
Abstract
Abstract
Background:
Increased defecation frequency and soiling are common complications of surgery for right-sided Hirschsprung's disease (HD). Though the laparoscopic Duhamel procedure is a favorable option in right-sided HD, the conventional laparoscopic technique is time consuming and has complications that are associated with the reservoir. In this study, we described a modified laparoscopic Duhamel technique with ex-anal rectal transection combined with the Deloyer's procedure for right-sided HD.
Materials and Methods:
Between March 2010 and January 2015, 18 right-sided HD underwent this modified laparoscopic Duhamel procedure (MLDP). The main modifications were to mobilize the colon and to dissect the retrorectal space under laparoscopy, pull out, and transect ex-anally by using a linear stapling device through a transverse incision on posterior wall of the rectum. Seven age-matched patients who underwent a conventional laparoscopic Duhamel procedure (CLDP) between March 2008 and December 2010 were included as the control group. Demographics, surgical procedures, operative data, postoperative complications, and clinical outcomes were compared between these two groups.
Results:
Operative time was significantly shorter in the MLDP group (150 minutes versus 195 minutes; P = .03). There was no significant difference in mean timespan to obtain a normal defecation frequency (3.8 months versus 3.6 months), incidence of soiling (11.1% versus 14.3%; P = .34), and constipation (5.6% versus 14.3%; P = .69). Pouchitis were not found in the MLDP group, whereas 2 patients in the CLDP group (28.6%) presented with pouchitis and intractable diarrhea, requiring spur division. The incidence of postoperative enterocolitis was not significantly different in the two groups (11.1% in MLDP versus 14.3% in CLDP; P = .68). All 22 patients had a normal defecation over 4 years of age.
Conclusions:
Laparoscopic Duhamel with ex-anal rectal transection is a simple, easy-to-learn, and effective procedure for right-sided HD. It has low postoperative pouchitis because of a short pouch.
Introduction
H
In the surgical treatment of right-sided HD, increased defecation frequency, perianal skin erosion, and soiling are more frequently encountered.6,7 Several publications showed the Duhamel's advantages over the Swenson and Soave techniques, including less pelvic dissection, a larger anastomosis, and the formation of a reservoir, making it a favorable option to decrease defecation frequency and soiling in patients with right-sided HD.3,6,8–10 The major concern is that, if the reservoir is too long, it may cause pouchitis, constipation, or Hirschsprung's disease-associated enterocolitis (HAEC).3,9,10 With the introduction of minimally invasive surgery, classic open pull-through techniques were modified and improved with less pain and better cosmesis, but longer operative time and difficulty in manipulation of transection of the rectum in the laparoscopic-assisted Duhamel procedure hindered its application.3,8,10,11 We describe herein our experiences with the laparoscopic Duhamel procedure with ex-anal rectal transection combined with the Deloyer's procedure. The clinical outcomes of patients were compared with the conventional laparoscopic Duhamel procedure in the same center by the same surgical team.
Materials and Methods
From March 2010 to January 2015, 376 children with HD underwent laparoscopic-assisted pull-through surgery in our hospital. Fifty-nine (15.7%) of them were diagnosed as having long-segment HD. 12 Of those 59 cases, the transitional zone was located in hepatic flexure in 2 cases, in transverse colon in 11 cases, in splenic flexure in 5 cases, and in descending colon in 41 cases. A total of 18 children (10 boys, 8 girls) with right-sided HD underwent a modified laparoscopic Duhamel procedure (MLDP) combined with ex-anal rectal transection and colorectal anastomosis by using a linear stapling device. Seven of them underwent initial diverting ileostomy at the age between 18 days and 4 months because severe HAEC or abdominal distension was not alleviated by washouts. The definitive pull-through procedure was performed at the mean age of 7.0 ± 4.1 months (range 1.5–65 months). Between March 2008 and December 2010, 7 cases (4 boys, 3 girls), whose transitional zone was located in hepatic flexure in 2 cases, in transverse colon in 4 cases, and in splenic flexure in 1 case, were treated with conventional laparoscopic Duhamel procedure (CLDP) and used as the control group. Two of them underwent initial diverting ileostomy at the age of 28 and 65 days, respectively. The definitive pull-through procedure was performed at the mean age of 6.4 ± 3.9 months (range 1.8–72 months). All the surgeries were performed by the same surgical group. Confirmed diagnosis of HD was established by anorectal manometry, rectal suction biopsy, and postoperative pathological investigation. Resection level of the colon was determined based on the barium enema and intraoperative frozen biopsy. Our research was approved by the ethics committee of Union Hospital, Tongji Medical College, Huazhong University of Science and Technology.
