
Abstract
Abstract
Objectives:
Selective circular myotomy (CM) is recommended in peroral endoscopic myotomy (POEM) for achalasia, but completeness of myotmoy is the prerequisite for excellent long-term results of conventional surgical myotomy. The aim of our study was to compare the efficacy and safety between peroral endoscopic full-thickness and simple CM for the treatment of severe achalasia.
Materials and Methods:
A total of 123 severe achalasia patients who underwent POEM from August 2011 to May 2013 were included. They were divided into circular or full-thickness myotomy (FTM) groups according to the depth of myotomy. Demographics, Eckardt score, procedure-related parameters, perioperative adverse events, pre- and postoperative esophageal diameter, esophageal manometry, and follow-up results were retrospectively collected and compared between the two groups.
Results:
All the 123 patients underwent POEM successfully, and the mean operation time was significantly shorter in FTM group compared with CM group (57.4 ± 8.2 minutes versus 63.2 ± 12.3 minutes, P < .05). There was no significant difference between the two groups in terms of treatment success, pre- and postoperative Eckardt score, esophageal diameter, esophageal manometry, and perioperative adverse events (P > .05). Twenty-four-hour pH monitoring was performed in 19 patients (11 in FTM, 8 in CM). Although no statistical difference was detected in rate of abnormal esophageal acid exposure between groups, this rate was higher in FTM group than CM group (60% versus 40%, P > .05).
Conclusion:
Treatment efficacy in short-to-medium term are comparable between circular or FTM. FTM significantly reduce the operative duration, but it may increase potential risk of gastroesophageal reflux disease incidence.
Introduction
A
Peroral endoscopic myotomy (POEM) was introduced as a novel promising treatment by Inoue et al. in 2010. 7 This minimally invasive therapy was subsequently reported to relieve symptoms and improve quality of life in short to intermediate terms.8–12 Generally, POEM is recommended to divide circular muscle fibers alone and preserve the longitudinal esophageal muscle fibers to avoid entering the pleural cavity and decrease morbidity.13–15 However, completeness of myotomy involving both circular and longitudinal layers is the prerequisite for sufficient and long-term reduction of LES pressure and the basis for excellent results of conventional surgical myotomy.16,17 In our early practice, we performed simple circular myotomy (CM) for all patients with achalasia, but we found that some patients could not receive satisfactory outcome, and those patients generally have following characteristics: severe clinical symptoms (Eckardt score ≥6), esophagus expansion (diameter ≥6 cm), or sigmoid-type esophagus. We consider those that meet at least one of the above points as severe achalasia, and began to perform full-thickness myotomy (FTM) for severe achalasia patients in our center after March 2012. In this study, we retrospectively collected clinical data to compare the safety and efficacy between peroral endoscopic full-thickness and circular muscle myotomy.
Materials and Methods
Patients
A total of 123 severe achalasia patients were retrospectively collected in our center from August 2011 to May 2013, and most of the patients who received FTM were admitted after March 2012. The inclusion criteria for enrollment were as follows: (1) Diagnosis of achalasia on the basis of clinical symptoms, barium esophagogram, esophagogastroduodenoscopy (EGD), and high-resolution manometry (HRM). (2) Severe achalasia was considered when at least one of the following points are met: (a) Eckardt score 18 : preoperatively ≥6; (b) diameter of esophagus ≥6 cm; and (c) sigmoid-type esophagus. (3) Patients consent to undergo POEM procedure at our hospital. Exclusion criteria were active esophagitis or giant ulcer at EGJ and pseudoachalasia, a secondary achalasia, which is usually associated with malignancy rather than idiopathic neuromuscular dysfunction of esophageal motility. 19 Also, patients with severe coagulopathy, cardiopulmonary disease, or other disease that lead to intolerability of EGD or operation should be excluded as well. The study was approved by the Ethics Committee of the Second Xiangya Hospital, Central South University. Informed consent was obtained from all patients before the procedure was performed. And all of them were notified of possible complications and other possible treatment options.
