
Abstract
Abstract
Introduction:
The aim of this study was to compare the effectiveness and safety of endoscopic injection sclerotherapy (EIS) with endoscopic variceal ligation (EVL) in the management of esophageal variceal bleeding (EVB).
Patients and Methods:
In this prospective study, we compared the EIS and EVL in 124 patients who had endoscopically proved bleeding from esophageal varices. According to different treatment methods, they were randomly divided into the EIS and the EVL groups. Sixty-four patients were treated with sclerotherapy and 60 with ligation. The patients were followed for a mean of 2 years, during which we determined the incidence of complications and recurrences of bleeding and the number of treatment sessions needed to eradicate varices, mortality, and survival.
Results:
Active bleeding at the first treatment was controlled by EIS in 19 of 19 patients and by EVL in 16 of 16 patients. The likelihood of early rebleeding was slightly smaller in the patients treated with EIS (7.8% versus 11.7%, P = .47). However, late rebleeding rate was slightly more in EIS patients (28.1% versus 23.3%, P = .54) without statistical significance. The rate of eradication of varices in the EIS group was slightly lower than in the EVL group (79.7% versus 86.7%, P = .30). There were also no statistically significant differences in mortality (1.6% versus 3.3%, P = .61) or survival rate (71.9% versus 78.3%, P = .41) (all P > .05) after EIS and EVL. However, fever in the EIS group was significantly higher compared to that of in the EVL group (n = 17, 26.6% versus n = 6, 10.0%, P = .02).
Conclusions:
Both EIS and EVL produce excellent results, are safe, effective, feasible, and acceptable for EVB with minimum complications and obviate need for subsequent procedures in the short term. To make better choice, we should consider the hospital conditions, operator experience, and the characteristics of esophageal varices.
Introduction
E
Various techniques such as Balloon tamponade, vasoconstrictor, and surgical intervention have been applied, but these measures did not reduce the risk of rebleeding, complications, and improvement in survival in EVB. The advantage of TIPS is offset by a risk of developing hepatic encephalopathy, the most relevant postprocedural complication. 9 Currently, two endoscopic techniques are being used to treat bleeding esophageal varices; endoscopic injection sclerotherapy (EIS) and endoscopic variceal ligation (EVL).10–12 It is widely accepted that both EIS and EVL are effective in the control of acute variceal bleeding, decrease the rate of rebleeding, and prolong the survival time. 13 EIS of esophageal varices is designed to control the initial bleed and prevent subsequent bleeding by thrombosing the veins or thickening the mucosa overlying the veins in this area. EIS can be accomplished by either intravariceal EIS or extravariceal EIS.10,14 Several technical variables may affect the outcome of any individual sclerotherapy session or clinical trial. 15 Important factors influencing the complication rate are the experience of the endoscopist, the specific injection technique used, the use of ancillary devices, including overtubes or balloon tamponade, and whether sclerotherapy is performed as an emergency or elective procedure. 16 Other interrelated anatomical factors are the close proximity of the esophagus to vital mediastinal structures, repetitive breaching of the mucosa, and the potential for pulmonary and systemic spread of sclerosant through portal venous collaterals.16–18
EVL was developed as an alternative endoscopic method of treating esophageal varices with the anticipation that EVL would be as effective as EIS, but with fewer complications. 19 A practical limitation of EVL is the suction cap on the tip of the endoscope, which reduces the field of vision by 30% and is a disadvantage when treating actively bleeding varices as blood and clot may pool in the suction cap and further reduce visibility. The new transparent caps have improved visibility. EVL performed every 2 months (bimonthly) showed better results than EVL once every 2 weeks (biweekly) in patients with esophageal varices. 20 Treatment sessions separated by a longer interval had a higher rate of total eradication and lower rates of recurrence and additional treatment. 12 Some reports showed that EVL plus pharmacological therapy was effective for the prevention of recurrent variceal hemorrhage. 21 Some scholars believe that EIS should be replaced by EVL because EIS is associated with more complications, while others insist that EIS is still the most effective way to control acute EVB and should not be abandoned. EIS has had a high success rate in controlling bleeding varices and has become established as the recommended treatment modality in the management of EVB. In contrast, the EIS technique differs among operators, leading to nonuniformity of results. The combination of EVL and small-volume EIS has the potential advantage of augmenting the benefits of both techniques by achieving more rapid variceal eradication and less chance of variceal recurrence, thus reducing the likelihood of later rebleeding. 22
This study compares the safety and efficiency of EVL and EIS treatment modalities for the management of EVB.
Patients and Methods
Patients and data collection
The characteristics of the patients included in this prospective study are summarized in Table 1. Between January 2010 and June 2012, a total of 124 patients with endoscopically proved EVB were enrolled at Shandong Provincial Hospital Affiliated to Shandong University. All the patients were diagnosed by esophagogastroduodenoscopy and were randomly assigned to undergo EIS or EVL according to a computer-generated randomization sequence. All the patients met the following criteria: (a) no history of previous endoscopic or surgical treatment for varices; (b) absence of hepatocellular carcinoma or other malignant tumors; and (c) written informed consent was obtained. Diagnosis of cirrhosis was confirmed by liver biopsy or by a combination of clinical and biochemical findings. Etiology of cirrhosis is shown in Table 2.
EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation; PBC, primary biliary cirrhosis.
Ethics statement
This study was approved by the Ethics Committee of Shandong Provincial Hospital Affiliated to Shandong University. All patients, or their legal representatives, signed informed consent forms.
Materials
Endoscopes (GIF—XQ260) and needle injectors (NM-200L-0421 Olympus) were used in the procedure. Lauromacrogol injection (Tianyu Pharmaceutical Company, shaanxi-China) was used as a sclerosing agent. The Six-Shooter Multi-band Kit (MBL-6, Cook, Inc., Winston-Salem) was chosen for EVL.
Methods
Before EVS or EVL, all patients included in this study were treated with octreotide or somatostatin, proton pump inhibitors. Blood volume resuscitation was done in case of massive bleeding with the goal to maintain the hemodynamic stability (BP >90/60 mmHg). Diazepam (10 mg), raceanisodamine (10 mg), and pethidine (50 mg) were administered intravenously as premedication just before therapy.
In the EVL group, whenever the exact rupture point was not identified, application of the bands was started from the cardiac part of the stomach and progressed upward in a helical way for ∼5 cm. Six to eighteen bands were placed depending on the number and size of the varices. Procedure was repeated monthly until the varices were eradicated (Fig. 1A–D).

Endoscopic photograph shows esophageal varices.
In EIS group, sclerosing agent was injected both intravariceal and paravariceal. According to the grade of varices, whether there was red-color sign and the perforating veins, sclerosing agent would be injected into the tela submucosa 5 cm above the cardiac beside the varices by 20–35 points. When intravariceal injection was performed, 3–10 mL sclerosing agent was injected into each lumen of varices by one or two points. However, the maximum volume used for intravariceal injection was 30 and 50 mL per session. Procedure was repeated monthly until the varices were eradicated (Fig. 1E–H).
Follow-up
After endoscopic treatment, patients were followed up until 2 years through bedside appointments or telephone contact. Esophagogastroduodenoscopy was performed every 3 months in the first year and every 6 months thereafter. Varices were treated as previously if they recurred.
Definitions
To evaluate the efficacy of both treatment modalities, they were compared regarding failure in bleeding control (up to 5 days), early recurrence of bleeding (5 days and 6 weeks), late recurrence of bleeding (after 6 weeks), and complications and survival rate at the end of the follow-up. Failure in bleeding control was defined as the failure to control bleeding at the moment of examination or the occurrence of rebleeding or mortality within the first 5 days after the procedure. Failure was defined as death or the need to change therapy, including the following criteria: (a) fresh hematemesis or NG aspiration of P100 mL of fresh blood P2 h after the start of a specific drug treatment or therapeutic endoscopy, (b) development of hypovolemic shock, and (c) 3 g drop in Hb (9% drop of Ht) within any 24 h period if no transfusion was administered. Recurrent hemorrhage was proven by upper gastrointestinal endoscopy.
Statistical analysis
SPSS 17.0 program was used to analyze the result. A student's t-test was used for the comparison of mean with normal distribution variables. χ2 test or Fisher's exact test was used to compare the frequencies observed in variables across the EIS and EVL groups. The level of significance was P < .05.
Results
Patient's characteristics and clinical outcomes in EIS and EVL groups
All patients presented with hematemesis and melena and were confirmed having esophageal varices by endoscopy. One hundred and twenty-four patients participated in this study, 64 in the EIS group and 60 in the EVL group. There was a male predominance in gender (96 males, 77.4%). Active bleeding was observed in (n = 35, 28.2%) cases. Number of patients according to Child Pugh classification were as follows, Child Pugh A Class (n = 44, 35.5%), Child Pugh B Class (n = 62, 50%), and Child Pugh C Class (n = 20, 16.1%). The grade of varices was mostly G2 (n = 19, 15.3%) and G3 (n = 105, 84.7%).
In EIS group, the number of sessions received by each patient was 1–6 (mean: 3.1). A mean of 37.6 mL Lauromacrogol injection was used by 20–40 (mean 27.4) points in the first session. In EVL group, the number of sessions received by each patient was 1–5 (mean: 2.7). At average, 13.7 bands were applied in each patient during the first session. For most of the patients, the interval between first two sessions was about 1 month. Only small number of patients received single endoscopy session due to following reasons: (1) no recurrent hemorrhage; (2) poor compliance due to heavy economic burden; and (3) high risk of suffocation in patients with massive hemorrhage under general anesthesia. Most of the patients underwent EIS or EVL without anesthesia due to the reason that they cannot tolerate it. The analysis included 64 patients in the EIS group and 60 patients in the EVL group. Baseline clinical characteristics were not significantly different between the two groups (Table 1).