Surgical technique for modified laparoscopic Duhamel pull-through
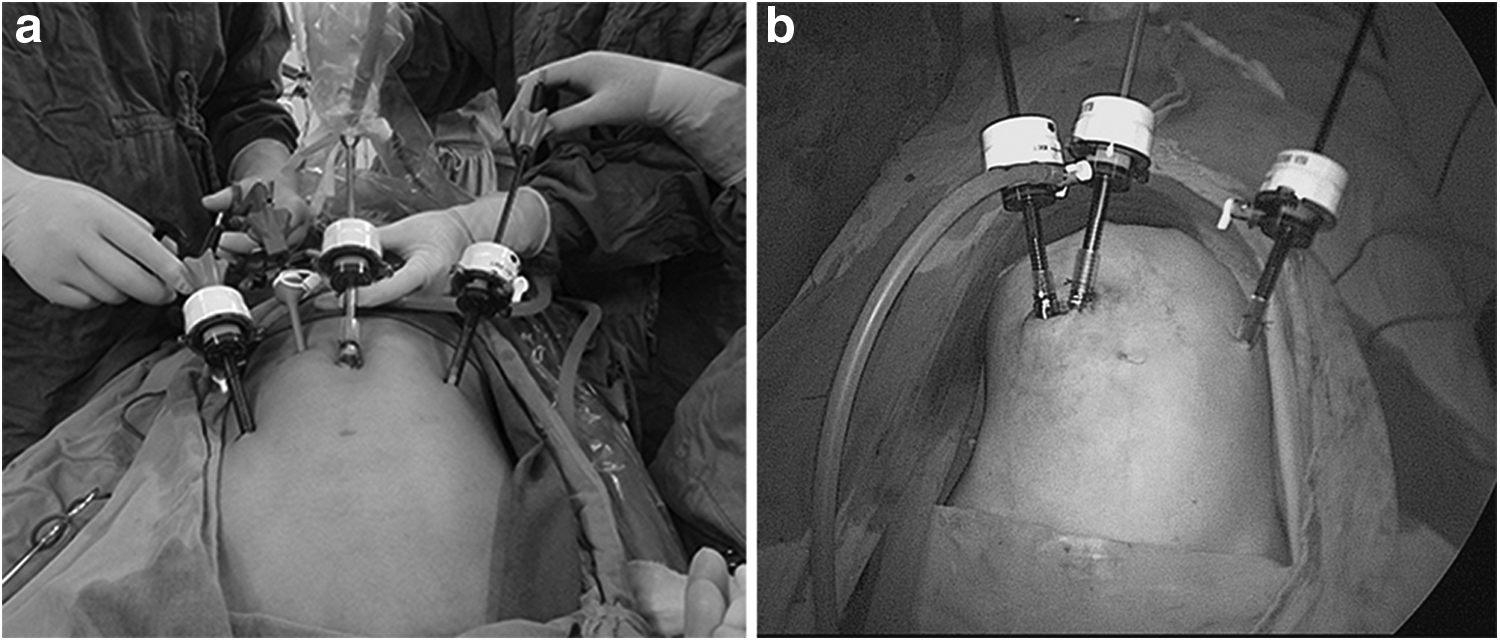
The laparoscopic technique was performed by using four ports (three 5 mm trocar and one 3 mm trocar) (Fig. 1a). For the patients with colostomy, we separated the stoma, mobilized and removed partial colon through abdominal opening, and finally used this abdominal opening to place two 5 mm trocars as working ports. The third 3 mm or 5 mm trocar was inserted in the left upper quadrant for a traction forceps (Fig. 1b). After the resection level was confirmed, the transverse, descending, ascending, and sigmoid colon were mobilized by using the ultrasonic scalpel, preserving the ascending branch of the right colic artery. Intrapelvic dissection was continued in retrorectal space to the level just above the dentate line. By using the Deloyer's maneuver, the colon was transpositioned 180° anticlockwise followed by concurrent appendectomy.