POEM procedures
Prophylactic intravenous antibiotics and proton pump inhibitors (PPI) were introduced before the procedure. POEM was performed under general anesthesia via tracheal intubation using a standard single-channel endoscopy (GIF-Q260Z; Olympus, Tokyo, Japan) with a transparent cap (D-201-11802; Olympus) attached to the front. CO2 insufflator (UCR; Olympus) was used. Other equipment and accessories included a high-frequency generator (VIO 200; ERBE, Tübingen, Germany), an argon plasma coagulation unit (APC300; ERBE), an injection needle (NM-4L-1; Olympus), a hybrid knife (ERBE), a dual knife (KD-650L; Olympus), and hemostatic clips (HX-600-135; Olympus). The POEM procedure was performed as reported and shown in Figure 1. 20 A submucosal injection was made into right posterior esophageal wall at about 10 cm proximal to the EGJ. Submucosal tunnel entry was created via a 2 cm longitudinal incision, with at least 0.5 cm lateral dissection along both sides. 21 And the tunnel was created, passing over the EGJ, and 3 cm into the proximal stomach. The myotomy was performed starting from 2 to 3 cm distal to the mucosal entry point to the 3 cm distal to the EGJ in all patients. In circular myotomy (CM), selective circular muscular bundles were resected and the outer longitudinal muscle bundles remained. While in peroral endoscopic FTM, both internal circular and longitudinal muscle layers were resected within a range of 6 cm from the EGJ. After thorough hemostasis, the mucosal entry site was closed with several endoscopic clips.
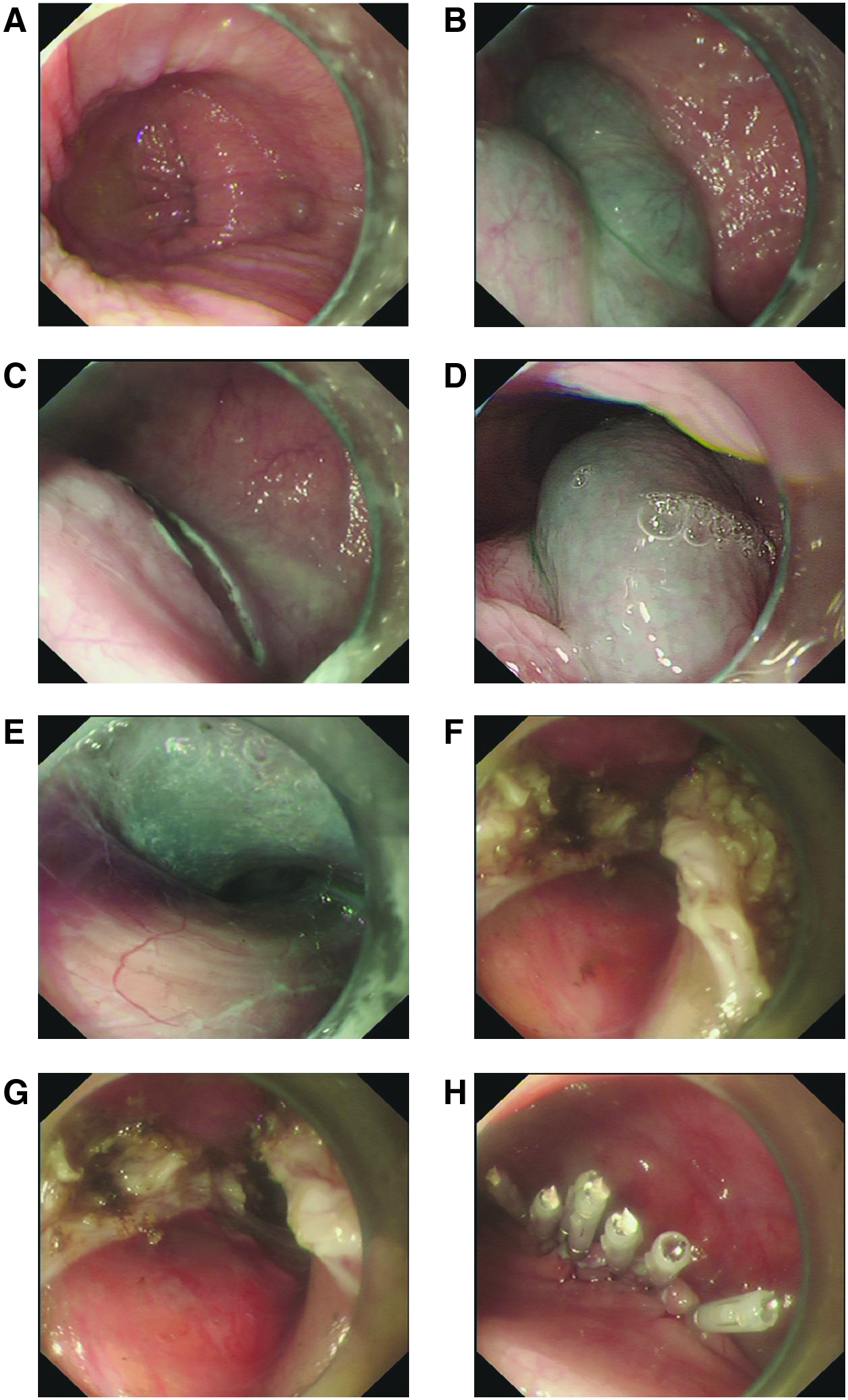
Case illustration of endoscopic FTM.
Postprocedure management
Patients were kept nil per os for 24 hours, a liquid diet for an additional 3 days, and returned gradually to a normal diet within 2 weeks. Intravenous PPI and antibiotics were used for 3 days after POEM. On postoperative day 2, a thoracoabdominal X-ray, or sometimes a chest computed tomography scan were carried out to evaluate procedure-related complications such as subcutaneous emphysema, pneumothorax, pneumoperitoneum, and pleural effusion.
Definition and assessment
1. The efficacy of achalasia treatment is assessed with several metrics including the widely used after-treatment Eckard score of ≤3, LES pressure decrease (usually >50% decrease), and improvement of esophageal emptying as assessed by barium esophagram. 15