Etiology of cirrhosis in EIS and EVL groups
Chronic hepatitis B still remains the main cause of cirrhosis in China. The etiology of cirrhosis in the EIS group compared with EVL was viral hepatitis B (n = 34, 53.1% versus n = 38, 63.3%, P = .25), viral hepatitis C (n = 3, 4.7% versus n = 1, 1.7%, P = .62), viral HBV+HCV (n = 1, 1.6% versus n = 2, 2.3%, P = .61), alcoholic liver disease (n = 4, 6.2% versus n = 3, 5.0%, P = 1.00), primary biliary cirrhosis (n = 3, 4.7% versus n = 0, 0.00%, P = .25), and cryptogenic (n = 19, 29.7% versus n = 16, 26.7%, P = .71) (Table 2).
Treatment modality and its clinical effects
The rate of successful control of active bleeding was achieved in 100% (19/19 patients) in the EIS group and 100% (16/16 patients) in the EVL group. The early rebleeding rate in EIS group was slightly lower than that in the EVL group (7.8% versus 11.7%, P = .47). The late rebleeding rate in EIS group was slightly higher than that in the EVL group (28.1% versus 23.3%, P = .54). The variceal eradication rate in the EIS group was also slightly lower than that in the EVL group (79.7% versus 86.7%, P = .30) Table 3. These results were not statistically significant.
EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
Complications of the EIS and EVL groups
Possible complication of endoscopic treatment was observed in both the groups. Retrosternal pain or discomfort in the EIS group was higher compared with EVL group (n = 40, 62.5% versus n = 31, 51.7%, P = .22) without statistical significance. However, fever in the EIS group was significantly higher compared to that of in the EVL group (n = 17, 26.6% versus n = 6, 10.0%, P = .02). Milder complications such as nausea and vomiting were slightly higher in EIS group compared with EVL group (n = 10, 15.6% versus n = 8, 13.3%, P = .72), but without statistical significance; mild decrease in ascites was observed in EIS group than EVL group (n = 6, 9.4% versus n = 7, 11.6%, P = .68). In