
Abstract
Abstract
The treatment for achalasia changed dramatically after the introduction of minimally invasive surgery. Since 1991, laparoscopic Heller myotomy (LHM) has replaced pneumatic dilatation (PD) as the primary form of treatment in many centers. Over time, PD became safer, and eventually endoscopic experts were able to perform an endoscopic myotomy via a per oral endoscopic myotomy (POEM). This article reviews the advantages and disadvantages of each technique. Ultimately, the best outcomes are obtained by a multidisciplinary team that can tailor a specific treatment to each individual patient.
Introduction
T
This review focuses on the three treatment modalities—PD, LHM, and POEM—currently available for the treatment of achalasia.
Heller Myotomy and Fundoplication
Myotomy of the lower esophagus was introduced in 1913 as an alternative to the cardioplasty, the preferred treatment at the time. Over the past 100 years, the technique evolved from a double myotomy via an open abdominal approach to a single myotomy plus a fundoplication through a laparoscopic approach. 6 Today, there is a consensus among most surgeons that a partial fundoplication, either anterior or posterior, should be added to the myotomy. 7 This article describes a Dor fundoplication, since the fundus covers the exposed esophageal mucosa while providing reflux protection.
Technique
The patient is positioned in a steep reverse Trendelenburg position. This modified lithotomy position may be set with the legs on stirrups or on operating tables that allow separation of the inferior portion. The legs should not be flexed above 30° to avoid knocking of the thighs with instruments or the surgeon's elbows. A beanbag and/or straps may keep the patient in position and prevent sliding. The video monitor is placed at the head of the patient. Additional lateral monitors help ergonomics of the assistants.
The surgeon stands between the patient's legs with one assistant to his right and one to his left to hold a 30° camera. The scrub nurse is usually positioned to the left, close to the camera assistant.
Positioning of the trocars
The trocars are positioned by following the same principles of an antireflux operation. Usually, a midline trocar is placed in the 14 cm distal to the xyphoid process and used for the laparoscope (usually a trocar for a 10 mm camera, although some surgeons opt for a 5 mm camera). The surgeon's hands operate through ports located under the right and left costal margins, at the level of the mid-clavicular line (usually a 5 mm trocar for the left hand and a 10 mm trocar for the right hand). A trocar (5 mm) in the left flank is used by the assistant to retract the stomach. The liver is retracted via a port on the right flank (with a fan-shaped or ideally a paddle-shaped retractor) or, alternatively, at the levels of xiphoid, since both a fan retractor and a Nathanson are viable options.
Dissection of the hiatus and distal esophagus
The dissection proceeds similar to an antireflux operation. The gastro-hepatic ligament is divided, exposing the right bundle of the right crus of the diaphragm. The esophagus is then separated from the hiatus by division of the phreno-esophageal membrane and blunt dissection that continues clockwise to the left bundle of the crus. The posterior portion of the esophagus is not dissected unless a concomitant hiatal hernia is present and a hiatoplasty is anticipated, or if a sigmoid-shaped esophagus requires circumferential dissection of the esophagus to achieve a straight axis.
The distal esophagus is dissected anteriorly and laterally into the mediastinum for at least 6 cm to ensure exposure and the anterior vagus nerve is preserved.
Myotomy
Before the myotomy is started, the fat pad overlying the esophagogastric junction and angle of His is removed. The upper and lower extents of the myotomy are demarcated with the electrocautery to facilitate an adequate and straight myotomy. The myotomy extends from 2 to 3 cm below the esophagogastric junction to 5–6 cm above the junction. At the esophagogastric junction, the separation of the muscular from the submucosa layers is more difficult; thus, the myotomy should not start on this area but just above this zone and should continue superiorly. This region also allows the surgeon's arms to abduct and extend naturally.
The plane between the muscular layer and the submucosa may be achieved with a hook, scissors or tearing the muscles with two graspers. The correct plane is recognized easily by the vascular pattern of the submucosa and the herniation of the submucosa between the edges of the muscular layer. Once this plane is reached, the myotomy is continued superiorly with the aid of a hook cautery, scissors, or harmonic scalpel. The creation of a tunnel between the muscular and submucosa with gentle blunt dissection facilitates subsequent division of the muscular layer. After the esophageal myotomy is completed and the surgeon is confident about the correct plane, the myotomy is extended caudally. The loss of the longitudinal and circular pattern of the muscular layers to an oblique orientation demarks the esophagogastric junction (Fig. 1).