2. The safety of treatment is assessed with perioperative adverse events and late adverse events occurred in follow-up.
3. Treatment success was defined as a post-myotomy Eckadt score ≤3.
4. Treatment failure was defined as Eckadt score > 4 within postoperative 6 months.
5. Perioperative adverse events were defined as incidences that occurred intra- or postoperatively during hospital stay, like infection, bleeding, gas-related complication, and mucosal perforation.
Follow-up
Patients were scheduled for a follow-up visit at 1, 3, 6, and 12 months after POEM for EGD and symptom assessment. Then, every 6 months thereafter by telephone to obtain Eckardt score and annually for EGD to observe the status of esophageal closure and check for any signs of reflux esophagitis. They also underwent barium swallow to evaluate the esophageal diameter at postoperative month 6 and some of them took HRM and 24-hour pH monitoring.
Statistical analysis
SPSS version 17.0 was used for data analysis. Continuous variables were presented as mean ± standard deviation and analyzed using Student's t-test. Non-continuous variables were expressed as median-range and evaluated using Wilcoxon signed-rank test. Paired variables in the same patient before and after surgery were compared using the repeated measure of analysis of variance. And qualitative data were calculated using the chi-square test. A two-tailed P < .05 was considered as statistically significant in all cases.
Results
Patient characteristics
We enrolled 123 patients (mean age 42.1 years, range 14.0–74.0 years) with average disease course of 5 years (range 0.5–33 years). Among them, 70 cases underwent FTM and 53 cases received CM. Besides, 18 cases had previous therapies and 11 were accompanied by sigmoid-type esophagus. The demographics, median history, previous treatments, achalasia type, and preoperative evaluations (Eckardt scores, esophageal diameter) between groups were comparable as detailed in Table 1.
CM, circular myotomy; FTM, full-thickness myotomy; SD, standard deviation.
Procedure-related parameters
All patients underwent POEM successfully, and the operative time was shorter in FTM group (57.4 ± 8.2 minutes versus 63.2 ± 12.3 minutes, P < .05). The average lengths of tunnel and lengths of myotomy between two groups were both comparable as detailed in Table 1 (P > .05).
