
Abstract
Abstract
Introduction:
Recently, robotic-assisted thymectomy (RAT) has emerged as an alternative to either, an open transsternal approach or to a video-assisted thoracoscopic approach, for both thymic tumors and benign lesions. We have reviewed our early experience with RAT to assess the associated learning curve as well as the short-term perioperative outcomes.
Methods:
A prospectively collected database was reviewed for patients who underwent RAT for all causes in the period 2012–2016. Robotic thymectomy cases were stratified and compared according to the number of cases performed by each surgeon (≤15 versus >15 cases). A propensity score matching was done to compare perioperative outcomes in patients undergoing robotic and transsternal resection of thymomas.
Results:
Seventy patients (47 females) with a median age of 52, underwent RAT. The median operative time was 102 min with 5 conversions to an open approach for local invasion (n = 3) or for complete pleural symphysis (n = 2). There were 2 rib fractures and 1 recurrent laryngeal nerve palsy. Median length of chest tube drainage and length of stay were 1 and 3 days, respectively. Operative time and estimated blood loss plateaued after surgeon's initial 15–20 cases, which may reflect the initial learning curve. A comparison between early and late robotic cases showed that with the growing experience, the operative time becomes shorter (94 versus 107 min, P = .018). Propensity score analysis between robotic and transsternal resection of thymoma (n = 22 in each group) showed no significant differences in operative time (P = .79), intraoperative complications (P = .99), or postoperative complications (P = .99).
Conclusions:
Robotic thymectomy is feasible and safe, and is associated with comparable perioperative outcomes to the traditional transsternal approach in patients undergoing thymomectomy. An initial learning curve of 15–20 robotic thymectomy cases may be required by the surgeons to adequately perform this relatively novel technique.
Introduction
T
The RAT approach has significant potential advantages for surgeons. The high-definition three-dimensional vision alongside the enhanced instrument articulation provided by the robotic surgical system (Intuitive Surgical, Inc., Mountain View, CA) further enables a surgeon to explore the anterior mediastinum. Also, CO2 insufflation through a complete portal approach opens up this confined space and allows for bilateral phrenic nerve visualization and bilateral thymic horn dissection, well into the cervical region.
Despite the increased interest in RAT, there is a paucity of clinical data describing the learning curve associated with this approach. This study reports a single institution's initial experience of 70 consecutive robotic-assisted thymectomies performed over a 4-year period. It also assesses the learning curve associated with robotic thymectomy and compares the perioperative outcomes in propensity matched groups of patients undergoing robotic and transsternal resection of thymoma.
Patients and Methods
Study design and patients
A retrospective review of a prospectively collected thoracic surgery database was performed for patients who underwent RAT at New York Presbyterian Hospital, Weill Cornell Medical College in the period January 2012–August 2016. Patients were included in the study based on intention-to-treat analysis. Demographic, operative, and postoperative data were collected and analyzed.
Robotic thymectomy cases were stratified into two groups according to the number of cases done by each surgeon. To determine the cutoff number of cases that defines the two groups, we plotted the operative time and estimated blood loss (EBL) against surgeons' experience and the plateau point was observed after 15–20 initial cases. The two groups (early 15 cases versus late 15 cases) were compared to assess the effect of the cumulative surgeons' experiences on the perioperative outcomes.
Furthermore, comparison of the demographics and clinical, pathologic, and perioperative outcomes between propensity score-matched groups of patients undergoing robotic and transsternal resection of thymoma was done (n = 22 in each group). Due to the small number of transsternal thymectomies done during the study period, the balanced group was selected from cases done before and during the study period (2004–2016). Propensity matching included the following variables: age (≥52 versus < 52 years “median age of the whole cohort”), gender, pathologic size of tumor (≤5 versus > 5 cm), Masaoka-Koga stage (I/II versus III/IV), and World Health Organization (WHO)-Histologic subtypes (B3/C versus others). Propensity scores were calculated by logistic regression modeling. Matching was done one to one with the use of the nearest neighbor methods without replacement by using 0.2 caliper width.