Esophagocardiomyotomy (Heller's myotomy). Myotomy should extend from 2 to 3 cm below the esophagogastric junction to 5–6 cm above the junction. The plane between the muscular layer and the submucosa may be achieved with a hook, scissors or tearing the muscles with two graspers
Bleeding from small vessels may occur during the myotomy. Diathermy is avoided to control bleeding, since a thermal injury may occur and increase the risk of a delayed leak (24–48 hours later). Simple compression of the vessel for a couple of minutes guarantees hemostasis.
Insufflation of the area of the exposed submucosa with an orogastric tube positioned at the esophagogastric junction not only allows identification of undetected small perforations but also allows identification of residual muscular fibers. These fibers produce a waist that prevents full protrusion of the submucosa through the muscular defect. If a mucosal tear is found, it is repaired with fine interrupted absorbable sutures and the closure is tested with saline and methylene blue. Intraoperative endoscopy or manometry may be used but is not required using this technique.
Dor fundoplication
The Dor fundoplication is an anterior partial fundoplication, with the gastric fundus anchored to the left and right borders of the myotomy. The procedure is started at the left border where three interrupted non-absorbable sutures secure the fundus to the esophagus. The uppermost stitch incorporates the gastric fundus, the left side of the esophageal wall, and the left pillar of the crus. Division of the short gastric vessels ensures a tensionless rotation of the fundus to the right. The fundoplication does cover all the exposed submucosa, otherwise the wrap would be too long and intrathoracic. The fundoplication covers the esophagus below the diaphragm. Further rotation of the gastric fundus to the right allows the surgeon to anchor the fundoplication to the right border of the esophageal myotomy. Again, three sutures are used, and the uppermost includes the stomach, the esophagus, and the right bundle of the crus. In addition, two or three stitches may be placed between the gastric fundus and the rim of the esophageal hiatus (without incorporating the esophageal wall) to decrease the tension along the right row of sutures (Fig. 2).
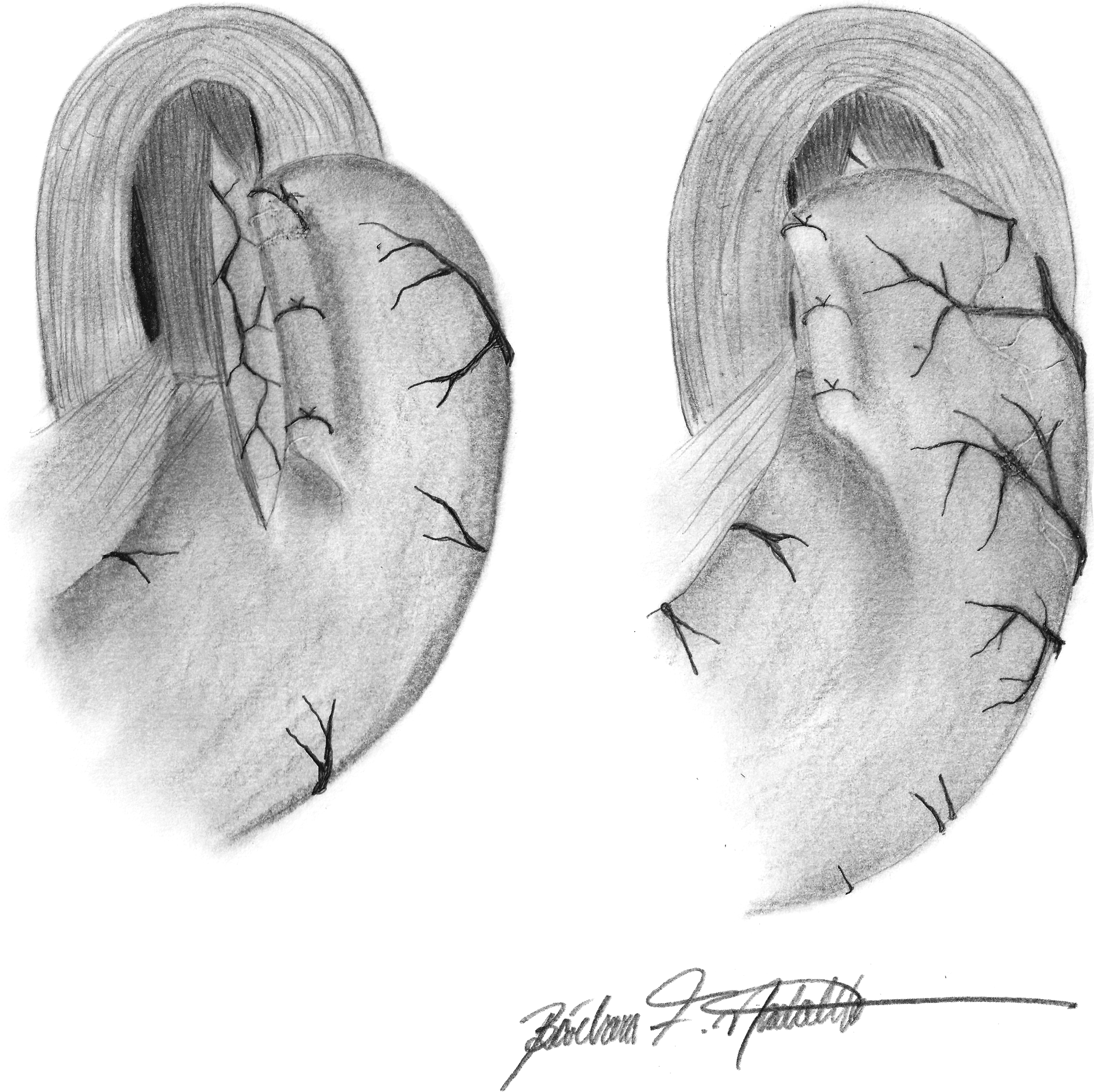
Dor fundoplication. The procedure consists of an anterior partial fundoplication with the gastric fundus anchored to the left and right borders of the myotomy and diaphragm.
Advantages
LHM with a fundoplication is a safe procedure. Complications associated to this procedure occur in <5% of the cases according to nationwide studies. 8 Mortality is <0.1%.8,9 Although length of stay is usually 1 or 2 days, 9 some surgeons even perform the operation as a same-day procedure. 10
There are a few reports of a Heller myotomy with the robotic platform, although clinical outcomes are similar to the laparoscopic technique. 11
Disadvantages