Perioperative adverse events
A total of 14 patients (11.4%) encountered perioperative adverse events, 8 cases (11.4%) were in FTM group, and 6 cases (11.3%) were in CM group. There was no statistical difference (P > .05). Three patients had small mucosal perforations that were closed by 1 to 2 hemostatic clips. Gas-related complication occurred in 11 cases, and 10 of them were simple neck subcutaneous emphysema and 1 was mediastinal emphysema plus subcutaneous emphysema. Those with simple subcutaneous6 emphysema were self-absorbed within 3–5 days, and no special intervention was required. The one with mediastinal emphysema plus subcutaneous emphysema suffered from chest tightness, and the symptom relieved after deflation via subcutaneous puncture.
Follow-up results
The median duration of follow-up was 30 months (range from 24 to 46 months). The treatment success was similarly achieved between FTM group and CM group during periodical follow-up (98.6% versus 98.1%, P > .05). One patient in each group encountered treatment failure and both of them achieved symptom remission after further treatment of balloon dilation. There were four patients lost to follow-up in our study, and the loss rate of follow-up was 3.3% (4/123). The Eckardt score dramatically decreased after POEM in each group (P < .05), but the difference between two groups in the same period was not statistically significant (Table 1). The mean esophageal diameter in FTM group decreased postoperative and in CM group (P < .05). However, there was no statistical significance in pre- and postoperative esophageal diameter between the two groups (P > .05). Among the 11 patients with sigmoid-type esophagus, 10 cases had postoperative morphological improvement that includes curvature straightness and diameter reduction, but the other one has little change. The illustration of one case with morphological change was presented in Figure 2.

Case illustration of barium swallow before and after POEM.
Before POEM, the LES pressure was measured in total 123 patients, and it was 35.02 ± 7.28 mmHg in FTM group and 34.02 ± 6.84 mmHg in CM group. After POEM, 33 patients in FTM group and 28 patients in CM group underwent HRM at 6-month postoperatively, and the others refused to undergo esophageal manometry especially for those with apparent symptom remission. Mean LES pressure significantly decreased to 11.58 ± 5.31 mmHg in FTM group and to 12.08 ± 4.92 mmHg in CM group (P < .05) and both reductions achieved the treatment efficacy. There was no statistical difference between the two groups in pre- and post-treatment LES pressures. Figure 3 showed that in a patient with type II achalasia the LES pressure decreased after POEM.
