Microline, Beverly, MA).
Appendiceal base was secured using an endoloop (Vycril Endoloop-0; Ethicon Endo-surgery) or polymeric clips (Ligating Clips XL; Grena, Brentford, United Kingdom). When a loop was used, it was placed at the base of the appendix, and the appendix was divided 5 mm above the loop with the device used for dissecting the mesoappendix. When polymeric clips were used, two polymeric clips were placed at the base of the appendix, and the appendix was divided 5 mm above the clips with the device used for dissecting the mesoappendix. In all cases, a 5-mm scope was used through the supraumbilical trocar. Each specimen was retrieved inside a disposable specimen retrieval bag (Ecosac EMP 70; Espiner Medical Ltd.) through the largest trocar.
Follow-up
The patients were followed up at our outpatient clinics at the first and fourth weeks after surgery for detection of any complications. Skin sutures were removed in the first week visit.
Statistical analysis
The data were analyzed using the Microsoft Excel for Windows Version 11.0 (Microsoft Corporation) and SPSS 19.0 (IBM Corp, Armonk, NY) software programs. Distributions of quantitative data were described by means and standard deviations, or medians and ranges, whereas absolute rates and percentages were used to describe categorical data. Differences in median values of quantitative variables between the groups of patients were tested with t-test for independent samples or Mann–Whitney U test, depending on distribution of the data. The chi-square test or Fisher's exact test was used for the statistical analysis of the categorical data, depending on the distribution of data. All values of P < .05 were considered to indicate statistical significance.
Results
Two hundred seventy-seven consecutive patients were identified for the analysis. Polymeric clips were used in 36.5% (n = 101) and endoloop ligatures in 63.5% (n = 177). Distribution of devices used for securing of the appendiceal stump during the study period (2011–2016), is shown in Figure 1. An analysis of the patient data showed that there was a significant difference between the groups only with respect to sex and body mass index (BMI). There were 62% males in the polymeric clips group and 48% in the endoloop group (P = .019). The median BMI in the polymeric clips group was 19 kg/m2 (interquartile range [IQR] 17, 21) and 20 kg/m2 (IQR 19, 23) in the endoloop group (P = .003). There were no significant differences between the two groups regarding age, preoperative laboratory values (white blood cell count, C-reactive protein level, neutrophil count), or clinical data (duration of symptoms, nausea, vomiting, body temperature, local clinical findings) (Table 1).
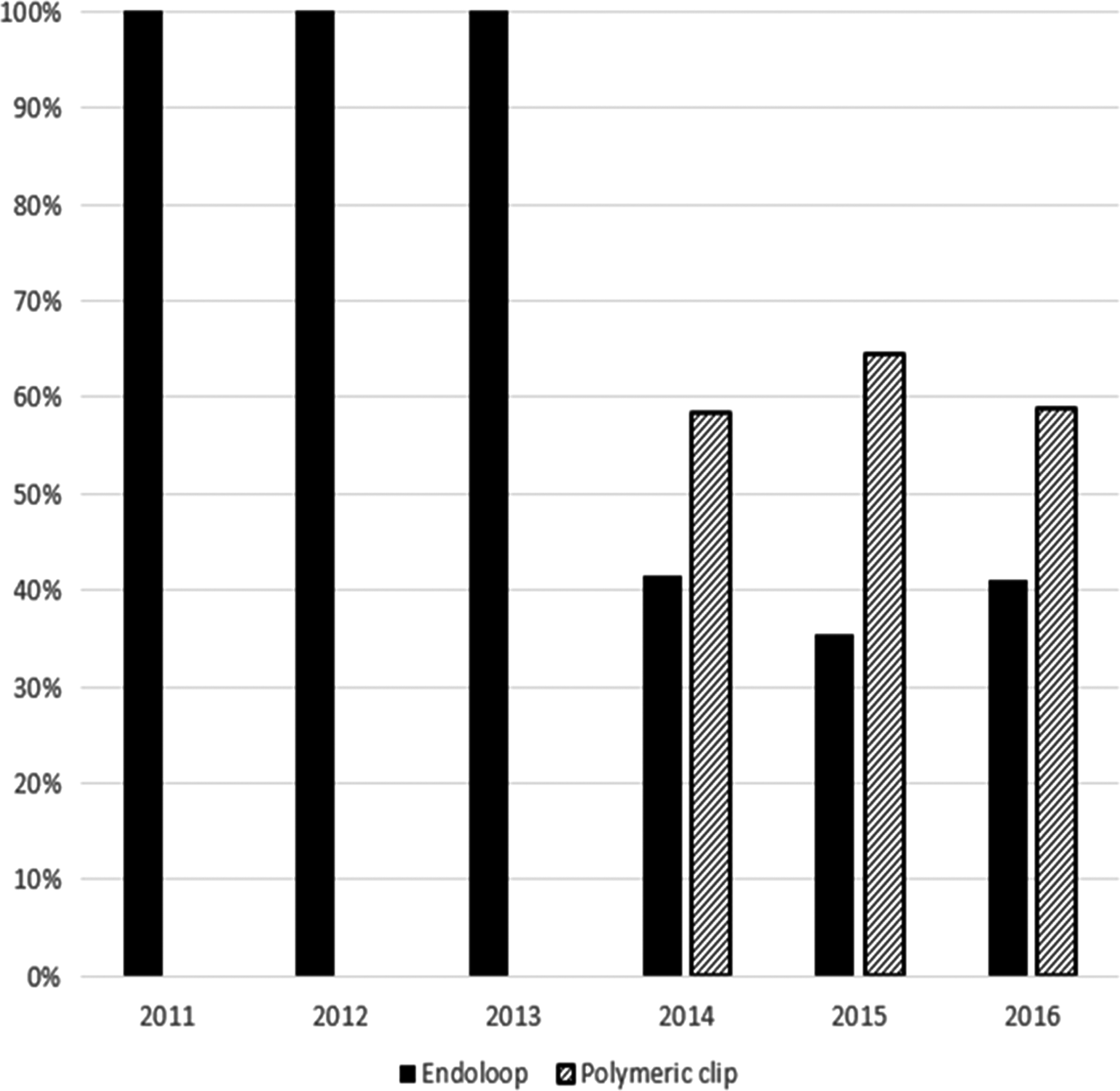
Annual distribution of applied devices for laparoscopic appendectomy.