the EIS group, esophageal stricture was slightly higher compared with EVL group (n = 3, 4.7% versus n = 2, 3.3%, P = 1.00) without significance Table 4. Except fever, no significant differences were found between the EIS and EVL groups. Other complications such as esophageal perforations and ARDS were not observed.
Value in bold represents fever in the EIS group was statistically significant as compared to that of in the EVL group (n = 17, 26.6% versus n = 6, 10.0%, P = .02). P < 0.05 were considered statistically significant in our study.
EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
Survival time
There was no statistically significant difference in postoperative death in the EIS and EVL groups (1.6% versus 3.3%, P = .61) and the 2-year survival rates (71.9% versus 78.3%, P = .41) in the EIS and EVL groups Table 5. In the EIS group, one patient died 5 h postoperatively; there was no evidence of rebleeding found by endoscopy and no positive finding on brain CT. Patient's family refused to undertake the postmortem. We suspected the brain stem infarction as the cause of death according to clinical manifestation. A large dose of sclerosing agent might be the initiating factor. Seventeen patients died during the following 2 years. In the EVL group, 2 patients died due to massive hemorrhage caused by early band detachment at days 5 and 10 after EVL. Eleven patients died during the following 2-year follow-up. Three main causes of death in the two groups and survival curve are shown in Figures 2 and 3.
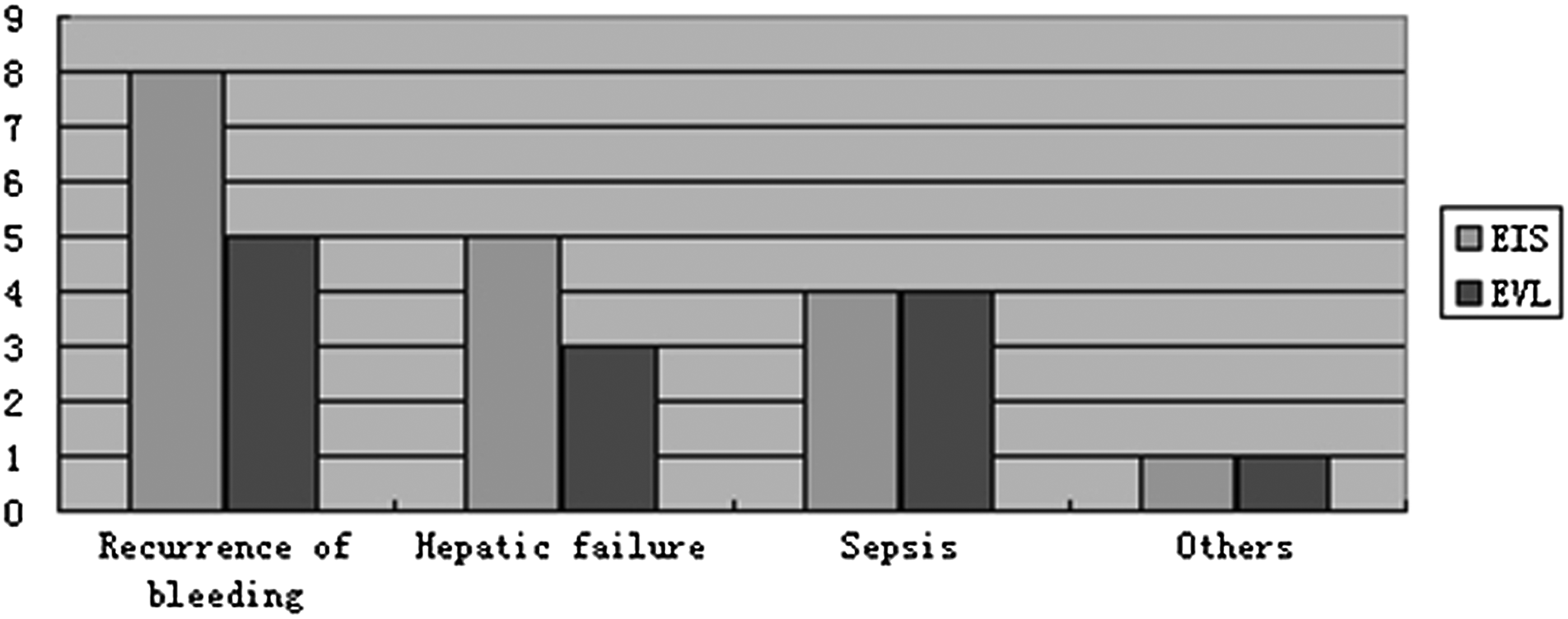
The causes of death in EIS and EVL. EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
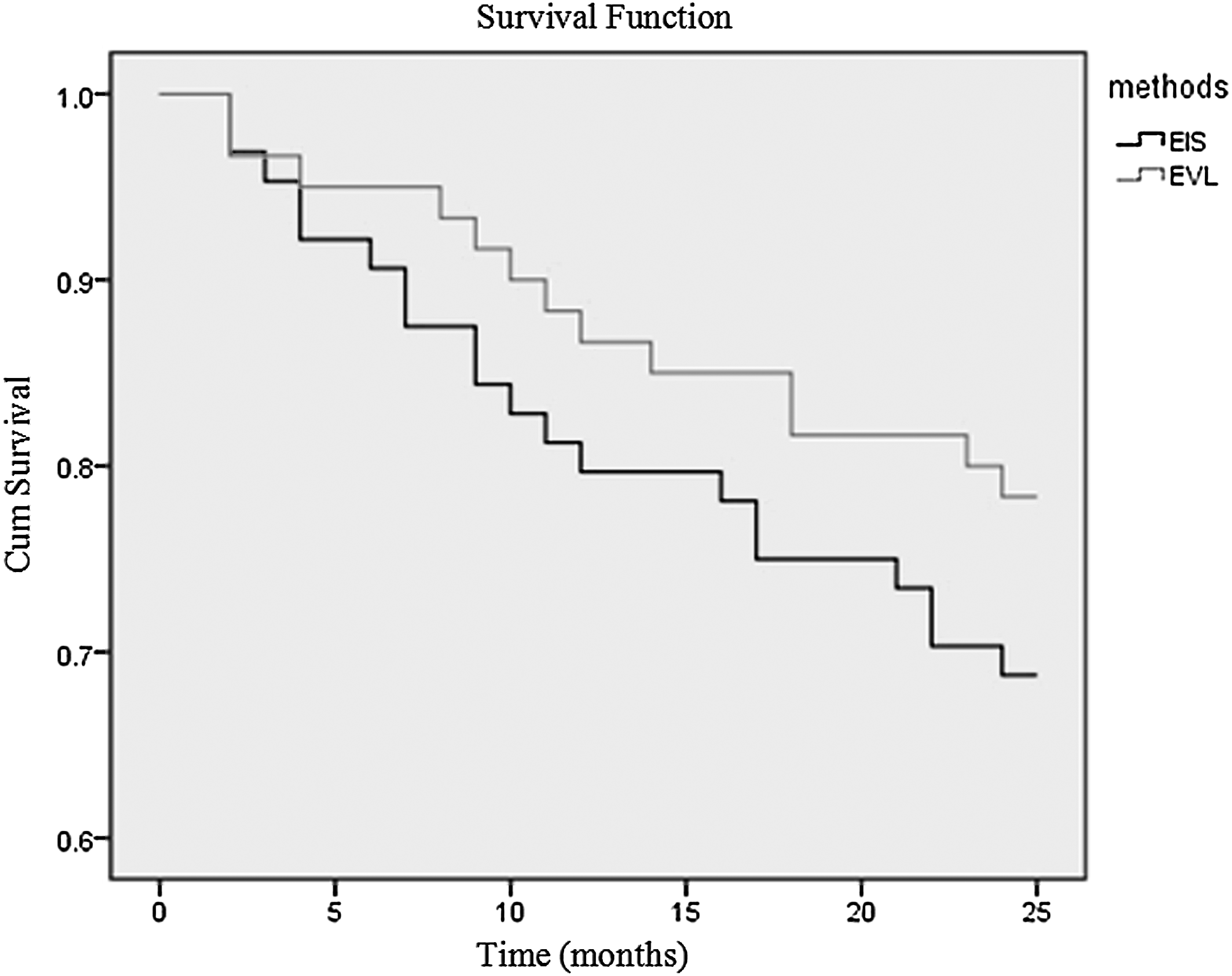
The cumulative survival curves after EIS and EVL. Survival shows no significant difference between the two groups (χ2 = 1.572, P = .21). EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
EIS, endoscopic injection sclerotherapy; EVL, endoscopic variceal ligation.