The main side effect of LHM is gastroesophageal reflux (GER), even when a fundoplication is added to the procedure. GER occurs after ablating the lower esophageal sphincter and is accentuated by aperistalsis and slow acid clearance. Table 1 shows that objective evaluation of GER by pH monitoring ranges from 3% to 42%. Tracings should be carefully reviewed to exclude pseudo-reflux.
Outcomes
Dysphagia is resolved in 90%–95% of patients at 5 years, and in 80%–90% of patients at 10 years. 8 Reoperative rate for dysphagia recurrence is ∼2%. 20
Pneumatic Dilatation
Forceful dilatation of the cardia was the first treatment for achalasia and is based on the disruption of the lower esophageal sphincter (LES). The technique of dilatation has evolved from rigid dilators to hydrostatic balloons that are designed to achieve maximum and controlled volume with a low pressure to improve efficacy and prevent esophageal perforation. 21
Technique
There is no consensus on the ideal diameter of the balloon (ranging from 30 to 40 mm), the need for fluoroscopic guidance during the procedure, and the length of time that the balloon is inflated. 22
Using fluoroscopic guidance, the operator may gauge success by witnessing the loss of the waist at the esophagogastric junction. A 30 mm balloon is used initially. A 35 mm balloon is used if an adequate dilatation is not achieved or in subsequent dilatations if symptoms recur. A 40 mm balloon is rarely employed due to a higher risk of perforation.
Advantages
PD is performed routinely as an outpatient procedure, as opposed to LHM and POEM. In addition, it may be suitable for frail patients, as a palliative treatment to improve nutrition, or as a bridge to LHM or POEM. 23
Disadvantages
The esophageal perforation rate is negligible in expert hands with modern equipment. 24 GER is a drawback for PD and may affect up to 30% of patients. 16 Intuitively, a successful PD induces more reflux through the esophagogastric junction. Typically, more than a quarter of patients will require more than one PD to achieve symptomatic control. 16
Current outcomes
Early results are good for PD and are comparable to LHM; however, a decrease in efficacy is noted over time. A meta-analysis showed symptomatic relief in 85% of patients at 1 month and declined to 68% at 12 months and to 58% at 18 months. 3
Two prospective trials comparing surgery versus dilatation were recently published, including long-term results. The Swedish trial 25 reported the outcomes at 5 years of 36 patients who had PD as compared with 25 who underwent LHM and Toupet fundoplication. Symptom relief was better after an LHM at short follow-up but was equal to PD at 5 years. However, the failure rate that included recurrence of symptoms after three treatments or before 3 months, complications, or the patient's or physician's desire to change therapy was 36% for PD versus 8% for an LHM. The European trial 4 followed 192 patients for 6 years. The success rates for dysphagia relief were 94% for surgery and 90% for PD after 1 year, 89% and 86% after 2 years, and 84% and 82% after 5 years of follow-up. PD, however, required multiple sessions in a quarter of the patients.