The median duration of surgery was 25 (IQR 21, 36) minutes when polymeric clips were used compared with 35 (IQR 25, 50) minutes when endoloops were used (P < .001) (Table 1, Fig. 2). The median hospital stay was 3 (IQR 2, 4) days for the polymeric clips group and 3 (IQR 3, 4) days for the endoloop group (P = .008) (Table 1, Fig. 3). A total number of 4 patients required reoperation, 2 patients in the polymeric clips group and 2 patients in the loop group (P = .358) (Table 1). A histopathological analysis revealed a positive diagnosis of appendicitis in 250 patients (90.2%).
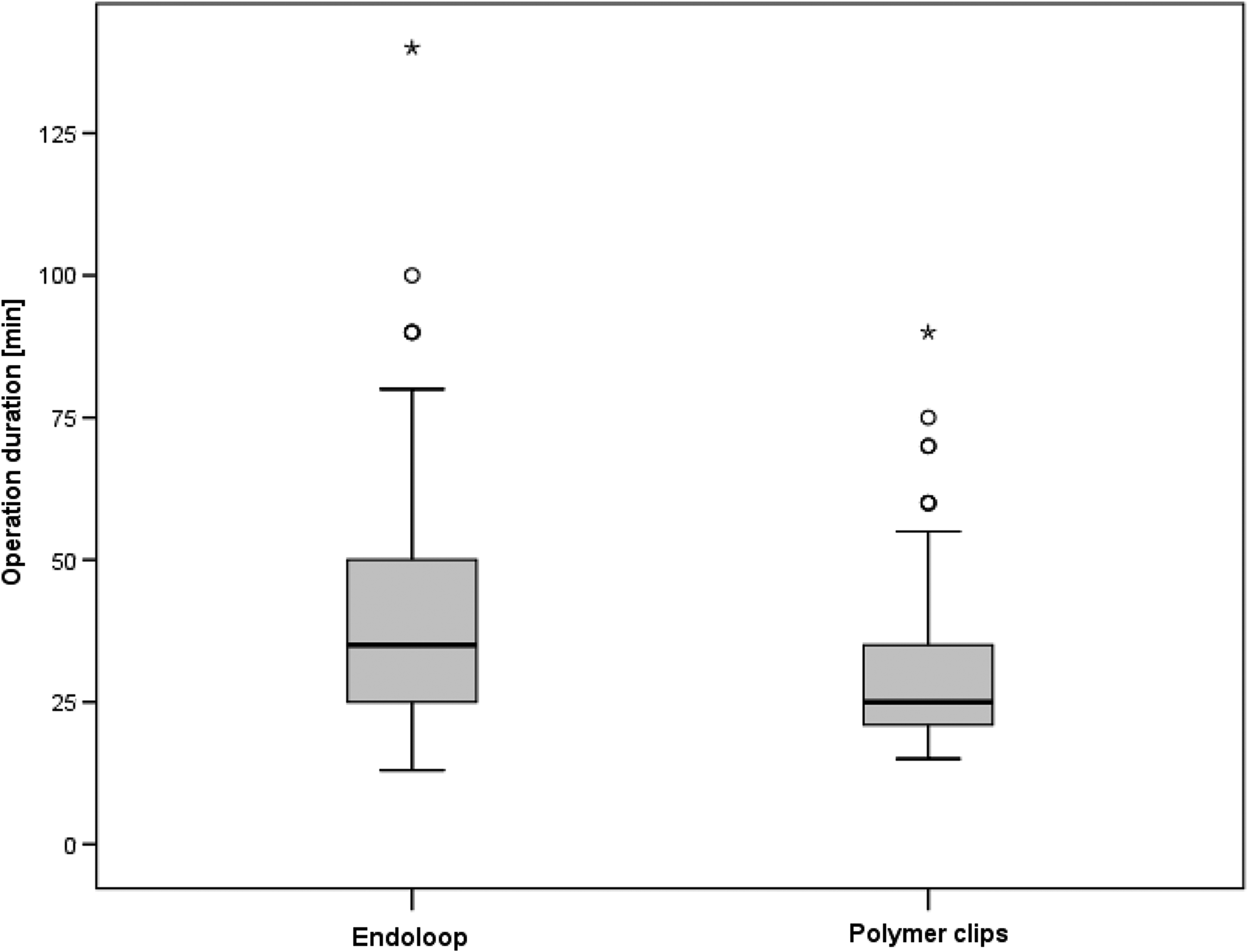
Box plot of operation duration depending on the applied technique (P < .001). Asterisk represents highest value.
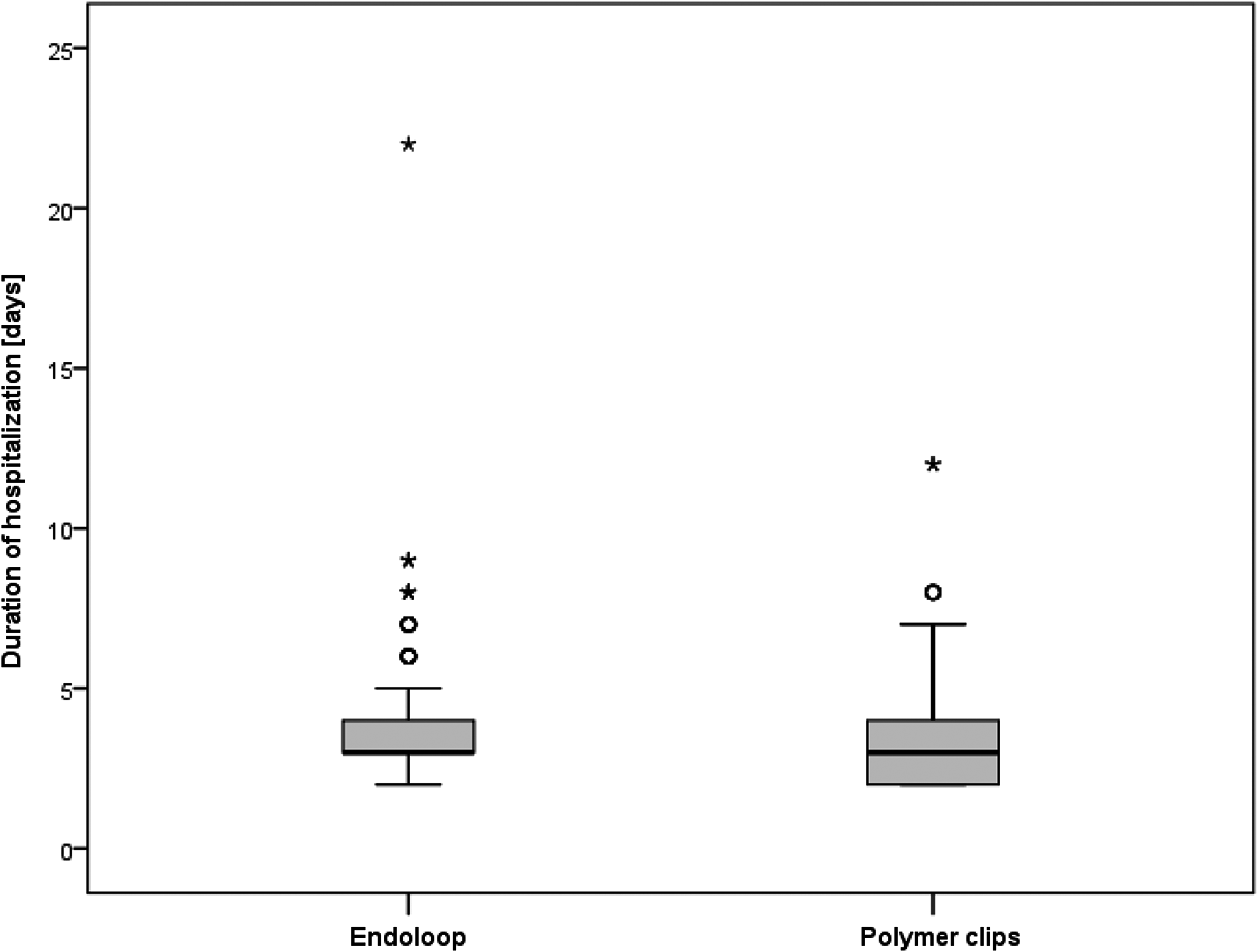
Box plot of hospital stay depending on the applied technique (P = .008). Asterisk represents highest value.
There were 13 patients (4.7%) with an innocent appendix and 14 patients (5.1%) with other pathology (Table 2). Among the 277 patients included in the study, there were no cases of intraoperative complications. There were 17 (6.1%) postoperative complications. There were 5 (1.8%) wound infections (3 in the polymeric clips group, 2 in the loop group), 5 (1.8%) intra-abdominal abscesses (2 in the polymeric clips group, 3 in the loop group), 6 patients with fever lasting >3 days (2.2%) (2 in the polymeric clips group, 4 in the loop group), and 1 (0.3%) case of trocar site bleeding (in the polymeric clips group). There were no significant differences between the groups regarding the postoperative complications (Table 3). The procedures used for treating the complications are shown in Table 4.
Fisher's exact test.
Fisher's exact test.
Discussion
In many countries, laparoscopic appendectomy has become the standard surgical approach to treat acute appendicitis.3–5 Less pain, lower rates of intra-abdominal adhesions and wound infection, and shorter hospital stay, due to reduced surgical trauma, are advantages of a laparoscopic procedure over an open approach.1–3,5,13 Despite the lack of a clear outcome benefit of laparoscopic appendectomy, most cost studies have confirmed a substantially higher cost of laparoscopic appendectomy compared with open appendectomy, due to expensive disposable equipment used during the procedure.5,11,14,15 However, the safest endoscopic technique to close the appendiceal stump remains debateable.2,5,10–12 Different techniques can be used in the laparoscopic closure of the appendix stump, but the superiority of any of these techniques could not be demonstrated so far. The closure of the appendiceal stump is a very important step during a laparoscopic appendectomy, because most of the postoperative complications are caused by its inappropriate management.5,12 Most surgeons prefer either endostaplers or endoloops to close the appendiceal stump.