Procedure time was defined as the time from port-site skin incision till skin closure. Postoperative hospital stay was calculated from the day of surgery until discharge from the hospital. Operative mortality was defined as death within 30 days of surgery or during the same hospital stay. Histopathological typing of thymomas was performed using the WHO classification (3rd edition), and pathological staging was done using the Masaoka-Koga system. Categorical variables were expressed as numbers (percentage) and were compared using Chi-Square or Fischer's exact tests. Continuous variables were expressed as median (interquartile range) and were compared using Mann–Whitney U-test. Data analysis was performed using IBM SPSS software (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0; IBM Corp., Armonk, NY) and PS-matching package version 3.04.
Anesthetic consideration, surgical technique, and postoperative management of robotic thymectomy cases
All patients were operated on with a double-lumen endotracheal tube as well as with appropriate hemodynamic monitoring, including an arterial line. Patients were placed in the supine position with a bolster to elevate the operative side 30°. Laterality was chosen based on the predominant side of the lesion or usually right sided for nonthymomatous myasthenia gravis cases. A three- to four-port technique was utilized with 8 mm ports placed in the 2nd, 4th, and 6th intercostal spaces at the anterior axillary line. CO2 is insufflated (Surgiquest) and limited to 10 mmHg. All patients included in this study underwent extended thymectomy regardless of the pathology. An extended thymectomy is performed in a caudal to cephalad direction, beginning with resection of the pericardial fat and mediastinal tissue off the diaphragm. The right phrenic nerve is then identified and skeletonized throughout its course up to the cervical region. Similarly, on the left side, dissection is performed along phrenic nerve dissecting the thymic tissue in the aortopulmonary (AP) window up to the level of the innominate vein. Branches of thymic veins are then taken with hemoclips or harmonic scalpel.
The thymectomy is completed by delivering the cervical horns from the right and left side, and the specimen is removed through the inferior robotic port using a surgical specimen bag (EndoCatch, Ethicon). Commonly, this port will be enlarged for large thymic neoplasms. A single 28F soft drain (Blake) is placed for pleural drainage. Patients are routinely extubated in the operating room (OR) and their drains removed on the first postoperative day (POD). We aim for discharge on the second POD.
Results
In the period (2012–2016), we performed 89 thymectomies; of them, partial sternal split/sternotomy was used in 12 patients (13%), VATS was used in 7 cases (8%), and 70 cases (79%) were done using the surgical robotic system and were included in this study [median age 52 years (34–61), 47 females]. Patients who underwent partial sternal split/sternotomy in the study period had prior sternotomy, large mass on computed tomography (CT) (>8 cm), and/or invasion/encasement of major vascular structures. However, the majority of VATS cases (n = 5) were done in the first 2 years of the study when robotic approach was not yet well established in our institution. The other 2 cases were done more recently due to surgeon's preference. The demographic and clinical characteristics of patients undergoing thymectomy during the study period are listed in Table 1.
NA, not applicable; VATS, video-assisted thoracoscopic.
Indications for surgery in patients undergoing robotic thymectomy were as follows: myasthenia gravis (19 patients, 27%), mediastinal mass in myasthenia gravis patients (10 patients, 14%), or an enlarged mediastinal mass without myasthenia gravis (41 patients, 59%). The right-sided approach was utilized in 42 patients (60%). The median operative time was 102 min (77–125) with a median EBL of 20 mL (20–50). There were 2 rib fractures and 1 recurrent laryngeal nerve palsy. A conversion to an open approach occurred in 5 patients (7%) due to dense adhesions (n = 2), or involvement of aorta/innominate vein (n = 3).
Sixty-eight patients (97%) were extubated in the OR. Two myasthenia gravis patients were extubated in the postoperative care unit. The median duration of chest drainage was 1 day (1–1). The median length of hospital stay was 3 days (2–4), with 32 patients (46%) discharged within 2 days of the surgery. A postoperative complication occurred in 8 patients (11%); 3 patients had myasthenic crisis, 3 patients had postoperative pneumonia, and 2 patients had prolonged air leak. There were no operative/30-day mortalities.