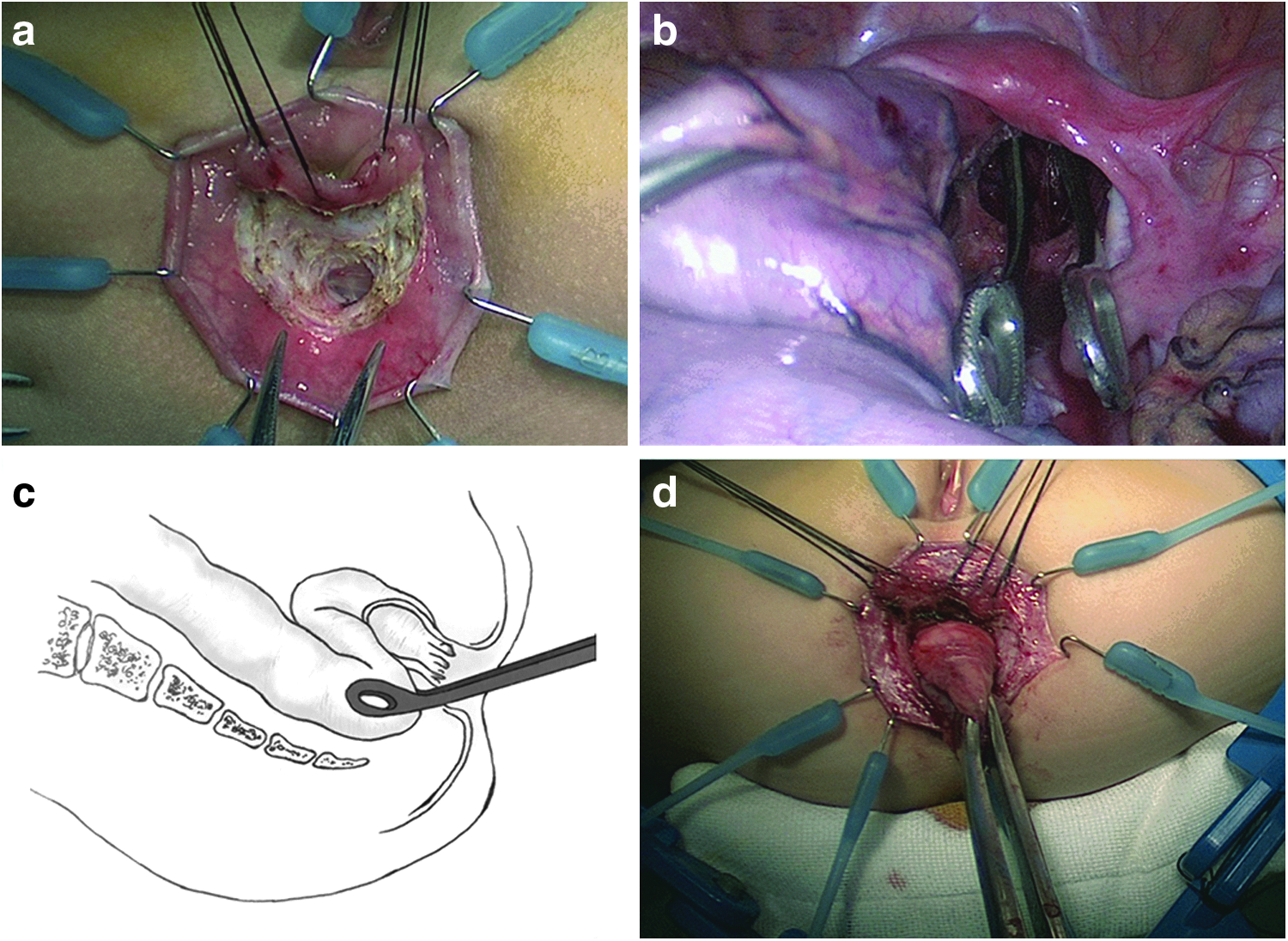
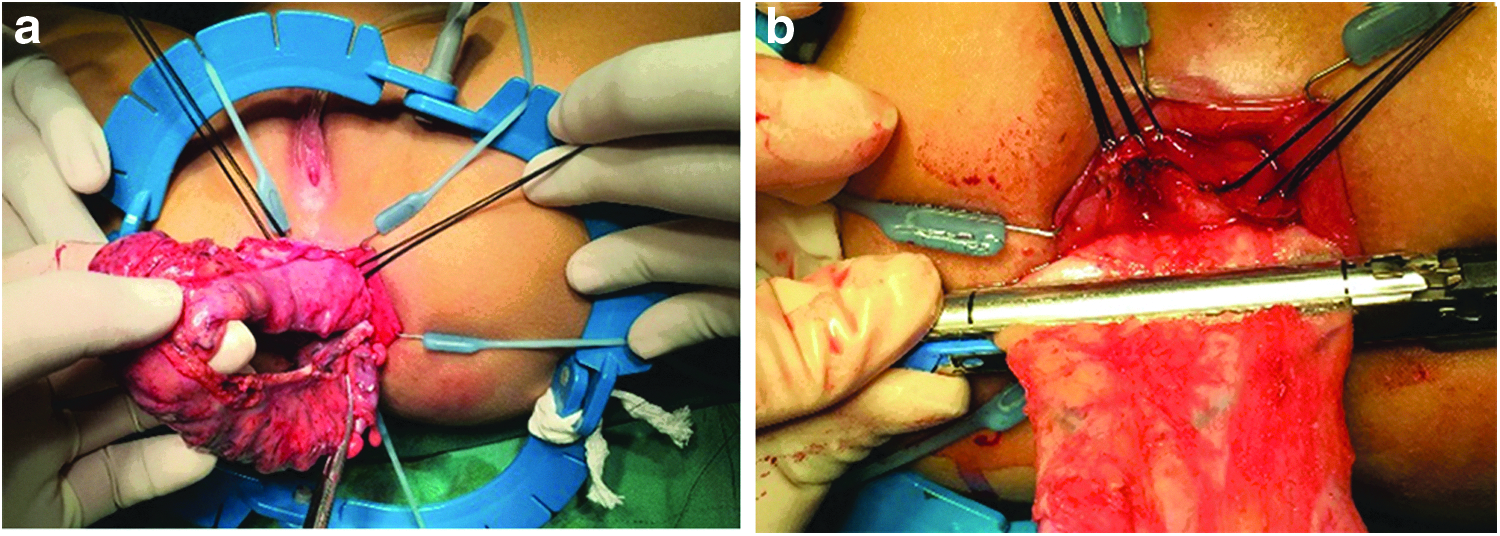
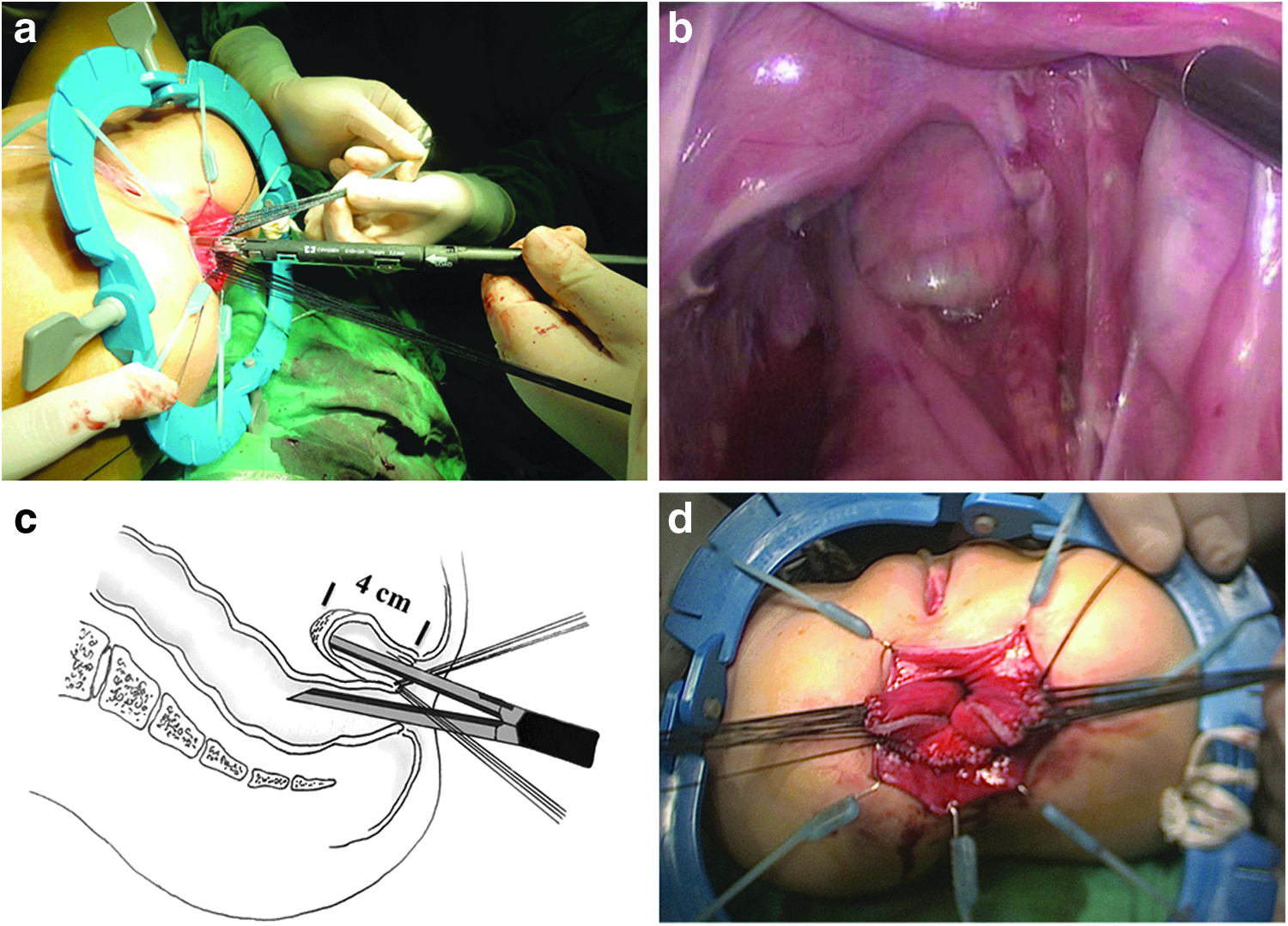
A Lone Star retractor (Lone Star Medical Products, Stafford, TX) was used to expose the anus. A full-thickness hemi-circumferential incision (1.5–2.0 cm) was made by using cautery in the inner posterior wall of the rectum 1 cm above the dentate line. Retrorectal dissection was performed by using Kelly forceps extending upward to create a retrorectal tunnel. A tissue-grasping forceps was subsequently introduced through the endorectal incision into the pelvic cavity (Fig. 2). Under laparoscopic visualization, the mobilized colon was grasped and pulled down through the retrorectal tunnel, facilitating extra-anal division of the rectum perpendicular to the anus by using Endo-GIA (Covidien, Mansfield, MA), to obtain a short 3.5–4.5 cm rectal stump (Fig. 3). We carefully pulled out the colon under the laparoscope to prevent bowel torsion, whereas only 12–15 cm of the ascending colon would be retained. The colorectal end-to-side anastomosis was completed between the pulled-through ascending colon and the posterior wall of the aganglionic rectum by using single-layer 4-0 Vicryl interrupted sutures. The side-to-side colorectal stapled anastomosis was completed by using Endo-GIA Stapler: One jaw of the stapler was put into the lumen of the native rectum up to the apex of the blind rectum stump, and the other one was put into the lumen of the pulled-down colon. Routinely, one cartridge (60 mm in length) was triggered while pulling the retracting sutures outward (insert-retracting technique) under laparoscopic view to maximize the septum resection (Fig. 4). Before retrieving the trocar, we observed again laparoscopically to make sure that the pull-through bowel had the right orientation. A rectal tube was inserted above the anastomosis level and remained for 3–5 days for decompression.