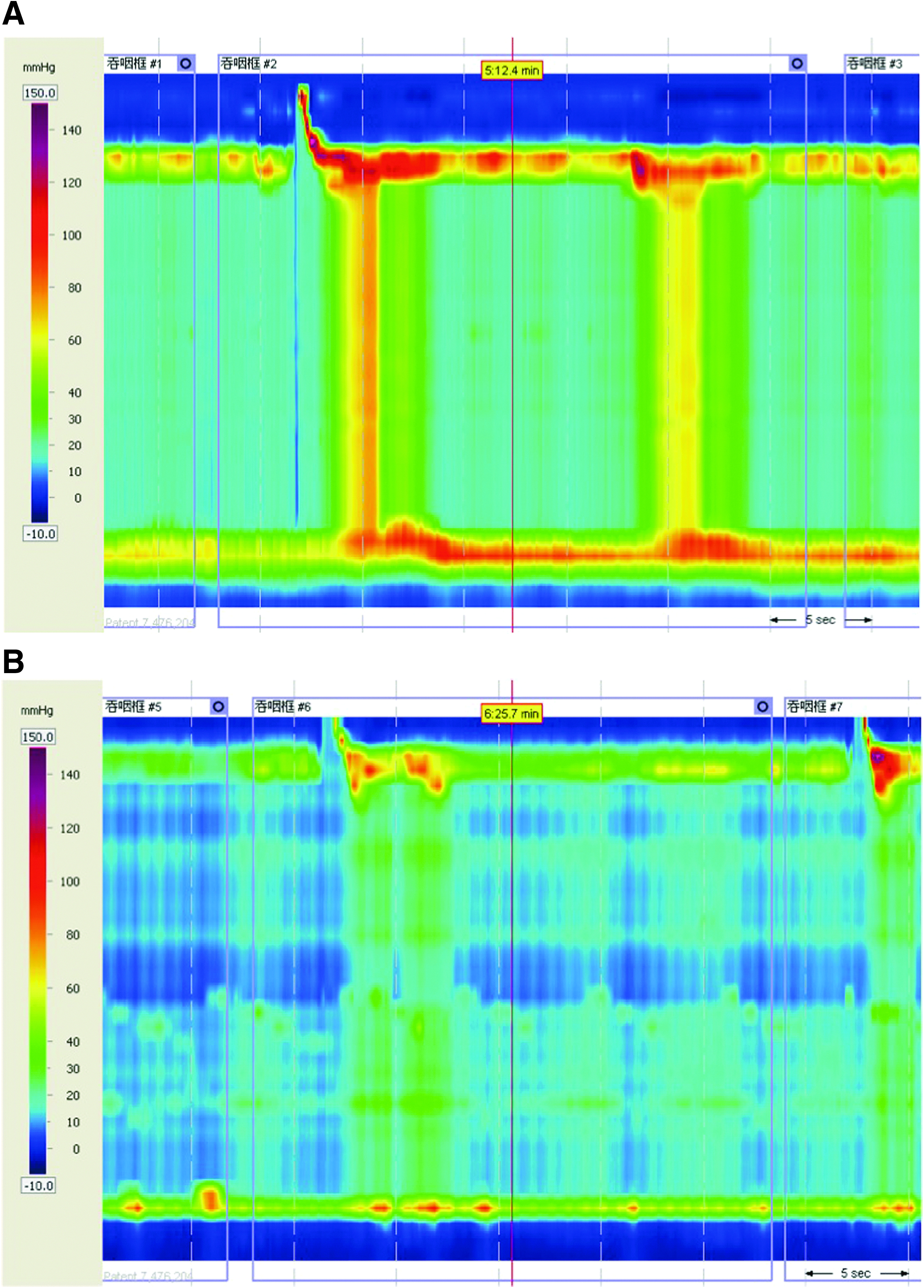
HRM outcomes before and after POEM
Twenty-four-hour esophageal pH monitoring was performed in 19 of 123 patients (11 in FTM, 8 in CM). Abnormal esophageal acid exposure was attested in 10 patients (6 in FTM, 4 in CM), which was defined as percentage total reflux time (esophageal pH <4) >5%. No statistical difference was detected in rate of abnormal esophageal acid exposure between groups, but this rate was higher in FTM group than CM group (60% versus 40%, P > .05). Among them, 6 patients had esophagitis with gastroesophageal reflux disease (GERD) symptoms (4 in FTM, 2 in CM) and the other 4 patients had no typical symptoms (2 in FTM, 2 in CM). Clinical characteristics of the 6 patients with esophagitis were detailed as Table 2. They all suffered from reflux symptom 2–12 months after POEM and EGD revealed reflux esophagitis. Five of them were relieved after oral PPI for 2 months and the other one needed intermittent administration.
A: Grade A—one or more mucosal breaks no longer than 5 mm that does not extend between the tops of two mucosal folds; B: Grade B—one or more mucosal breaks more than 5 mm that does not extend between the tops of two mucosal folds; CM, circular myotomy; FTM, full-thickness myotomy.
Discussion
POEM has become an effective therapeutic option for achalasia and its efficacy has been demonstrated by an international prospective multicenter clinical trial. 22 Differing from pneumatic dilation that usually accompanied unfavorable recurrence, 23 POEM could achieve exciting short to intermediate term efficacy.10–12 POEM has a comparable efficacy with HM and it takes advantages in a shorter operative time and a lower complication rate. 24 Furthermore, POEM was reported to be safe and feasible for patients at extremes of age and for those with prior endoscopic interventions or conventional surgery.25–28 During POEM for achalasia, a selective CM preserving the longitudinal outer esophageal muscle was generally recommended, which is designed to avoid gas-related complications and decrease risk of GERD.13–15 However, completeness of myotomy is the prerequisite of sufficient and long-term reduction of LES pressure, and is the basis for excellent results of conventional surgical myotomy.16,17 Whether FTM will result in better symptom relief compared with CM for achalasia patients is not yet clear.