Histopathological analysis of the resected specimens showed that 33 patients (47%) had thymic tumors; 28 patients had a thymic epithelial neoplasm, 3 had a mature cystic teratoma, 1 patient had a thymolipoma, and 1 patient had thymic amyloid tumor. The remaining 37 patients (53%) had thymic hyperplasia (n = 21), benign cyst (n = 8), and normal thymic tissue (n = 8).
Of the 28 patients who had robotic resection of thymic epithelial neoplasm, 6 patients (21%) had Masaoka-Koga stage I, 17 patients (61%) had stage II, 4 patients (14%) has stage III, and 1 patient (4%) had stage IVA. Eight patients (29%) had WHO type A/AB, 16 patients (57%) had WHO type B, 3 patients (11%) had a thymic carcinoma (2 cases stage IIA, 1 case stage III that was converted to open approach), and 1 patient (3%) had an infarcted thymoma for which the WHO type could not be identified.
The median tumor size was 5 cm (3–6.5), with the largest tumor resected being 9.5 cm. In this particular case, the preoperative CT scans showed a 7 cm anterior mediastinal mass in a patient presenting with myasthenia gravis. Resection was done using a left-sided approach following the same technical steps described in the Patients and Methods section, and final pathologic assessment showed a 9.5 cm, stage III, type B3 thymoma.
An R1 resection was found in 2 patients, both were stage III and had WHO type B3 and C. Complete resection was presumably achieved by robotic approach along with pericardial resection. The positive microscopic disease was related to the soft tissue surrounding the pericardial resection, which was managed by adjuvant radiation therapy. One of the 2 patients had a conversion to open approach. Whether using an open approach would have resulted in R0 resection in the other patient is questionable.
Robotic thymectomy cases included in this study were performed by 4 surgeons; of them, 2 surgeons performed more than 25 cases. Operative time and EBL were used as surrogates of technical proficiency. A plateau point was observed following surgeon's initial 15–20 cases (Fig. 1). Furthermore, robotic cases were stratified into two groups according to the number of cases done by each surgeon (early 15 cases versus late 15 cases). The late group had a shorter operative time (94 versus 107 min, P = .018), with increasing use of the left-sided approach (64% versus 27%, P = .002). There were no differences in EBL, intraoperative complications, conversion rate, postoperative complications, or length of stay (LOS) between the two groups (Table 2).