Other meta-analyses compared LHM with balloon dilatation, with consistent results favoring surgery, especially at long follow-up.3,26–29
Per Oral Endoscopic Myotomy
Although the idea of performing a Heller myotomy via endoscopy dates from the 1980s, 30 the procedure has gained popularity only recently.
Current technique
The technique involves a 2–3 cm esophageal mucosotomy 10–15 cm proximal to the esophagogastric junction at the right-anterior orientation (2 o' clock position). A submucosal tunnel is created caudally 2–3 cm onto the stomach. The circular muscle layer is divided starting 2 cm below the lower border of the mucosotomy. At the end of the procedure, the mucosal entry site is closed with endoscopic clips. 31 Although the majority of authors perform a circular myotomy only, a complete myotomy of both longitudinal and muscular layers (full-thickness myotomy) reduces operative time, with similar short-term outcomes and complication rates.32,33
Alternatively, a full-thickness myotomy may be performed along the posterior esophageal wall, with the patient in supine position. Prophylactic antibiotics are administered before the procedure. A high-definition, forward-viewing gastroscope with a plastic cap is used with CO2 insufflation. The electrosurgical dissection is accomplished with a HybridKnife Type T™(Erbe, Tübongen, Germany), since the tool protrudes through the working channel in a posterior position. This view of the knife minimizes the risk of pleural injuries and identifies the impression of the spine on the esophagus to ensure a straight myotomy. Anterior endoscopic views require endoscope rotation that may cause sinuous myotomies and increase the risk of pleural and pericardial injury in case of full-thickness myotomies.
Advantages
POEM significantly reduces post-operative pain 34 and length of stay. 35
Disadvantages
According to a recent systematic review, complications occur in about 14% of patients. 36 Major bleeding may occur in up to 6% of the cases, air leak (pneumothorax, pneumoperitoneum, subcutaneous emphysema) occurs in up to 55% patients, and lung atelectasis occurs in 50% of the patients.33,37–39 These complications do not seem to affect the clinical status, since the rate of intensive care admission and conversion to surgery is minimal and mortality was not reported. 36 Adverse events are more common in small series during learning curves, and the largest series to date with 500 patients reports a complication rate of 3% only. 31
GER is also a concern after POEM, since an antireflux mechanism is not added to the myotomy. Postoperative GER symptoms may occur in up to 44% of the patients. 40 Objective measurement by pH monitoring shows an incidence of GER in one third of the patients (Table 2).
Previous experience with PD showed that post-procedure LES resting pressure is a strong predictor for a successful outcome, with <10 mmHg as a threshold. 46 Although different series report a significant decrease in the sphincter pressure after POEM, a basal pressure inferior to 10 mmHg is not achieved in most patients.31,33,41,42,44
Outcomes
POEM is a new procedure, and long-term results are accruing. In short-term follow-up, however, outcomes are excellent in experienced hands. 31 There are no meta-analysis or prospective trials comparing PD and POEM. POEM and LHM have been compared in a recent meta-analysis. The largest analysis encompassed 486 patients from 11 studies. 35 Follow-up was short (no more than 1 year), and no randomized trials were available. The incidence of postoperative GER symptoms favored LHM, but similar results were apparent for complications and dysphagia relief. Other meta-analyses showed no difference between the two techniques47,48 with regards to dysphagia or complications. 49
Conclusions
There are currently three valid options for the primary treatment of achalasia. Since each method has similar outcomes, inherent advantages and disadvantages must be considered for each patient. Ultimately, a multidisciplinary approach is useful to help decide the most appropriate treatment for each patient.
Footnotes
Authors' Contributions
F.A.M.H. and E.G.H.M.—acquisition of data, analysis and interpretation of data, drafting the article, and final approval of the version to be published. M.G.P.—conception and design, review for intellectual content, and final approval of the version to be published.
Disclosure Statement
No competing financial interests exist.