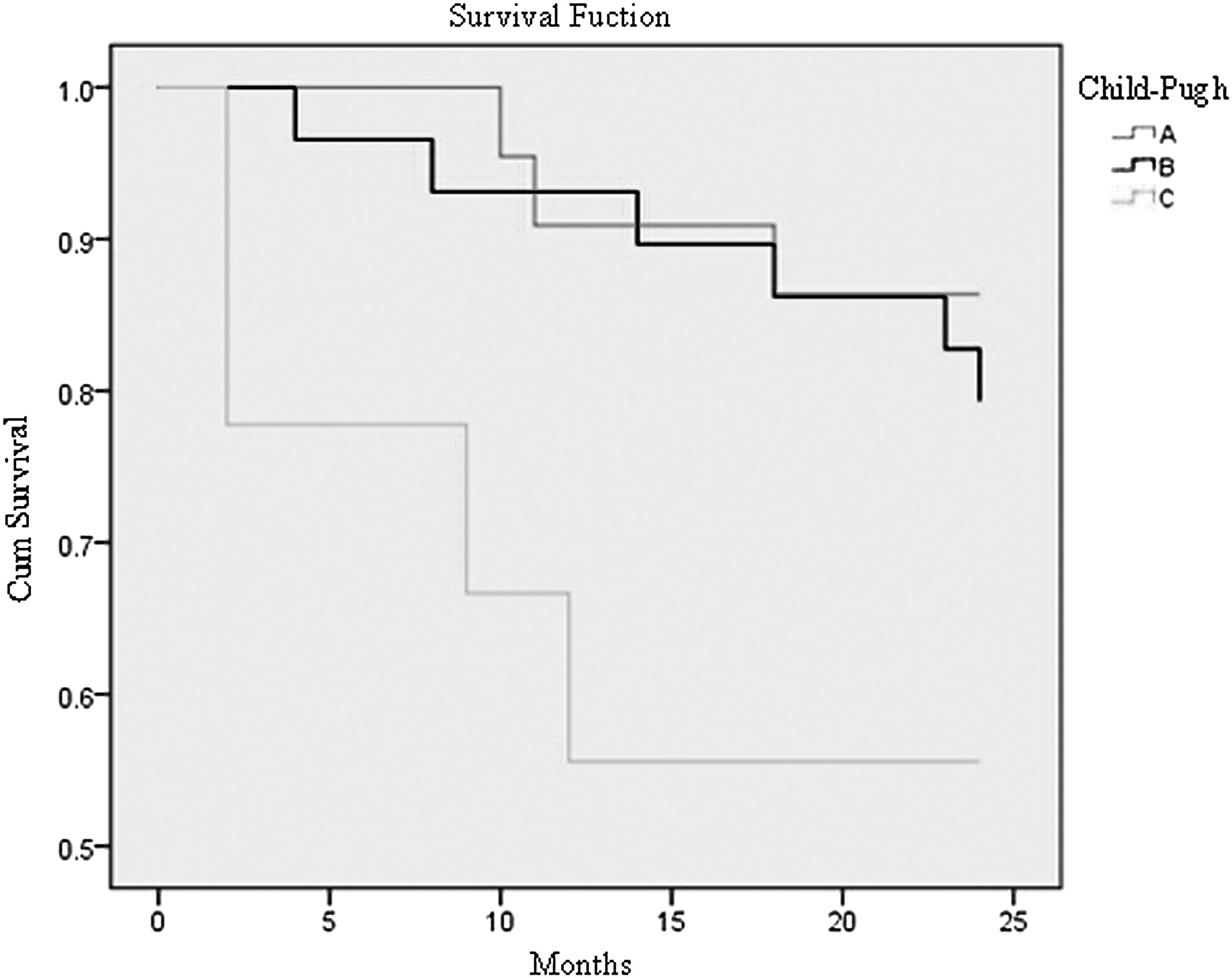
The survival curve for all patients is shown in Figure 3. Survival shows no significant difference between the two groups (χ2 = 1.572, P = .21). The cumulative survival curves according to Child Pugh classification (A–C) are shown in Figure 4. Fewer deaths occurred in Class A than Class B or Class C. (χ2 = 14.708, P = .001). The cumulative survival cures for all patients after EIS according to Child Pugh classification (A–C) are given in Figure 5. Fewer deaths occurred in Class A than Class B or Class C. (χ2 = 9.777, P = .008). The cumulative survival cures for all patients after EVL according to Child Pugh classification (A–C) (χ2 = 4.744, P = .093) are shown in Figure 6.