Surgical technique for conventional laparoscopic Duhamel pull-through
The operative technique was similar to that previously described. 13 Three 5 mm ports and one 12 mm port (right lower quadrant) were used to dissect the transverse, descending, ascending, and sigmoid colon. Under a laparoscope, retrorectal space was created and intra-abdominal transection of the rectum was achieved with a rectal stump of 5.0–6.0 cm. After the ganglionic colon was pulled through, the aganglionic rectum was anastomosed to the ganglionic ascending colon in the same fashion as described earlier. The colorectal spur was divided by Endo-GIA Stapler through the anus. Usually, one or two cartridges (60 mm in length) were triggered.
Postoperative management
Intravenous antibiotics were given in the first 72 hours, and the urinary catheter was removed after the first 24–48 hours postoperatively. Patients were fed orally when bowel sounds resumed, and they were discharged when they were clinically stable. A digital rectal examination was performed on an obligatory follow-up 4 weeks after the operation for each patient. Soiling is defined as involuntary leaking of small amounts of stool or liquid. In our study, the diagnostic criteria of soiling are defined as suffering from soiling once or more per week for at least 1 month. HAEC was defined as the presence of abdominal distention, diarrhea, vomiting, and fever. Constipation was defined as the voluntary bowel movement two or fewer times per week for at least 2 weeks. A normal defecation was defined as regular bowel movements, without soiling, and with 1–3 times per day or a time per 1–2 days. Surgical process, intra- and post-operative complications, and functional outcome of defecation were evaluated.
Results
The operation was completed laparoscopically for all patients with no conversion to open procedure. Of these 25 patients, there were no statistically significant differences in patient demographics between MLDP and CLDP groups, including age, body weight at surgery, and the transition zone location. There were no intraoperative complications in either group. Mean blood loss and mean length of hospital stay were not significantly different in the two groups; no transfusions were required. The mean operative time in MLDP was shorter than the one in CLDP (150 minutes versus 195 minutes, P = .03) (Table 1). The mean follow-up period was 42 months (range 12–58 months) in MLDP and 59 months (range 49–70 months) in CLDP. There was no statistically significant difference between the two groups in the frequency of bowel movement. Severe perianal erosion, anastomotic stricture, pelvic infection, fecaloma formation, or pouchitis was not found in any of these patients in MLDP, whereas there were 2 patients in CLDP (28.6%) who presented with pouchitis and intractable diarrhea, requiring spur division. Five patients had mild or moderate perianal erosion in the MLDP group; 1 patient with mild and 1 patient with moderate perianal erosion were noticed in the CLDP group (Table 2).
CLDP, conventional laparoscopic Duhamel procedure; MLDP, modified laparoscopic Duhamel procedure; N/A, not applicable.
CLDP, conventional laparoscopic Duhamel procedure; MLDP, modified laparoscopic Duhamel procedure; N/A, not applicable.
Three patients received regular anal dilation after surgery (2 in MLDP and 1 in CLDP). The mean timespan to obtain an acceptable defecation frequency is 3.8 months (range 2.2–6.3 months) in the MLDP group and 3.6 months (range 2.1–6.0 months) in the CLDP group, respectively. Two patients were readmitted postoperatively for HAEC at 5 months and 17 months, respectively, in the MLDP group. One patient was readmitted for HAEC at 8 months after surgery in the CLDP group (P = .68). The patients were managed successfully by conservative treatment. Two patients experienced episodes of postoperative constipation (1 in the MLDP group and another in the CLDP group, from 10–19 months to 9–17 months postoperatively, respectively; P = .69); a laxative or enema was effective in them. Soiling was seen in 2 patients in the MLDP group and in 1 patient in the CLDP group (P = .68), with a steady improvement of continence in the second year after surgery (Table 2). All 22 patients who were older than 4 years had a normal defecation control.