Linear staplers are more expensive than loops, require a 12-mm port for their introduction, and leave metal staples on the stump that can cause adhesion-related short bowel obstruction.16,17 Endoloops are associated with more manipulation of the stump and can potentially slip, which can cause intra-abdominal abscess formation. Endoloops are not safe for closure of the cecum when the base of the appendix is perforated or if the inflammation of the appendix has also involved the cecum.5,16
Many studies showed that there is no evidence for routine stapling to secure the appendiceal stump. The appendiceal stump can be secured safely with the use of endoloops or clips in majority of patients, and a selective use of a stapler should be considered in a small minority of patients. Use of staplers significantly increases the cost and duration of an operation. Because of that, surgeons should be selective to use a stapler only in specific cases where it is indicated.2,5,10,11 The alternatives to endoloops or endostaplers are intracorporeal suturing, extracorporeal sliding knot, or titanium clips, but none of it gained broad acceptance for the closure of appendix stump.5,11
Recently, nonabsorbable polymeric clips were introduced as a useful alternative for ligation of the appendicular base.2,12,15 Several studies have described the use of polymeric nonabsorbable clips as a safe, feasible, and cost-effective method.2,12,15 In these studies, one or two clips were placed on the appendiceal stump. The largest recommended diameter of the appendicular stump that can be safely closed with this clip is 10 mm. 15
In this prospective study, safety and feasibility of nonabsorbable polymeric clips were evaluated in laparoscopic appendiceal stump closure by comparing it with a widely used endoloop ligature.
In our study, no significant differences were found between endoloop and polymeric clips group regarding postoperative complications. Similar findings were observed in other published studies.12,15,18,19 Soll et al. reported that closure of the appendiceal stump using the nonabsorbable polymeric clips reduced the rate of intra-abdominal surgical abscesses compared to the application of endoloops. 2 Our data showed shorter time of operation, and lower cost in the polymeric clips group was found. Similar findings were reported in other studies.2,18,19 Colak et al. did not find a significant difference between groups regarding the time of operation. 12 In this study, shorter hospital stay was also found in the polymeric clips group. We believe that shorter hospital stay in polymeric clips group was an incidental finding because this was not observed in similar studies.2,12,15,18,19
Many studies pointed an advantage of nonabsorbable polymeric clips in lower cost than other products that are generally used for closure of appendiceal stump.2,12,15,18,19 In our country, the additional charges of polymeric clips, endoloop ligatures, and endoscopic staplers are € 17.64, € 34.16, and € 378.5 for each appendectomy procedure, respectively.
No intraoperative complications were recorded in this study. In similar studies, the most common reported intraoperative complication was thermal injury of surrounding tissues, but this complication do not depend on appendiceal stump closure technique.5,10,11,20–22
In this study, nonabsorbable polymeric clips and absorbable endoloops made of polyglactin were compared. It remains highly questionable whether this difference significantly affects an outcome. In addition, potential defects in the various closing mechanisms need to be considered a cause for leakage of the appendiceal stump and the development of abdominal abscesses. Since polymeric clips close systematically by a visible clicking mechanism at the end of the snap, the pressure of the closed endoloop on the tissue depends on the force used by the individual surgeon to lock the thread in place outside the abdominal cavity. Therefore, the knot of the endoloop system has a potentially higher risk of slipping due to insufficient closure or in contrast, a transection or necrosis of the tissue as the result of a knot that is too tight. 2
Another potential risk factor for the development of intra-abdominal abscesses might be protuberant mucosa of the appendiceal stump, distal of the closing devise. This negative aspect has already been described for the endoloop system. 2 Although results are significant and this study was prospective, the limitation refers to the design of the study since patients were not randomized.
Conclusions
Although it is not possible to make general conclusions, on basis of our findings, closure of the appendix stump with endoloop or polymeric nonabsorbable clips in laparoscopic appendectomy in children is safe and effective without difference in complications rate. The use of polymeric clips has an advantage in shorter operative time and lower costs compared to other widely used methods.
Footnotes
Disclosure Statement
No competing financial interests exist.