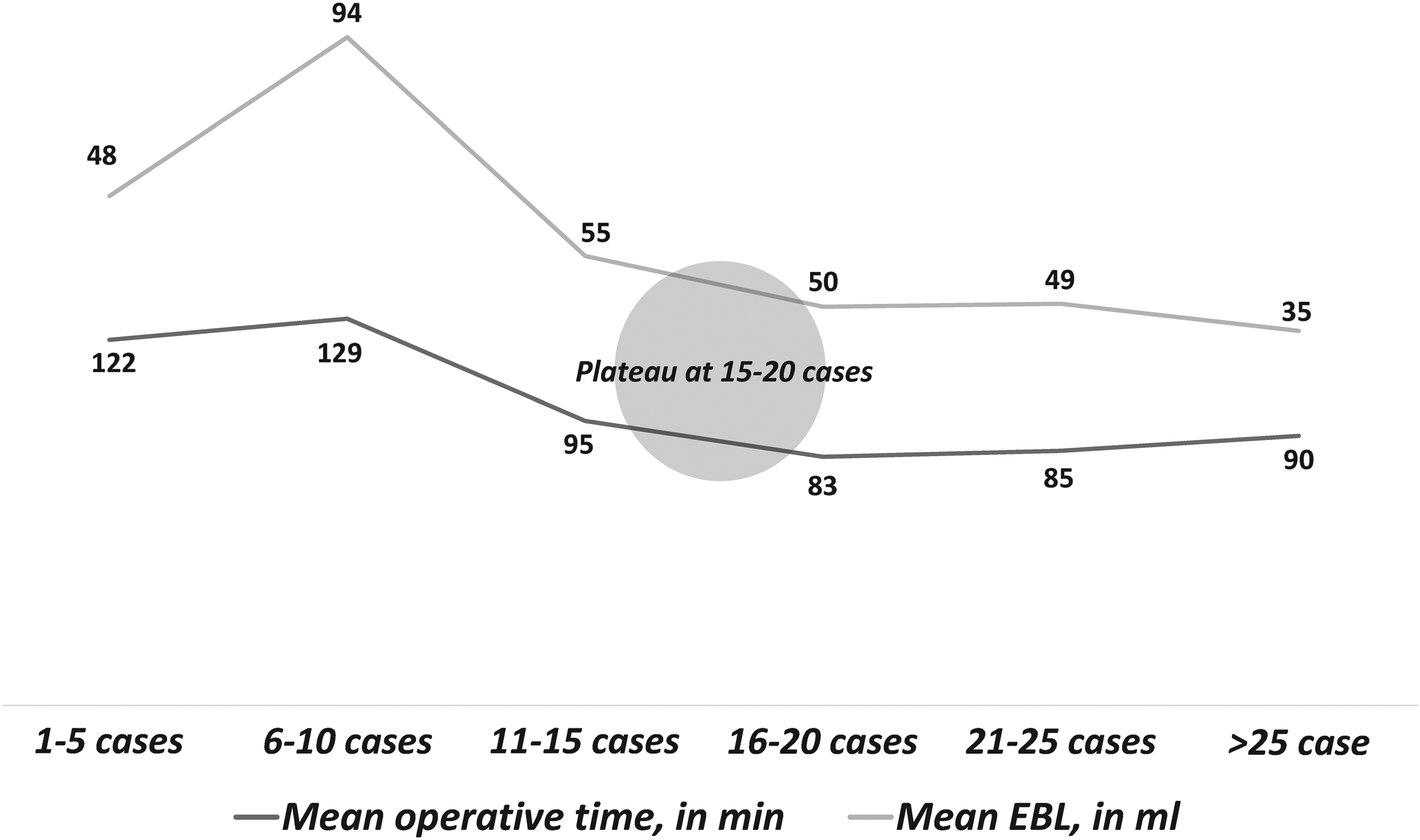
Learning curve associated with robotic thymectomy; operative time and EBL plotted against number of cases done by each surgeon. EBL, estimated blood loss.
P value calculated by Fischer's exact test.
EBL, estimated blood loss; LOS, length of stay.
Patients undergoing robotic thymectomy for thymomas were matched with a balanced cohort undergoing transsternal resection (n = 22 in each group). Patients were matched for age (P = .73), gender (P = .76), pathologic size of tumor (P = 1.00), Masaoka-Koga stage (P = .50), and WHO-Histologic subtypes (P = .71). There were no significant differences in operative time (P = .79), intraoperative complications (P = .99) or postoperative complications (P = .99) between the two groups. However, less EBL (50 versus 150 mL, P < .001), shorter chest drainage (1 versus 2 days, P < .001), and shorter LOS (2 versus 4 days, P = .010) were noted with the use of robotic approach compared to the transsternal approach (Table 3).
P value calculated by Fischer's exact test.
The remaining 2 cases had infarcted thymomas, for which histological type couldn't be identified.
EBL, estimated blood loss; LOS, length of stay; WHO, World Health Organization.
Comment
In 2001, Yoshino et al. published the first report of a robotic-assisted resection of a thymic tumor. 2 Since then, there has been a continued increase in the adoption of the RAT approach. It is estimated that more than 3500 cases have been performed in over 100 medical centers so far. 3 This study reports our institution's initial RAT experience with a good safety profile and low perioperative morbidity. Furthermore, this study spots the light on the learning curve and perioperative outcomes associated with robotic thymectomy.
Over three quarters of all thymectomies done in the study period were performed robotically. In selecting patients for a RAT approach, the only absolute contraindication was obvious locally advanced disease with questionable major vascular invasion. As our experience grew, patients with thymomas as large as 9.5 cm were included.