Discussion
Despite the fact that the transanal endorectal pull-through is becoming more popular in recent years for the treatment of HD, Duhamel techniques that may decrease defecation frequency and soiling occurrence, in both open and laparoscopic forms, still remain to be a good choice, particularly for patients with long-segment HD and total colonic aganglinosis. 6 As early as 1994, the laparoscopic technique was implemented in the Duhamel pull-through procedure by Smith et al. 13 Since then, several laparoscopic-assisted Duhamel-type operations have been described to reduce pain and improve cosmesis.14–16 However, the price to pay for these advantages is a longer operative time and an increased need for further surgery due to the division of rectal spurs.11,15–17 We have described herein our initial experiences with the laparoscopic-assisted Duhamel pull-through technique with ex-anal rectal transection combined with the Deloyer's procedure for the treatment of right-sided HD. The results have shown that this modified laparoscopic-assisted Duhamel technique is an effective procedure with a shorter operative time and fewer reservoir-associated postoperative complications.
The conventional laparoscopic-assisted Duhamel procedure usually requires a larger transabdominal port (12 mm)14,17 for the rectal transection by using an endoscopic stapler. However, laparoscopically it is difficult for proper transection of the rectum in the deep pelvis, possibly resulting in a long rectal pouch and a residual colorectal septum, which may cause pouchitis after surgery.3,9,10,18 In this series, there were 2, out of a total of 7, patients who complained of pouchitis in the CLDP group, whereas there were none in the MLDP group with our “ex-anal” transection.
According to previous publications,10,16,19 a short pouch or a completely divided septum is associated with better fecal control, lower incidence of pouchitis and HAEC. To achieve this, Nah et al. 16 have reported the laparoscopic Duhamel procedure with eversion of the rectum. Lamas-Pinheiro et al. 9 have reported the application of the curved Endo-GIA Stapler to obtain a low rectal transection via the retrorectal orifice under laparoscopic guidance. However, difficulty in completing the low resection of the rectum still remains in infants. Recently, Urushihara et al. 10 have described their excellent experiences with laparoscopic Z-shaped colorectal side-to-side anastomosis. In that procedure, the proximal rectum is pulled down through the incision in the posterior rectum and extracorporeally transected, and then the colorectal septum is completely divided without a blind pouch by using Endo-GIA through the anus under laparoscopic vision, followed by intracorporeal interrupted sutures under a laparoscope. It requires the skilled intracorporeal suturing technique and is challenging for the majority of pediatric surgeons. Meanwhile, it still bears the risk of pelvic infections caused by fecal contamination.
We simplified the technique reported by Urushihara and preserved a short pouch of 3.5–4.5 cm. The main advantages in our technique described here are two aspects: intraoperative technical advantage and postoperative functional benefits. Technically, pulling the rectum downward and performing ex-anal rectal transection near the anus allows the creation of a shorter rectal pouch even compared with Urushihara's technique. In the patients with colostomy, after detaching the stoma from the abdominal wall, we further mobilized the neighboring colon through the abdominal opening, which facilitated the laparoscopic mobilization of the remaining colon afterward and actually turned laparoscopic subtotal colectomy into laparoscopic left-side colectomy. Our modified techniques were less complex as the mean operative time was shorter than that of the control group and that of other reported procedures (245 minutes by Scholfield and Ram, 3 296 minutes by Urushihara et al. 10 ). Though we did not completely obliterate the colorectal spur as a Z-shaped modified technique, we managed to make it extremely short by the “insert-retracting technique.” The septum was so short that it could be easily missed out on a digital rectum examination. Postoperatively, our technique avoided the potential infection otherwise caused by transection and suturing of the rectum in the abdomen cavity. Meanwhile, symptoms due to remnant septum with subsequent pouchitis or fecaloma formation in the rectal ampulla were not found in the MLDP group during an average follow-up time of 42 months.
Three patients who needed regular anal dilation after surgery were infants (range 1.5–2.6 months), and they had a small diameter of anastomosis after surgery because of their smaller-sized intestine. Except for them, according to the digital rectal examination performed on an obligatory follow-up 4 weeks postoperatively, all other patients did not receive regular anal dilation, and anastomosis stenosis was not observed during the follow-up, probably benefiting from the larger anastomosis diameter of the Duhamel procedure.