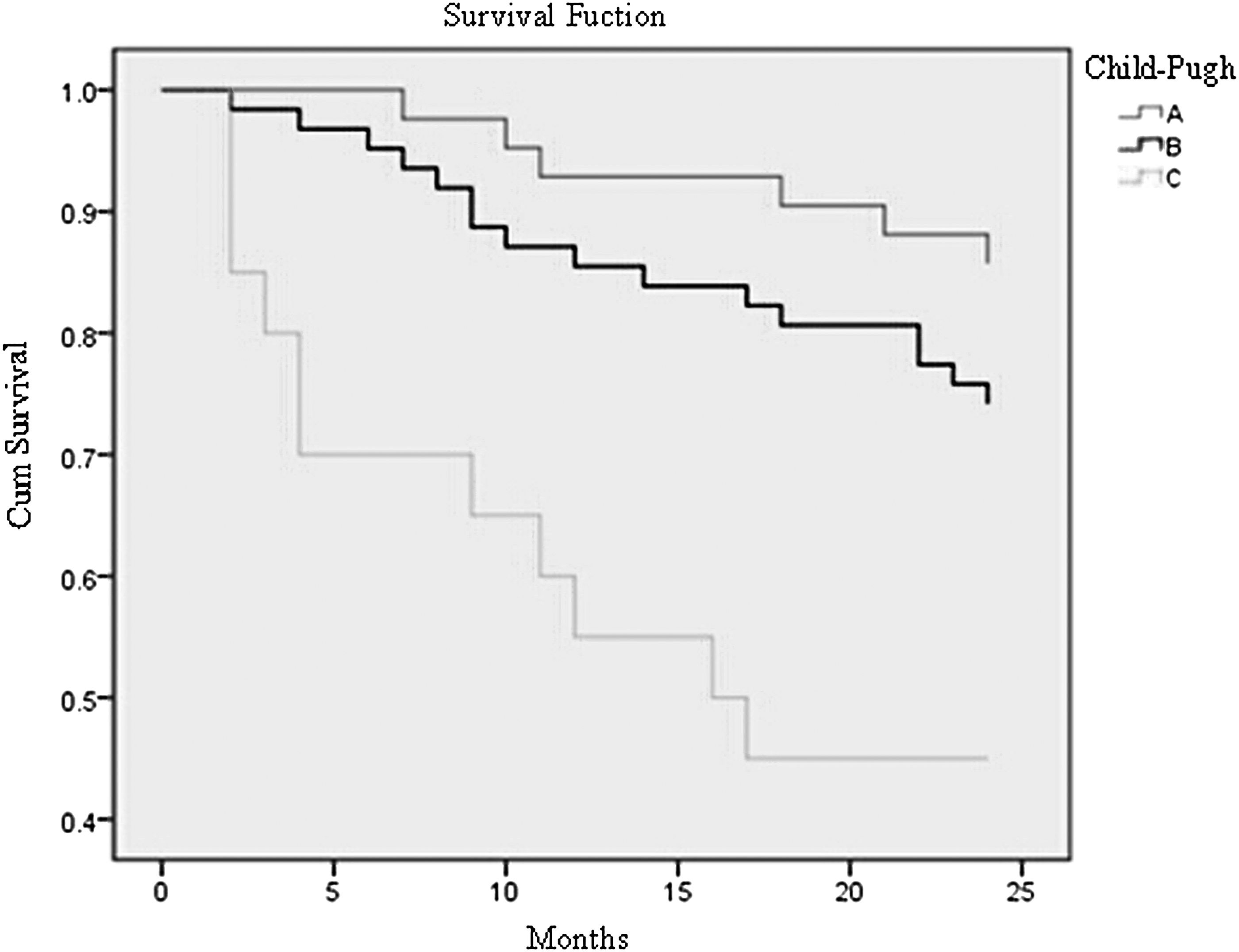
The cumulative survival cures according to Child Pugh classification (
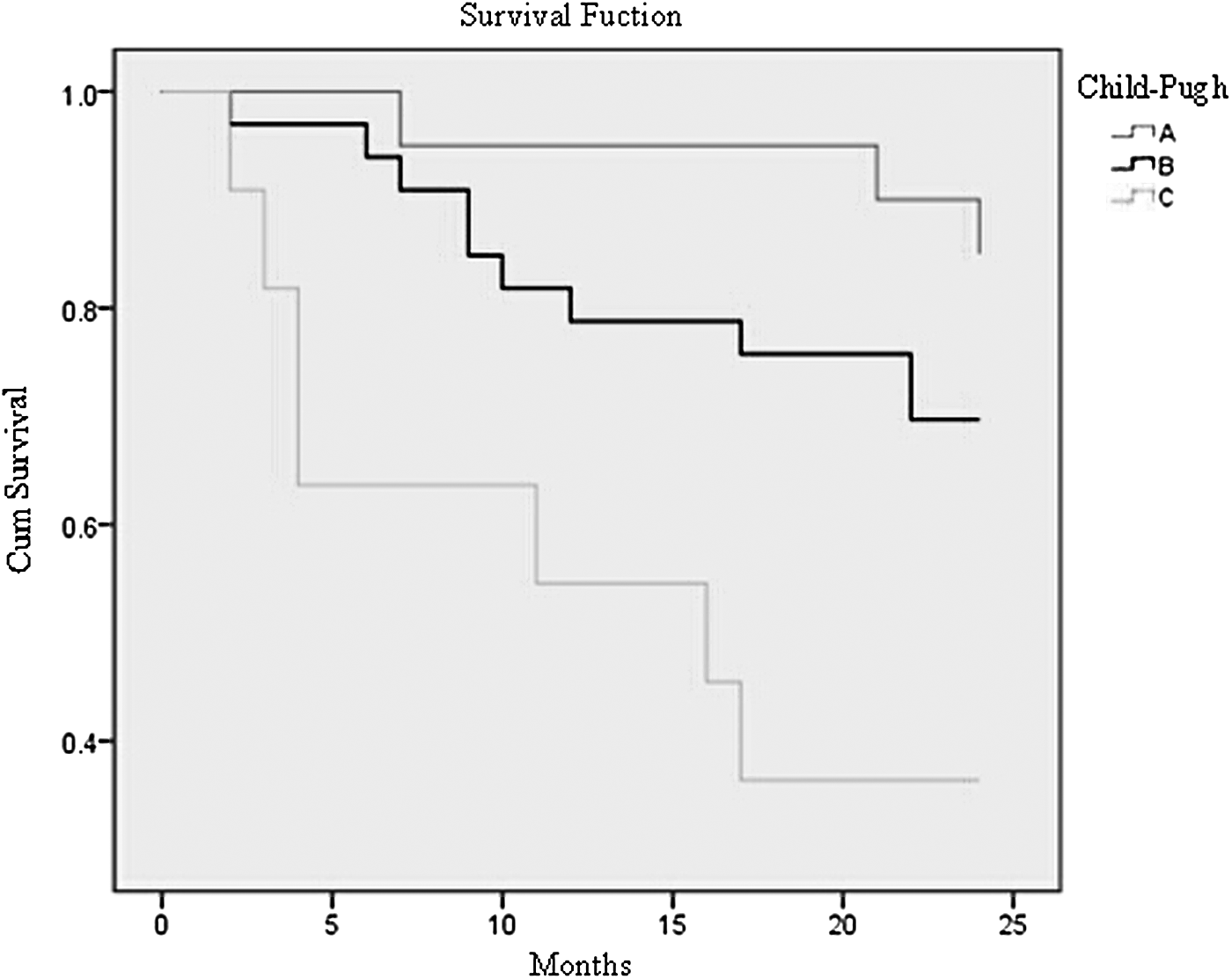
The cumulative survival cures for all patients after EIS according to Child Pugh classification
The cumulative survival cures for all patients after EVL according to Child Pugh classification (A, B, C). (χ2 = 4.744, P = .093). EVL, endoscopic variceal ligation.
Discussion
Since EVB is the main cause of the upper gastrointestinal bleeding and is associated with a high mortality rate, prevention of bleeding might be expected to result in improved survival. Both EIS and EVL are recommended for EVB because of their high safety and efficiency.23–26 Recently, many European and United States scholars have urged that the use of EIS should be replaced by EVL due to its complications,27–30 whereas Chinese and Japanese researchers hold different opinions. However, there has been a general consensus that EVL is easy to operate, requires shorter duration of time, less complication, and fewer sessions required to achieve varices elimination.18,22,31 In contrast, compared with sclerotherapy, EVL is less invasive because no sclerosant or sclerotherapy needle is used. 28 However, there are technical drawbacks with EVL, the main disadvantage of EVL is a higher frequency of variceal recurrence32,33 and is contraindicated when the vascular diameter is greater than 2.0 cm or less than 0.5 cm. The original single-band ligating device required repeated removal of the endoscope for reloading and reinsertion each time a new band was applied. 31 Moreover, fatal massive bleeding could result after successful EVL due to early spontaneous slipping of the rubber band,34–37 which is higher than previously reported. However, data from prospective randomized controlled trials comparing the efficacy and complications of EVL and EIS have shown more complications in EIS than EVL. Stiegmann et al. found band ligation to have improved survival and fewer complications than EVL. 28 Laine et al. reported a significant reduction in local complications, but no difference in rebreeding or mortality. 27 However, in our study, the rate of complications and survival were without statistical significance. Iwase et al., also showed that EIS was a safe procedure for EVB and provided good hemostasis with a low rate of recurrence, even over the long term. 38 It was reported that patients treated by repeated sclerotherapy must be diligently observed for development of extra esophagogastric varices.39,40 However, occurrence of extra esophagogastric varices in our study was rare and none was observed beyond 2 years after the initial EIS.