There are several points to be considered when contemplating a robotic approach. Once the robotic arms are docked, a patient's position cannot be changed, and it becomes rather difficult for the anesthesiologist to access the patient. Therefore, proper positioning, padding of pressure points, and field avoidance precautions must be adequately implemented before robotic docking. To avoid brachial plexus injury, proper axillary padding should be performed. Also, care must be taken not to hyperabduct the upward located arm (right arm in the right-sided approach), which sometimes may be tempting to the surgeon so as to make more room for the robotic arms. Furthermore, careful attention should be paid to properly place and position the robotic arms to allow for an optimum accessibility of planned resection anatomy and avoid robotic arm collision and patient injury. 4
In general, we prefer the right-sided approach, as it provides a larger operative field. However, a left-sided approach was utilized for left-sided dominant lesions. Interestingly, the left phrenic nerve and AP window can be accessed through a right-sided approach. If there is any concern in regard to left phrenic nerve identification, a separate 5 mm camera could be inserted into the left chest for assistance. However, in our experience, we were able to identify the left phrenic nerve without the need to use any extra ports. Regardless of the approach side, care must be exerted not to exert excess traction/compression on the heart or the great vessels to avoid possible arrhythmias and/or hypotension.
In this series, open conversion was required in 5 cases due to dense adhesions, suspected involvement of the phrenic nerve, or the caval/innominate junction (Table 1). No conversions were done for surgical complications or bleeding.
To date, most robotic series have demonstrated low perioperative morbidity rates (2%–11%) with no surgery-related mortalities. The most commonly reported intraoperative complications were bleeding either due to injury to the internal mammary vein or to one of the thymic venous branches draining into innominate vein. Also reported, have been phrenic nerve injury and recurrent laryngeal nerve injury. Pandey et al. reported a case of robotic thymectomy for myasthenia gravis, with intraoperative brachial plexus stretch injury resulting from a nonfavorable hyperabducted arm positioning as well as possible direct robotic arm impingement on the axillary region during the surgery. In addition, this study reports 2 cases of rib fracture due to torque from the robotic arm. Both cases occurred in our late experience. The ports' site and instruments used in the 2 cases were the same as we used in the other cases. Therefore, care must be exerted by surgeon, patient side assistant, and scrub nurse to avoid robotic arm pressure injury of the patients. Other less common complications have been reported and included pneumothorax, persistent air leak, desaturation, and chylothorax. However, the incidence of postthymectomy myasthenic crisis has tended to be low (0%–11%), compared to those previously mentioned with the open approach (12%–34%).3, 5–15
To our knowledge, this is the first study to assess the number of cases needed by each surgeon to adequately perform robotic thymectomy. We used the operative time and EBL as surrogates of technical adequacy and found that the learning curve consists of surgeon's initial 15–20 cases. Based on that number, we divided robotic thymectomy cases into two groups [initial 15 cases (n = 45) and late 15 cases (n = 25)]. With growing experience, operative time became significantly shorter. Although not statistically significant, the late group included resection of higher percentage of thymoma compared to other thymic pathologies (52% versus 33%), with higher percentage of more advanced stages (stage III/IVA: 23% versus 13%). Moreover, the 4 surgeons that performed the robotic cases had extensive prior experience in the minimally invasive thoracoscopic techniques. These together may explain the lack of differences in perioperative complications and conversion rates between early and late groups. The two intraoperative complications occurring in the late group were rib fracture by the torque of robotic arms as discussed earlier.
In concordance with previous reports that compared robotic and transsternal thymectomy, this study found no major differences in the perioperative outcomes in propensity-matched groups of patients undergoing resection of thymomas.16,17 It is worth mentioning that the robotic approach was associated with less EBL and shorter duration of chest drainage and LOS. Moreover, robotic approach allows for the exploration of the pleural cavity, particularly in large tumors where the incidence of pleural implantation is high. 18
Conclusions
This study represents a single institution's experience with robotic thymectomy. This study highlights the safety and efficiency of the robotic approach in the management of thymic diseases, including thymomas. An initial learning curve of 15–20 cases may be needed to attain technical proficiency. Future research should assess the long-term oncological and neurologic outcome of patients following robotic thymectomy.
Footnotes
Disclosure Statement
No competing financial interests exist.