Lower incidence of postoperative HAEC can be seen in the MLDP group, and the incidences in the two groups meet with a reported incidence of 5%–46% from previous studies.20,21 Although it seems that there is no statistically significant difference between the two groups (11.1% versus 14.3%, P = .68), it may be because of the small size of the sample in our study. The short rectal pouch without ganglion cells may be the reason for the decreased incidence of postoperative enterocolitis in the MLDP group; a large sample study will be necessary to confirm our inference in the future. As previously described, the incidence of constipation could be as high as 7%–81% after the Duhamel operation for recto-sigmoid HD.3,10 Two factors could account for the low incidence of constipation (5.6%) in this series. First, for right-sided HD who received extensive colectomy, only 12–15 cm of the colon is retained, which leads to a short residing time of the stool in the gut, causing more frequent defecation. Second, patients can sense the fullness and the urge to defecate accurately by the remaining rectal wall of the short rectal pouch. We previously reported that bowel movement can reach a maximum of 1–3 times per day after 6 months to 1 year for most patients who received the laparoscopic-assisted Soave procedure with extensive colectomy. 22 This study showed quicker recovery of fecal frequency (3.8 months after surgery) for right-sided HD, and this is due to less pelvic dissection and the formation of a reservoir from the laparoscopic Duhamel technique. Two (11.1%) of the patients in the MLDP group and 1 (14.3%) of the patients in the CLDP group experienced postoperative soiling and it decreased significantly 1 year later, which compares well with a reported incidence from previous studies 18 The magnification in laparoscopy allows clearer visualization and more precise dissection, minimizing trauma to nerves and sphincter, 3 better visualization may also allow for a shorter rectal pouch, and these contributory factors have been shown to reduce soiling after the Duhamel procedure. The other factors that can cause increase in soiling are manipulation and stretching of the sphincter and the length of the aganglionic segment. 18 Thus, our results may be influenced by synthetic factors. Recent literature demonstrated 18 that the laparoscopic-assisted Duhamel pull-through had the lowest soiling rate (15.1%), but the highest constipation rate (67%) compared with laparoscopic-assisted Swenson and Soave pull-through for left-sided HD. Our results showed that application of modified laparoscopic-assisted Duhamel pull-through with a short rectal pouch in right-sided HD can achieve adequate balance between constipation and soiling in the early stage after surgery.
For the 6 patients whose transitional zone was located at spleen flexure in two groups, the colon had to be mobilized and transected at least up to 10–20 cm above the transitional zone to allow a pull-through with “near-normal” colon for subsequent colorectal anastomosis. We noticed that irrigation in long-segment HD cannot be as effective as in short-segment HD and there are various degrees of dysmotility and hypertrophy in the proximal colon of the transitional zone according to a pathological review of our patients' samples. Similar to Georgeson's point of view, 7 we believe that although ganglion cells exist in the transitional colon, it might be abnormal in morphology or function, 23 removal of this part may be more beneficial for the low incidence of HAEC and recurrent constipation.24,25 In those patients with the transitional zone at splenic flexure, it means removing part of the left-side transverse colon to reach the “near-normal” colon. In that case, it is impossible for a well-vascularized and tension-free colorectal anastomosis without Deloyer's procedure due to the long distance between the remaining colon and the anus after a direct pull-down,26,27 which the reported technique 28 by taking down the proximal colon through an avascular window of the ileal mesentery for anastomosis requires an intact transverse colon and may still cause jejunal loop obstruction.
In conclusion, our results showed that the laparoscopic-assisted Duhamel procedure with ex-anal rectal transection combined with Deloyer's procedure is a simple, easy-to-learn, and effective procedure for right-sided HD with a low incidence of postoperative pouchitis. A large sample and long-term follow-up are necessary to evaluate the outcome of this modified procedure.
Footnotes
Acknowledgment
This study was supported by the Public Welfare Research, and special funds were received from the National Health and Family Planning of China (Grant No. 201402007).
Disclosure Statement
No competing financial interests exist.