Experience of the operator is very important for both EVL and EIS. For EVL, we believe that dense ligation has better effects, which interrupt the blood supply faster, safer, and more efficiently. Although some bands dislodge too early, always there is little chance of fatal bleeding. EVL procedure should be started from the cardiac part of the stomach and progress upward in a helical manner in case of esophageal stricture. The proper distance between each band should be 1.5 cm. If the two adjacent bands are placed too close, the band would be easily dislodged due to the mechanical stress from adjacent band. Otherwise, incomplete endoscopic ligation may occur, leaving various residues. For EIS, we advocate the use of combination of intravascular and paravascular technique, which can eradicate varices and collateral vessels, causing the fibrosis of the lower esophageal submucosal tissue thus decreasing recurrence of varices. EVL compared with EIS is associated with more complications. However, with the development of latest endoscopic sclerosing technique and sclerosing agent used, there is small risk of severe complications, such as perforation, ectopic embolism, and hemorrhagic ulcer. Most of the complications show minor symptoms and do not need further treatment. When EIS is applied, the injection angle should be well adjusted, and vertical pierce should be avoided, especially for paravascular injection. A 60 mL of Lauromacrogol was injected in a patient in EIS group who died later. We suggest the use of 35 mL for intravascular injection up to 50 mL for one session. Operator should not increase injection volume blindly to achieve hemostasis. With the help of transparent cap, operator can adjust angle and depth of injection more easily and quickly and improve the efficiency of EIS. Meanwhile, one should be meticulous to reduce the unnecessary scratch between the cap and varices.
It is still controversial whether EIS should be replaced by EVL. Our results suggest that EIS and EVL are equally efficient for the control of acute variceal bleeding and prevention of rebleeding. To make a better choice, we should consider the condition of hospital, the experience of the operator, and the characteristics of the esophageal varices. We believe that EIS is irreplaceable for esophageal varices bleeding (EVB) because of the following reasons. (1) Many large-scale clinical studies had proved the safety and efficiency of EIS. But so far, no studies of EVL with a sample capacity more than 1000 have been reported. Besides, strict randomization cannot be achieved in clinical treatment in patients with vascular diameter greater than 2.0 cm. Varices in this part are usually very severe. So there is higher risk of postoperative complications and poor efficiency and prognosis. (2) A meta-analysis comparing the use of sclerotherapy and band ligation was published in 2006, concluding that both band ligation and sclerotherapy are safe and effective. No differences in mortality were found, and sclerotherapy was considered as the first-choice therapy for cases of bleeding. 41 EIS has a better effect in preventing variceal recurrence, and there are no limitations of Child Pugh and the vascular diameter. Emergency EIS can be repeated if the first treatment failed to control active bleeding. (3) EIS shows incomparable advantages over EVL in the control of acute bleeding. When EVL is used, it is necessary to withdraw the endoscope for system assembly, and distal cap with the bands restrict the endoscopic field of view and may allow pooling of blood, further obscuring the endoscopes' view. Besides, varices shrivel and become difficult to be sucked after bleeding. This makes EVL difficult to perform, potentially increasing the procedure time and complication risk. In contrast, sclerosing agents can be injected immediately after the endoscopic diagnosis of esophageal variceal rupture, which is extremely important to save time for emergency hemostasis. (4) Patients with Child-Pugh C often show significant hypoalbuminemia, portal hypertension gastropathy, and coagulopathy. There are also physiopathologic changes in esophageal mucosa, including hyperemia, edema, increased brittleness, and gastrointestinal motor function obstacle, prone to reflux and antiperistalsis. This increases the risk of early band detachment. Due to coagulopathy, thrombosis and organization require longer time and massive hemorrhage may occur. In such cases, endoscopy cannot be repeated because of ligation bulb. Unfortunately, TIPS is not widely available and the patient may not be suitable for surgery because of poor liver function and ascites. These severe complications are associated with extremely high mortality rate. A case–control study involving 605 patients showed that 21 patients developed early spontaneous band slippages with bleeding on post banding ulcer, and 11 of the 21 patients (52%) died within a few days. 34 We cannot ignore the deficiencies in China healthcare system and the poor medical literacy of the general public. Medical disputes have become a serious issue in China. Family members often cannot accept the perioperative mortality and there is high probability of medical disputes. (5) It is well recognized that esophageal collateral vessels play an important role in variceal recurrence. 42 Effective ways to eliminate the collateral vessels may develop a new breakthrough in future research. From this point of view, EIS seems more promising than EVL.
On the basis of similar rates of rebleeding, mortality, and complications (local complications and systemic complications) and similar rates of variceal eradication, our research has found that EIS and EVL are both appropriate endoscopic treatment options for patients with EVB. In conclusion, our study confirms the feasibility, efficacy, and safety of EIS and EVL in the management of EVB.
Footnotes
Disclosure Statement
No competing financial interests exist.