In our early experience, we found that those severe achalasia patients who received simple CM could not acquire satisfactory efficacy, and FTM was intended for them. Those patients usually had severe symptoms or obvious radiological change, in our observation. As we know, clinical symptoms were generally assessed by Eckardt score and radiological change could be graded by Henderson’ criteria, 29 therefore we consider those patients had severe achalasia when they met at least one of the following points: (a) Eckardt score preoperatively ≥6; (b) diameter of esophagus ≥6 cm; and (c) sigmoid-type esophagus. Recently, several researchers have explored FTM by animal experiments and clinical studies. Both of them indicated that there was no statistical difference between the two types of myotomy in symptom relief, but FTM could decrease the procedure time and might be superior in rapid esophagogastric emptying.9,30,31 Our results showed that FTM is as good as CM in aspect of symptom relief, that is FTM did not reveal significant superiority in dysphagia improvement, as a result of the fact that postoperative Eckardt scores and esophagus diameter were comparable between two groups in short-to-medium follow-up. There was no significant difference in parameters comparison except operation time, which mirrored the findings of previous reports. 31 However, whether FTM will enhance long-term benefit for severe achalasia patients still needs further investigation.
Although parts of CM were accomplished earlier in the series, all POEM procedures were completed by a single senior operator (D.L.) in our center. Moreover, for an experienced endoscopist, resected curve may be on a platform and operating duration tended to be stable after about 20 cases practices. 32 Thus, skillful performance may not be regarded as an important factor for the shorter procedure time. In addition, the longitudinal layer is relatively thinner, which is close to the circular layer and has weak connection with the periesophageal membrane. FTM may reduce the time for dividing the circular and longitudinal muscular layer. Moreover, our prior studies have demonstrated that the myotomy depth is not a risk factor for gas-related adverse events during POEM. 20 Because of intraoperative mechanical trauma or electrocautery damage during CM procedure, unintentional splitting of longitudinal muscle is likely to occur so that integrity of the outer longitudinal muscle fibers is hard to preserve. It might be one of the reasons for the high events of gas-related complication in simple CM. In our opinion, to prevent gas-related complication, one of the most important steps is to maintain the integrity of periesophageal or serous membrane rather than overemphasize the integrity of longitudinal muscle.
GERD is another question of common concern for patients undergoing FTM. In our retrospective study there were only 19 patients who underwent 24-hour pH test, and abnormal esophageal acid exposure was attested in 10 patients. The esophagitis incidence was detected in 6 patients who underwent EGD after POEM. The abnormal esophageal acid exposure rate was higher in FTM group than CM group (60% versus 40%) and the reflux esophagitis incidence was increased as well (67% versus 33%). Although no statistical difference was detected in both abnormal esophageal acid exposure and reflux esophagitis rate between two groups, which may be due to the small sample size, it showed a tendency that FTM would increase GERD rate. So we consider FTM may increase potential risk of GERD incidence compared with CM. Besides, it is worthy to mention that accurate GERD incidence in two options is still uncertain and further investigation is warranted.
Limitations of our study include that it was a retrospective design and there was a lack of overall evaluations like esophageal manometry and 24-hour pH testing, as those who had symptoms relief were more likely to refuse the assessment. Besides, reflux esophagitis incidence is not equal to GERD occurrence, which may lead to an underreported rate of GERD. We will continue to gather and analyze data of esophageal manometry especially for the long-term outcomes.
In conclusion, compared to simplex CM with FTM for severe achalasia patients, the treatment efficacy and safety were similar in short-to-medium term. FTM significantly reduce the operative duration, but it may increase potential risk of GERD incidence.
Footnotes
Disclosure Statement
No competing financial interests exist.